Download as pdf or txt
You might also like
- How To Make Your Own Colloidal SilverDocument21 pagesHow To Make Your Own Colloidal Silverrawzero92% (12)
- Paper 4 Publication 333Document14 pagesPaper 4 Publication 333leBariNo ratings yet
- Final Argumentative EssayDocument8 pagesFinal Argumentative EssayMatthew EbaluNo ratings yet
- Hygienic Practices Among Food Vendors in Educational Institutions in Ghana: The Case of KonongoDocument14 pagesHygienic Practices Among Food Vendors in Educational Institutions in Ghana: The Case of KonongoEarl John Barroga SolamoNo ratings yet
- Application of The WHO Keys of Safer Food To Improve Food Handling Practices of Food Vendors in A Poor Resource Community in GhanaDocument10 pagesApplication of The WHO Keys of Safer Food To Improve Food Handling Practices of Food Vendors in A Poor Resource Community in GhanaOldriana Prawiro HapsariNo ratings yet
- Food Hygienic Practices and Safety Measures AmongDocument7 pagesFood Hygienic Practices and Safety Measures AmongIntrovert PrinzNo ratings yet
- 9+food Safety and Hygiene Standards in The Hospitality Industry by Sarthak Mahajan and Anshu SinghDocument16 pages9+food Safety and Hygiene Standards in The Hospitality Industry by Sarthak Mahajan and Anshu Singhmaedehmohamadian80No ratings yet
- Evaluation of Basic Knowledge On Food Safety and Food Handling Practices Amongst Migrant in MalaysiaDocument10 pagesEvaluation of Basic Knowledge On Food Safety and Food Handling Practices Amongst Migrant in MalaysiaSiska PratiwiNo ratings yet
- Main Main - Final - Result - Project - 2Document65 pagesMain Main - Final - Result - Project - 2Ebuka AniNo ratings yet
- The Final Result Project 2Document32 pagesThe Final Result Project 2Ebuka AniNo ratings yet
- Food Handling Serving and Hygiene PractiDocument7 pagesFood Handling Serving and Hygiene PractiFarha KamilatunNo ratings yet
- Food Safety Practices Among Vendors in Capaoay San Jacinto PangasinanDocument4 pagesFood Safety Practices Among Vendors in Capaoay San Jacinto PangasinanPatricia Mae SabadoNo ratings yet
- Relationship of Knowledge and Attitude With Food Handling Practices: A Systematic ReviewDocument12 pagesRelationship of Knowledge and Attitude With Food Handling Practices: A Systematic ReviewIJPHSNo ratings yet
- Staphylococcus Aureus, Campylobacter, Rotavirus and Enteric Bacteria Are Identified (1,2)Document2 pagesStaphylococcus Aureus, Campylobacter, Rotavirus and Enteric Bacteria Are Identified (1,2)Achmad Faoezan GandjilNo ratings yet
- GROUP 3.docx One TitleDocument18 pagesGROUP 3.docx One TitleEllaine Ann AbundaNo ratings yet
- Articulo - Food Safety and Education LevelDocument6 pagesArticulo - Food Safety and Education LevelNicole PerezNo ratings yet
- Microbial Quality and Safety of Cooked Foods Sold in Urban Schools in Ghana: A Review of Food Handling and Health Implications Ghana A Review of Food Handling and Health ImplicationsDocument10 pagesMicrobial Quality and Safety of Cooked Foods Sold in Urban Schools in Ghana: A Review of Food Handling and Health Implications Ghana A Review of Food Handling and Health ImplicationsresearchpublichealthNo ratings yet
- Food Safety 3Document22 pagesFood Safety 3Syarahdita Fransiska RaniNo ratings yet
- 234684535Document8 pages234684535Safi MohammedNo ratings yet
- Essay Article On Consumer Awareness Towards Food SafetyDocument4 pagesEssay Article On Consumer Awareness Towards Food SafetyMohd Faizal Bin AyobNo ratings yet
- FoodhygiencepaperDocument10 pagesFoodhygiencepaperHamid AshrafNo ratings yet
- Food Safety Practices Among Street Food VendorsDocument8 pagesFood Safety Practices Among Street Food VendorsDiana Rose BayangNo ratings yet
- Research Grade 12Document21 pagesResearch Grade 12riclyde cahucom100% (1)
- Chapter 22Document11 pagesChapter 22MaryGraceVelascoFuentesNo ratings yet
- Factors Influence Awareness Canteen Student MalaysiaDocument4 pagesFactors Influence Awareness Canteen Student MalaysiaPawitra RamuNo ratings yet
- RESEARCH - Chapter 1Document9 pagesRESEARCH - Chapter 1Ivan PadecioNo ratings yet
- Assessment of Food Safety Knowledge, Attitude, Self-Reported Practices, and Microbiological Hand Hygiene of Food HandlersDocument14 pagesAssessment of Food Safety Knowledge, Attitude, Self-Reported Practices, and Microbiological Hand Hygiene of Food HandlersNadanNadhifahNo ratings yet
- Food Consumption Habits of Consumers in The Philippines: Changes Amidst The PandemicDocument8 pagesFood Consumption Habits of Consumers in The Philippines: Changes Amidst The PandemicIJPHSNo ratings yet
- Foods 02 00460Document2 pagesFoods 02 00460fssaimundraNo ratings yet
- Evaluating Food Safety Knowledge and Practices Among Foodservice Staff in Al Madinah Hospitals, Saudi ArabiaDocument19 pagesEvaluating Food Safety Knowledge and Practices Among Foodservice Staff in Al Madinah Hospitals, Saudi ArabiaAiza ConchadaNo ratings yet
- Understanding The Risk Landscape Analyzing Factors Impacting Food Vending in NigeriaDocument8 pagesUnderstanding The Risk Landscape Analyzing Factors Impacting Food Vending in NigeriaKIU PUBLICATION AND EXTENSIONNo ratings yet
- An Assessment of Food Safety Needs of Restaurants in Owerri, Imo State, NigeriaDocument14 pagesAn Assessment of Food Safety Needs of Restaurants in Owerri, Imo State, NigeriaRizwan KhalidNo ratings yet
- RecheckDocument11 pagesRecheckPearl Jean SediegoNo ratings yet
- Background of The StudyDocument3 pagesBackground of The StudyKraeNo ratings yet
- Food Safety Attitude and Practice QuestiDocument7 pagesFood Safety Attitude and Practice QuestiHamid AshrafNo ratings yet
- Chapter 1Document8 pagesChapter 1Mikageシ TVNo ratings yet
- Assessment of Knowledge, Attitude and Practices Concerning Food Safety Among Restaurant Workers in Putrajaya, MalaysiaDocument10 pagesAssessment of Knowledge, Attitude and Practices Concerning Food Safety Among Restaurant Workers in Putrajaya, MalaysiaAlexander DeckerNo ratings yet
- 2023 Sanitary Quality HospitalDocument15 pages2023 Sanitary Quality HospitalRudy OcañaNo ratings yet
- Ijphs Fix B.inggrisDocument14 pagesIjphs Fix B.inggrisrizkimNo ratings yet
- Food Hygiene Standard Satisfaction of Singaporean Diners ChoiDocument23 pagesFood Hygiene Standard Satisfaction of Singaporean Diners Choijyap_62No ratings yet
- Assessment of The Food Hygiene Practices of Food Handlers in The Federal Capital Territory of NigeriaDocument6 pagesAssessment of The Food Hygiene Practices of Food Handlers in The Federal Capital Territory of Nigeriarafael514No ratings yet
- Food Safety Practices of Food Handlers Working inDocument13 pagesFood Safety Practices of Food Handlers Working inAnthony FloresNo ratings yet
- Group 7 BSN 3h Research ProposalDocument69 pagesGroup 7 BSN 3h Research ProposalLeah Mae TomasNo ratings yet
- Apjeas-2020 7 1 06Document7 pagesApjeas-2020 7 1 06ROY BULTRON CABARLESNo ratings yet
- Specific Hygiene Procedures and Practices AssessmentDocument4 pagesSpecific Hygiene Procedures and Practices AssessmentKatherine RomeoNo ratings yet
- Determinants of Food Safety Practices Among Food Handlers in Selected Food EstablishmentsDocument9 pagesDeterminants of Food Safety Practices Among Food Handlers in Selected Food EstablishmentsIJPHSNo ratings yet
- Knowledge, Attitudes and Practices of Food Hygiene Among Mobile Food Ven1ors in - 1Document17 pagesKnowledge, Attitudes and Practices of Food Hygiene Among Mobile Food Ven1ors in - 1Samson ArimatheaNo ratings yet
- The Problem and Its Setting Background of The StudyDocument70 pagesThe Problem and Its Setting Background of The StudyJoana Mae M. Wamar100% (1)
- Final PaperDocument27 pagesFinal PaperJan Leanne OrbigosoNo ratings yet
- Research Paper (Judy Garcia & Ybeth Duerme)Document8 pagesResearch Paper (Judy Garcia & Ybeth Duerme)Judy GarciaNo ratings yet
- Thesis About Improper Hygiene11Document18 pagesThesis About Improper Hygiene11Angelie UmambacNo ratings yet
- Foods 10 01878 v2Document11 pagesFoods 10 01878 v2Anchang Don MaximNo ratings yet
- DocumentationDocument4 pagesDocumentationnurNo ratings yet
- Food Safety Guidelines 1Document6 pagesFood Safety Guidelines 1Ella DenostaNo ratings yet
- Unit 4 FSQCDocument28 pagesUnit 4 FSQCvaralakshmi KNo ratings yet
- Research PaperDocument19 pagesResearch PaperDearlyne AlmazanNo ratings yet
- Food Safety Knowledge and Self-Reported Practices PDFDocument29 pagesFood Safety Knowledge and Self-Reported Practices PDFAlle Eiram PadilloNo ratings yet
- Final Research WCC FORMAT FOOD SAFETY AND SANITATION PRACTICESDocument27 pagesFinal Research WCC FORMAT FOOD SAFETY AND SANITATION PRACTICESlowi shooNo ratings yet
- Research 22Document22 pagesResearch 22Mhylgray AniñonNo ratings yet
- Related Literatures by MeDocument4 pagesRelated Literatures by MeJanna DatahanNo ratings yet
- Yahaya Musa Balarabe's Project CHAPTER ONE To ThreeDocument25 pagesYahaya Musa Balarabe's Project CHAPTER ONE To ThreeJonah MerabNo ratings yet
- A Cross Sectional Study On Food Safety Knowledge Among Adult ConsumersDocument8 pagesA Cross Sectional Study On Food Safety Knowledge Among Adult ConsumersAlina ShahidNo ratings yet
- Gastronomic Guardians : Safeguarding Food Safety at Home and BeyondFrom EverandGastronomic Guardians : Safeguarding Food Safety at Home and BeyondNo ratings yet
- Acute Diarrhea in Adults and Children A Global PerspectiveDocument10 pagesAcute Diarrhea in Adults and Children A Global PerspectiverobyNo ratings yet
- Literature ReviewDocument2 pagesLiterature ReviewericNo ratings yet
- V. Mallikarjun RaoDocument6 pagesV. Mallikarjun Raonurahmi widyani ratriNo ratings yet
- First Aid With Essential Oils.Document5 pagesFirst Aid With Essential Oils.Vicki O'MalleyNo ratings yet
- Review On Antimicrobial ResistanceDocument2 pagesReview On Antimicrobial ResistancePiNo ratings yet
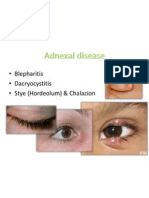
- Adnexal Diseases, Corneal Abrasion, FBDocument13 pagesAdnexal Diseases, Corneal Abrasion, FBPatt PopNo ratings yet
- Colloidal Silver Everything You Need To KnowDocument7 pagesColloidal Silver Everything You Need To Knowsanyu33333No ratings yet
- Adult Combined Schedule VaccineDocument33 pagesAdult Combined Schedule VaccinehatsuneNo ratings yet
- English 10 w1Document22 pagesEnglish 10 w1Bernadette Manili LptNo ratings yet
- Composition of Vaginal Microbiota and Their Antibiotic Susceptibility in Symptomatic WomenDocument6 pagesComposition of Vaginal Microbiota and Their Antibiotic Susceptibility in Symptomatic WomenAmirah MohdNo ratings yet
- Sepsis: Dr. Cristhian Huanca Panozo Medicina InternaDocument25 pagesSepsis: Dr. Cristhian Huanca Panozo Medicina InternafranciNo ratings yet
- CHN Sample NLE QuestionnairesDocument3 pagesCHN Sample NLE QuestionnairesJheanAlphonsineT.MeansNo ratings yet
- Early Myocardial Infarction Detection by Joshi Etal BMDDocument123 pagesEarly Myocardial Infarction Detection by Joshi Etal BMDtv20692No ratings yet
- Laboratory Associated Infections: Tania Chintya IKD BiomedikDocument16 pagesLaboratory Associated Infections: Tania Chintya IKD BiomedikTania Chintya Dewi KarimaNo ratings yet
- BIOTECH - DOST Tawa Tawa Food SupplementDocument7 pagesBIOTECH - DOST Tawa Tawa Food SupplementJoven CedricNo ratings yet
- 07-2006 Chassin Operative Strategy - Colorectal SurgeryDocument293 pages07-2006 Chassin Operative Strategy - Colorectal SurgeryConstantin DaradiciNo ratings yet
- Pain in The Throne: Cristal Ann Laquindanum TMC ER RotationDocument39 pagesPain in The Throne: Cristal Ann Laquindanum TMC ER RotationAkhil SunkariNo ratings yet
- Anaplasmosis in Farm AnimalsDocument2 pagesAnaplasmosis in Farm AnimalsANURAGNo ratings yet
- Bios Life Slim UAEDocument4 pagesBios Life Slim UAEJey BautistaNo ratings yet
- Abstract BookDocument317 pagesAbstract BookAyesha WaheedNo ratings yet
- Dengvaxia Position PaperDocument2 pagesDengvaxia Position PaperErlinda PosadasNo ratings yet
- English 10 1st Quarter Examination 22Document4 pagesEnglish 10 1st Quarter Examination 22Christian Jay PresiidenteNo ratings yet
- The Mortality of Cholera in EnglandDocument506 pagesThe Mortality of Cholera in England杨振宇No ratings yet
- Endocrine Drugs: Pituitary, Thyroid, Parathyroid, and Adrenal DisordersDocument29 pagesEndocrine Drugs: Pituitary, Thyroid, Parathyroid, and Adrenal DisordersPam LalaNo ratings yet
- College of Medicine & Health SciencesDocument56 pagesCollege of Medicine & Health SciencesMebratu DemessNo ratings yet
- Extra PointsDocument7 pagesExtra Pointspeter911x100% (2)