Download as pdf or txt
You might also like
- Lotus Materia Medica by Robin Murphy 8131908593Document5 pagesLotus Materia Medica by Robin Murphy 8131908593Indhumathi33% (6)
- Chronic Kidney DiseaseDocument9 pagesChronic Kidney Diseaseluvgrace100% (1)
- The Principles and Art of Cure by Homoeopathy Herbert Alfred Roberts.01431 - PDFDocument6 pagesThe Principles and Art of Cure by Homoeopathy Herbert Alfred Roberts.01431 - PDFIndhumathi0% (2)
- Pahtophysiology of EsrdDocument5 pagesPahtophysiology of EsrdCarl JardelezaNo ratings yet
- A MabCaseStudyVersion PDFDocument278 pagesA MabCaseStudyVersion PDFviswanath856100% (1)
- Complications of Chronic Kidney Disease Current STDocument32 pagesComplications of Chronic Kidney Disease Current STmetaNo ratings yet
- Chronic Kidney DiseaseDocument17 pagesChronic Kidney Diseaseniken_rizkiNo ratings yet
- RationaleDocument7 pagesRationaleJohn Michael ClimacoNo ratings yet
- Dr. Sunatrio - Management Hypovolemic ShockDocument59 pagesDr. Sunatrio - Management Hypovolemic ShockArga Putra SaboeNo ratings yet
- Pulmonary ThromboembolismDocument61 pagesPulmonary ThromboembolismsanjivdasNo ratings yet
- Chronic Kidney DiseaseDocument33 pagesChronic Kidney DiseasesexiiimammaNo ratings yet
- A Case Study On Graves DiseaseDocument46 pagesA Case Study On Graves DiseaseRenie SerranoNo ratings yet
- What Is Hypertensive NephropathyDocument11 pagesWhat Is Hypertensive NephropathyIvy Pamanian DeldaNo ratings yet
- Rheumatic Heart DiseaseDocument30 pagesRheumatic Heart DiseasejustinahorroNo ratings yet
- Chronic Renal FailureDocument29 pagesChronic Renal Failuregeorgia.langNo ratings yet
- Heart Failure NCLEX QuestionsDocument5 pagesHeart Failure NCLEX QuestionsMelodia Turqueza GandezaNo ratings yet
- Activity IntoleranceDocument6 pagesActivity IntoleranceRaidis PangilinanNo ratings yet
- Pre Eclampsia EclampsiaDocument28 pagesPre Eclampsia Eclampsiachunna110No ratings yet
- Acute Glomerulonephritis (AGN) : Group A Beta Hemolytic StretococcusDocument3 pagesAcute Glomerulonephritis (AGN) : Group A Beta Hemolytic StretococcusKristine Danielle DejeloNo ratings yet
- Congestive Heart Failure OverviewDocument12 pagesCongestive Heart Failure OverviewkazelleNo ratings yet
- Case Study 2Document2 pagesCase Study 2CJ BagasNo ratings yet
- REVIEWERDocument12 pagesREVIEWERCynde KerrNo ratings yet
- Risk For Bleeding - Cirrhosis NCPDocument2 pagesRisk For Bleeding - Cirrhosis NCPPaula AbadNo ratings yet
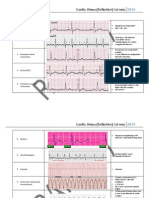
- Cardio QuizDocument100 pagesCardio QuizEvidence ChaibvaNo ratings yet
- Pulmonary EdemaDocument47 pagesPulmonary Edemamaeliszxc kimNo ratings yet
- ASSE Project Final ExamDocument7 pagesASSE Project Final ExamMycz DoñaNo ratings yet
- Presby Methotrexate Protocol For Ectopic PregnancyDocument3 pagesPresby Methotrexate Protocol For Ectopic PregnancyTrina JoyceNo ratings yet
- Drills-1 Np4 AquinoDocument11 pagesDrills-1 Np4 AquinoSolah SalvatoreNo ratings yet
- Renal Disorders Nursing Practice QuizDocument5 pagesRenal Disorders Nursing Practice QuizblaireNo ratings yet
- Integumentary Communicable DiseasesDocument4 pagesIntegumentary Communicable DiseasesFreeNursingNotesNo ratings yet
- QADocument11 pagesQAGladys FernandezNo ratings yet
- Chapter 23 P - Management of Patients With Chest and Lower Respiratory Tract DisordersDocument5 pagesChapter 23 P - Management of Patients With Chest and Lower Respiratory Tract DisordersMary SingletonNo ratings yet
- Test Quiz Hypo Kale MiaDocument6 pagesTest Quiz Hypo Kale MiaVivian Montesena BreganzaNo ratings yet
- What Is Acute Glomerulonephritis?: Acute Glomerulonephritis (GN) Comprises A Specific Set of Renal Diseases inDocument6 pagesWhat Is Acute Glomerulonephritis?: Acute Glomerulonephritis (GN) Comprises A Specific Set of Renal Diseases inAnnapoorna SHNo ratings yet
- Hirschsprung Disease Case Study ScenarioDocument2 pagesHirschsprung Disease Case Study ScenarioKrizzia Angela BacotocNo ratings yet
- Medical-Surgical Nursing Table of ContentsDocument2 pagesMedical-Surgical Nursing Table of Contentsɹǝʍdןnos0% (1)
- Metabolic and Endocrine ManagementDocument42 pagesMetabolic and Endocrine ManagementAlyssa MontimorNo ratings yet
- Gastro NotesDocument24 pagesGastro NotesMicah EllaNo ratings yet
- Case Study (Pleural Effusion)Document4 pagesCase Study (Pleural Effusion)Jvspapa ShilohNo ratings yet
- Nursing Diagnosis For Lower Respiratory DiseasesDocument5 pagesNursing Diagnosis For Lower Respiratory Diseasesngoto8867% (3)
- Activity 3 Case Scenario GcsDocument3 pagesActivity 3 Case Scenario GcsDfatsbsNo ratings yet
- 50 Item Psychiatric Nursing ExamDocument8 pages50 Item Psychiatric Nursing Examalexis_borjNo ratings yet
- Research and ManagementDocument9 pagesResearch and ManagementMa Charmaine Dawn VillaruelNo ratings yet
- NCM116 Module 3 Cerebrovascular Disease QuizDocument5 pagesNCM116 Module 3 Cerebrovascular Disease QuizIvan FernandezNo ratings yet
- Hematologic ManagementDocument17 pagesHematologic ManagementAlyssa MontimorNo ratings yet
- Acute Renal FailureDocument9 pagesAcute Renal FailureananNo ratings yet
- Gastrointestinal System - QUIZDocument4 pagesGastrointestinal System - QUIZsidejbeeNo ratings yet
- Professional AdjustmentDocument3 pagesProfessional Adjustmentkamae_27No ratings yet
- Chronic Renal FailureDocument28 pagesChronic Renal FailurePatricia Nadine Sarcadio NeffeNo ratings yet
- Cardio and Hema Super SamplexDocument24 pagesCardio and Hema Super SamplexMj Lina TiamzonNo ratings yet
- The Community Health Nursing and Communicable DiseasesDocument40 pagesThe Community Health Nursing and Communicable DiseasesericNo ratings yet
- Crestor (Rosuvastatin Calcium) : Abbreviations Abbrev Definitions Dictionary ICD9 Codes Equipment Hospitals Drugs More.Document2 pagesCrestor (Rosuvastatin Calcium) : Abbreviations Abbrev Definitions Dictionary ICD9 Codes Equipment Hospitals Drugs More.Aidi RahmanNo ratings yet
- Endo GI Extra QuestionsDocument3 pagesEndo GI Extra QuestionsToni Marie Buenconsejo PunzalanNo ratings yet
- Maternal and Child Health Nursing 1 Saundrs Pink EdDocument149 pagesMaternal and Child Health Nursing 1 Saundrs Pink EdVin SantosNo ratings yet
- Capstone Case Study Final - CHFDocument3 pagesCapstone Case Study Final - CHFapi-351999622No ratings yet
- Overview of Neonatal Respiratory Distress - Disorders of TransitionDocument14 pagesOverview of Neonatal Respiratory Distress - Disorders of TransitionAlfredo Junior Delgado PeláezNo ratings yet
- Pediatric Nursing - QuizDocument13 pagesPediatric Nursing - QuizChy ChyNo ratings yet
- Epiglottitis PDFDocument5 pagesEpiglottitis PDFhasan benokriNo ratings yet
- A. Gestational Diabetes Mellitus B. Secondary Diabetes Mellitus D. Type II Diabetes MellitusDocument32 pagesA. Gestational Diabetes Mellitus B. Secondary Diabetes Mellitus D. Type II Diabetes MellitusNebawNo ratings yet
- Chronic Kidney DiseaseDocument11 pagesChronic Kidney Diseasenaly23No ratings yet
- Nutri WopsDocument4 pagesNutri WopsRizzy Ugay100% (1)
- KARDEX Case 3Document3 pagesKARDEX Case 3Juviely PremacioNo ratings yet
- Chronic Kidney DiseaseDocument11 pagesChronic Kidney DiseaseMah AlfaroNo ratings yet
- Use of Rare Remedies in Homoeopathic Practice: Dr. Ayush Kumar GuptaDocument8 pagesUse of Rare Remedies in Homoeopathic Practice: Dr. Ayush Kumar GuptaIndhumathiNo ratings yet
- The Four Temperaments of Fandom: June 2016Document8 pagesThe Four Temperaments of Fandom: June 2016IndhumathiNo ratings yet
- 1999 4 PDFDocument3 pages1999 4 PDFIndhumathiNo ratings yet
- Anisometropia PDFDocument2 pagesAnisometropia PDFIndhumathiNo ratings yet
- Iii BHMS Syllabus PDFDocument11 pagesIii BHMS Syllabus PDFIndhumathiNo ratings yet
- 8 NEW Case Taking RepertoryDocument14 pages8 NEW Case Taking RepertoryIndhumathiNo ratings yet
- Research Gate ManuscriptDocument53 pagesResearch Gate ManuscriptIndhumathiNo ratings yet
- SCAhuja-CoconutAAH18 3Document29 pagesSCAhuja-CoconutAAH18 3IndhumathiNo ratings yet
- Glucuronic Acid From Fermented Beverages: Biochemical Functions in Humans and Its Role in Health ProtectionDocument14 pagesGlucuronic Acid From Fermented Beverages: Biochemical Functions in Humans and Its Role in Health ProtectionIndhumathiNo ratings yet
- Smith, Thompson, C. D. Bonner, S. C.: Was ToatDocument12 pagesSmith, Thompson, C. D. Bonner, S. C.: Was ToatIndhumathiNo ratings yet
- Preparation and Reaction of Carboxylic AcidsDocument6 pagesPreparation and Reaction of Carboxylic AcidsIndhumathiNo ratings yet
- Analysis and Evaluation of Rubrics Symptoms of DR Kent S Repertory of HomeoDocument11 pagesAnalysis and Evaluation of Rubrics Symptoms of DR Kent S Repertory of HomeoIndhumathiNo ratings yet
- Production Norms: Foundation I Tofoundation IiDocument4 pagesProduction Norms: Foundation I Tofoundation IiIndhumathiNo ratings yet
- IJPPR Vol10 Issue4 Article2Document7 pagesIJPPR Vol10 Issue4 Article2IndhumathiNo ratings yet
- 20131018Document4 pages20131018IndhumathiNo ratings yet
- Nutritional Aspects of CerealsDocument32 pagesNutritional Aspects of CerealsFlorinNo ratings yet
- Hyposplenic Review 2011Document12 pagesHyposplenic Review 2011IndhumathiNo ratings yet
- What Is Folic Acid Used For?Document2 pagesWhat Is Folic Acid Used For?IndhumathiNo ratings yet
- Index A - B: © SURGICAL HOLDINGS 2001 REV:05/2015Document14 pagesIndex A - B: © SURGICAL HOLDINGS 2001 REV:05/2015IndhumathiNo ratings yet
- Labour Admission Test: International Journal of Infertility and Fetal Medicine December 2011Document8 pagesLabour Admission Test: International Journal of Infertility and Fetal Medicine December 2011IndhumathiNo ratings yet
- Koh PrepDocument4 pagesKoh PrepIndhumathiNo ratings yet
- Assessment of Pregnancy Outcome in Primigravida: Comparison Between Booked and Un-Booked PatientsDocument3 pagesAssessment of Pregnancy Outcome in Primigravida: Comparison Between Booked and Un-Booked PatientsIndhumathiNo ratings yet
- Hang Drop PDFDocument2 pagesHang Drop PDFIndhumathiNo ratings yet
- Common Laboratory Investigations in Obstetrics and GynaecologyDocument4 pagesCommon Laboratory Investigations in Obstetrics and GynaecologyIndhumathiNo ratings yet
- The Pap Test and Bethesda 2014: ReviewDocument12 pagesThe Pap Test and Bethesda 2014: ReviewIndhumathiNo ratings yet
- Calculations PracticeDocument16 pagesCalculations PracticeMasarrah Alchi100% (1)
- Renal Function TestsDocument26 pagesRenal Function TestsDr. Ashish Jawarkar100% (1)
- CilazaprilDocument24 pagesCilazaprilMarcelle GuimarãesNo ratings yet
- 3 Biomedicine The Profession DMPK Lena Gustavsson 2015 FinalDocument50 pages3 Biomedicine The Profession DMPK Lena Gustavsson 2015 FinalJayrine MonteroNo ratings yet
- Adme PDFDocument29 pagesAdme PDFGopi JayaramanNo ratings yet
- LidocaineDocument27 pagesLidocaineNadya PrafitaNo ratings yet
- Pharmacokinetics Review CEE With Practice ProblemsDocument148 pagesPharmacokinetics Review CEE With Practice ProblemsBenhur Leithold LapitanNo ratings yet
- GELOFUSINE FinalSPCDocument9 pagesGELOFUSINE FinalSPCRoxana CalderonNo ratings yet
- CM PDFDocument50 pagesCM PDFGarth BrionesNo ratings yet
- How The Body Affects The Drugs: College of Health SciencesDocument42 pagesHow The Body Affects The Drugs: College of Health SciencesNat Lynne Distor TrondilloNo ratings yet
- Bourne, DavidW. A. - Strauss, Steven - Mathematical Modeling of Pharmacokinetic Data (2018, CRC Press - Routledge)Document153 pagesBourne, DavidW. A. - Strauss, Steven - Mathematical Modeling of Pharmacokinetic Data (2018, CRC Press - Routledge)GuillermoNo ratings yet
- ZavzpretDocument21 pagesZavzpretNeethu Anna StephenNo ratings yet
- Literature 2 - Pregabalin Vs GabapentinDocument10 pagesLiterature 2 - Pregabalin Vs GabapentinKeke NechNo ratings yet
- Drugs and Pharmaceutical Technology Question BankDocument7 pagesDrugs and Pharmaceutical Technology Question BankVanitha ENo ratings yet
- Definitions: - PharmacokineticsDocument31 pagesDefinitions: - PharmacokineticsmebibegNo ratings yet
- MCQ Biochemistry LipidsDocument38 pagesMCQ Biochemistry LipidsstuffNo ratings yet
- Nelson GNDocument280 pagesNelson GNNirvair SinghNo ratings yet
- Duodopa Intestinal Gel ENG SMPC - 09001be68007fc9a PDFDocument16 pagesDuodopa Intestinal Gel ENG SMPC - 09001be68007fc9a PDFmochkurniawanNo ratings yet
- AUBF QUiZDocument12 pagesAUBF QUiZGene Narune GaronitaNo ratings yet
- Renal Replacement Therapies in Critical CareDocument46 pagesRenal Replacement Therapies in Critical CareLe ThyNo ratings yet
- S 016 LBLDocument23 pagesS 016 LBLMuhammadAmdadulHoqueNo ratings yet
- AminoglycosidesDocument55 pagesAminoglycosidesIndira ButkoonNo ratings yet
- Kompartemen 1 TerbukaDocument64 pagesKompartemen 1 TerbukaNgakanNo ratings yet
- Safety and Safe MedicationDocument92 pagesSafety and Safe MedicationAngel FiloteoNo ratings yet
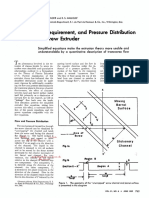
- Flow,: Power Requirement, and Pressure Distribution of Fluid in A Screw ExtruderDocument6 pagesFlow,: Power Requirement, and Pressure Distribution of Fluid in A Screw ExtruderLê Văn HòaNo ratings yet
- Insulin PDFDocument6 pagesInsulin PDFAttila TamasNo ratings yet
- Drug Use in Paeds and ElderlyDocument27 pagesDrug Use in Paeds and ElderlyCuthbert Tinotenda MusarurwaNo ratings yet
- Clinical-Chemistry-MB-Reviewer 2Document14 pagesClinical-Chemistry-MB-Reviewer 2Aubrey Jane TagolinoNo ratings yet
- Renal SystemDocument85 pagesRenal SystemFerasKarajehNo ratings yet