Download as pdf or txt
You might also like
- Louis S. Constine MD, Nancy J. Tarbell MD, Edward C. Halperin MD - Pediatric Radiation Oncology (2016, LWW) PDFDocument2,424 pagesLouis S. Constine MD, Nancy J. Tarbell MD, Edward C. Halperin MD - Pediatric Radiation Oncology (2016, LWW) PDFPan50% (2)
- Common ICU DripsDocument1 pageCommon ICU DripsSunshine Willis100% (2)
- GMC Official PLAB 1 Question SampleDocument8 pagesGMC Official PLAB 1 Question Samplemuntaser100% (1)
- 2019 Practice of Anesthesia For Infants and ChildrenDocument2 pages2019 Practice of Anesthesia For Infants and ChildrenJavier GlezqNo ratings yet
- Nutrition Case StudyDocument30 pagesNutrition Case StudyCher BautistaNo ratings yet
- Dr. Rubi Li v. Spouses Reynaldo and Lina SolimanDocument2 pagesDr. Rubi Li v. Spouses Reynaldo and Lina Solimanralph_atmosferaNo ratings yet
- Medad TeamDocument18 pagesMedad TeamAxmed MaxamedNo ratings yet
- UNC ED Pediatric Asthma Protocol 1-29-15 KJRDocument2 pagesUNC ED Pediatric Asthma Protocol 1-29-15 KJRMax ImousNo ratings yet
- Drug Indications&DosagesDocument3 pagesDrug Indications&DosagesSAMWEL JOSIANo ratings yet
- Tablas de Dosificacion Kirk 9na EdDocument68 pagesTablas de Dosificacion Kirk 9na EdMarlieth Rosales HernandezNo ratings yet
- Dosis Obat AnakDocument3 pagesDosis Obat AnakhannaNo ratings yet
- Dosis Obat AnakDocument3 pagesDosis Obat Anakimam mulyadiNo ratings yet
- Ambulatory Care MedicineDocument26 pagesAmbulatory Care MedicineJustineValJadeLacabaNo ratings yet
- COVID MX BsmmuDocument2 pagesCOVID MX BsmmuNuhiat NahreenNo ratings yet
- Age 2 Months Age 2monthsDocument1 pageAge 2 Months Age 2monthsd'Agung NugrohoNo ratings yet
- FLCCC Alliance MATHplus Protocol ENGLISHDocument2 pagesFLCCC Alliance MATHplus Protocol ENGLISHBhanu Kumar100% (1)
- SDL Obat EmergencyDocument26 pagesSDL Obat EmergencyfarhantunichiaNo ratings yet
- Analgesia y Anestesia para ConejosDocument7 pagesAnalgesia y Anestesia para ConejosIgnacio Rosas TellezNo ratings yet
- 2015 Pain Management For PediatricDocument2 pages2015 Pain Management For Pediatricdiany astutiNo ratings yet
- AsthmaDocument2 pagesAsthmaAndrei MurariuNo ratings yet
- Igd RsudDocument6 pagesIgd RsudRidho FrihaNo ratings yet
- Drug Dosages KTHDocument20 pagesDrug Dosages KTHQazi Saadullah LatifNo ratings yet
- Picu NotesDocument65 pagesPicu NotesAhmed Mohammed100% (2)
- COVID19 - DexamethasoneDocument2 pagesCOVID19 - DexamethasoneLe Hoang TuanNo ratings yet
- Emrgency DrugsDocument4 pagesEmrgency Drugshacker ammerNo ratings yet
- FLCCC Alliance MATHplus Protocol ENGLISHDocument3 pagesFLCCC Alliance MATHplus Protocol ENGLISHJhonn BlackNo ratings yet
- Brief Outline Questions To Ask: Acute AsthmaDocument15 pagesBrief Outline Questions To Ask: Acute AsthmaLevina AudreyNo ratings yet
- Obtain 12 Lead ECG and Cardiology ConsultationDocument2 pagesObtain 12 Lead ECG and Cardiology ConsultationPauline ChanNo ratings yet
- FLCCC Alliance MATHplus Protocol ENGLISHDocument3 pagesFLCCC Alliance MATHplus Protocol ENGLISHfernandohNo ratings yet
- Station 3 LeafletDocument5 pagesStation 3 LeafletFelicianna Ashwinie StanleyNo ratings yet
- Pediatric IV Push Quick ED Reference TableDocument4 pagesPediatric IV Push Quick ED Reference TableTayyab RazaNo ratings yet
- Table 17-3 - Common Endotracheal Intubation Medication IndicatDocument1 pageTable 17-3 - Common Endotracheal Intubation Medication IndicatDragutin PetrićNo ratings yet
- 4 Drugs Used in GastrointestinalDocument13 pages4 Drugs Used in Gastrointestinalrajkumar871992No ratings yet
- Pediatric Medication Dosing GuildelinesDocument2 pagesPediatric Medication Dosing GuildelinesMuhammad ZeeshanNo ratings yet
- ICE DrugsDocument2 pagesICE DrugsRichelle FrondaNo ratings yet
- Recommended Doses of Medications To Treat Children With An Acute Asthma ExacerbaDocument3 pagesRecommended Doses of Medications To Treat Children With An Acute Asthma Exacerbaمعاذ الشريفNo ratings yet
- Hospital Treatment Protocol For Covid-19Document4 pagesHospital Treatment Protocol For Covid-19Adrian BoboceaNo ratings yet
- 04 Chapter Respiratory SystemDocument18 pages04 Chapter Respiratory SystemMSKCNo ratings yet
- Tuberculosis: Sudchaya Prasoetpan (R1 Silpakorn University Residency Program)Document56 pagesTuberculosis: Sudchaya Prasoetpan (R1 Silpakorn University Residency Program)moraceaebmNo ratings yet
- Poster On Epilepsy Management in CaninesDocument1 pagePoster On Epilepsy Management in Caninessai hemachandNo ratings yet
- Drug Therapy For PicuDocument32 pagesDrug Therapy For PicuNeethu Mariya MathewNo ratings yet
- QR Klinik Kesihatan Setting, by DR Gerard Loh DMDocument34 pagesQR Klinik Kesihatan Setting, by DR Gerard Loh DMlailatul husnaNo ratings yet
- ANTI-ARRHYTHMIC DRUGS Veterinary PharmacologyDocument5 pagesANTI-ARRHYTHMIC DRUGS Veterinary PharmacologyljramosNo ratings yet
- NICU Drugs GuideDocument49 pagesNICU Drugs GuideArhanNo ratings yet
- PCP Example 2Document15 pagesPCP Example 2Pau Joy EstarezNo ratings yet
- UVA Phenobarb Protocol Sdutta 8-4-21Document3 pagesUVA Phenobarb Protocol Sdutta 8-4-21Shourik DuttaNo ratings yet
- Doses de MedicamentosDocument1 pageDoses de MedicamentosSoraya Bio VetNo ratings yet
- Marik Covid Protocol Summary PDFDocument2 pagesMarik Covid Protocol Summary PDFJody VivasNo ratings yet
- Rsud Kabupaten Bengkayang Bidang Anestesi Anesthesia Medication DosagesDocument5 pagesRsud Kabupaten Bengkayang Bidang Anestesi Anesthesia Medication DosagesBonny ChristianNo ratings yet
- Paramedic Drugs: Drug Class Indications Dosage NameDocument14 pagesParamedic Drugs: Drug Class Indications Dosage NameIbrahem Al100% (7)
- Rsud Sijunjung Obat Dosis Sediaan: KejangDocument2 pagesRsud Sijunjung Obat Dosis Sediaan: KejangAprita SaparNo ratings yet
- Paediatricshouseofficerguidehospitalkulim 151026150042 Lva1 App6891Document14 pagesPaediatricshouseofficerguidehospitalkulim 151026150042 Lva1 App6891Nadia SalwaniNo ratings yet
- 40kg Fent - dex.InitialGoal Directed Comfort Algorithm 1 Page Less Than 40 KG - 01!26!2018Document2 pages40kg Fent - dex.InitialGoal Directed Comfort Algorithm 1 Page Less Than 40 KG - 01!26!2018Georgia DugaciNo ratings yet
- CalciumchannelalgorithmDocument1 pageCalciumchannelalgorithmLind YLNo ratings yet
- Bagan KejangDocument10 pagesBagan KejangNie' MKNo ratings yet
- Dose Modification GuidelinesDocument1 pageDose Modification GuidelinesAhmed Maged FadelNo ratings yet
- 1: Adhd: Scientific Name Dose CommentsDocument4 pages1: Adhd: Scientific Name Dose CommentsSadiq Abdo92No ratings yet
- Dilution Protocol For AdultsDocument23 pagesDilution Protocol For AdultsSharumathi ChandraNo ratings yet
- Dosis Puyer Sudah UrutDocument1 pageDosis Puyer Sudah UrutSvara SenjaNo ratings yet
- FLCCC Alliance MATHplus Protocol ENGLISHDocument3 pagesFLCCC Alliance MATHplus Protocol ENGLISHDavid GrayNo ratings yet
- Notes in Neonates محمد ابراهيم مستشفى قوص قنا.WhiteKnightLoveDocument77 pagesNotes in Neonates محمد ابراهيم مستشفى قوص قنا.WhiteKnightLoveMaRwa IbrahimNo ratings yet
- الأدوية والجرعاتDocument1 pageالأدوية والجرعاتsalehtaha1989No ratings yet
- Missed Doses of Long Acting InjectionsDocument5 pagesMissed Doses of Long Acting InjectionsAbdualaziz AlmalkiNo ratings yet
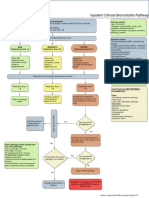
- Bronchiolitis Pathway InpatientDocument1 pageBronchiolitis Pathway Inpatientd'Agung NugrohoNo ratings yet
- Age 2 Months Age 2monthsDocument1 pageAge 2 Months Age 2monthsd'Agung NugrohoNo ratings yet
- Children's Hospital at Montefiore-IV Access Pathway: Predictor 0 Points 1 Point 2 PointsDocument1 pageChildren's Hospital at Montefiore-IV Access Pathway: Predictor 0 Points 1 Point 2 Pointsd'Agung NugrohoNo ratings yet
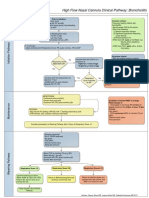
- High Flow Nasal Cannula Clinical Pathway: Bronchiolitis: Prior To Initiation: Inclusion CriteriaDocument1 pageHigh Flow Nasal Cannula Clinical Pathway: Bronchiolitis: Prior To Initiation: Inclusion Criteriad'Agung NugrohoNo ratings yet
- Bonus 2010 FA Step 1 Micro HIVDocument1 pageBonus 2010 FA Step 1 Micro HIVGabriel F. SotoNo ratings yet
- BT PTW GenogramDocument10 pagesBT PTW GenogramShashi YNNo ratings yet
- ArsenicDocument17 pagesArsenicChandrakumar Singh KhumukchambaNo ratings yet
- AMLS Mobile Reference GuideDocument6 pagesAMLS Mobile Reference GuideLim Jun Bin100% (1)
- Significance of Family History in Homoeopathic PrescribingDocument8 pagesSignificance of Family History in Homoeopathic PrescribingHomoeopathic Pulse50% (2)
- SSPL Product Brochure & Co Profile With Clients ListDocument12 pagesSSPL Product Brochure & Co Profile With Clients Listrohitagarwal_hlwNo ratings yet
- Neck DissectionDocument25 pagesNeck DissectionAdi SitaruNo ratings yet
- Standard Treatment Guidelines AND Essential Drugs List: Ministry of Health, Tonga-2007Document391 pagesStandard Treatment Guidelines AND Essential Drugs List: Ministry of Health, Tonga-2007Citra Ayu ApriliaNo ratings yet
- Serum Protein Electrophoresis and Immunofixation - BookFRev2web - PDF Oct 9, 2014Document19 pagesSerum Protein Electrophoresis and Immunofixation - BookFRev2web - PDF Oct 9, 2014mob3No ratings yet
- Askep Dalam Bahasa InggrisDocument6 pagesAskep Dalam Bahasa InggrisDhian Aji CandraNo ratings yet
- Vegetarianism: Sri Swami SivanandaDocument3 pagesVegetarianism: Sri Swami SivanandacusumanofrancNo ratings yet
- Management of Pregnant Patient in DentistryDocument10 pagesManagement of Pregnant Patient in DentistryVíctor Orduña LópezNo ratings yet
- Biotechnology Impact On SocietyDocument4 pagesBiotechnology Impact On SocietyEugeneKimANo ratings yet
- Pathophysiology of AppendicitisDocument2 pagesPathophysiology of AppendicitisDivine Jane Purcia67% (3)
- Schramm A., Gellrich N-C., Schmelzeisen R.-Navigational Surgery of The Facial Skeleton (2007)Document172 pagesSchramm A., Gellrich N-C., Schmelzeisen R.-Navigational Surgery of The Facial Skeleton (2007)Remus ChirciuNo ratings yet
- Product Monograph: (Clindamycin Phosphate Topical Solution USP)Document13 pagesProduct Monograph: (Clindamycin Phosphate Topical Solution USP)igunpharmNo ratings yet
- Thesis Statement About CigarettesDocument5 pagesThesis Statement About Cigarettesfexschhld100% (2)
- Ppz3o - Unit 1Document136 pagesPpz3o - Unit 1api-266151891No ratings yet
- Recurrent Pregnancy LossDocument211 pagesRecurrent Pregnancy LossGopal Kumar Das100% (1)
- Efusi Pleura & EmpyemaDocument47 pagesEfusi Pleura & EmpyemaArumLaksmitaDewiNo ratings yet
- Thyroid SwellingDocument8 pagesThyroid SwellingDn Ezrinah Dn Esham50% (2)
- Campus Map Building List PDFDocument1 pageCampus Map Building List PDFRicky Quizzagan MaguigadNo ratings yet
- NP 5Document28 pagesNP 5Trixia LivinaNo ratings yet
- Linear Quadratic (LQ) Model & Biological Based Treatment Planning - Dr. Manoj GuptaDocument60 pagesLinear Quadratic (LQ) Model & Biological Based Treatment Planning - Dr. Manoj GuptaSudhan Rajan100% (3)
- Maxillofacial Privileges QGHDocument4 pagesMaxillofacial Privileges QGHSanam FaheemNo ratings yet
- L 5 - Lungs PathologyDocument128 pagesL 5 - Lungs PathologyDiana Popovici100% (1)