
Amr Awareness Ppra Rs 2016abcde
Amr Awareness Ppra Rs 2016abcde
You might also like
- Kiran Mazumdar Shaw - 1Document15 pagesKiran Mazumdar Shaw - 1jincyalexander190% (1)
- BIOT643 Midterm Exam Summer 2016Document4 pagesBIOT643 Midterm Exam Summer 2016JayNo ratings yet
- Global Problem Amrws Ppra Kars Ed CP Compressed - 998Document28 pagesGlobal Problem Amrws Ppra Kars Ed CP Compressed - 998budi darmantaNo ratings yet
- Dr. Hari Paraton - Global Problem AMR - WS PPRA KARS Ed CPDocument28 pagesDr. Hari Paraton - Global Problem AMR - WS PPRA KARS Ed CPindriNo ratings yet
- WISELY USE OF ANTIBIOTIC - Revisi Agust 2018Document54 pagesWISELY USE OF ANTIBIOTIC - Revisi Agust 2018Dea PhillyaNo ratings yet
- Hari - Amr Problem - Praud IV 2019Document40 pagesHari - Amr Problem - Praud IV 2019rosaliafriskaNo ratings yet
- Materi DrharrypDocument38 pagesMateri DrharrypAnnisa Aisyha MalikNo ratings yet
- Materi 2 AMR KPRADocument53 pagesMateri 2 AMR KPRArizkiameliahexshaNo ratings yet
- Mdro Global Amr 2018Document7 pagesMdro Global Amr 2018rifkidwianugrahNo ratings yet
- 01265d5a f80f 401e B0fa 1f96da9503d6 Antibiotik Bijak KolegiumDocument33 pages01265d5a f80f 401e B0fa 1f96da9503d6 Antibiotik Bijak KolegiumTRI GUMILARNo ratings yet
- AMR PERSI 18 - Prof. Tjandra (Rev)Document60 pagesAMR PERSI 18 - Prof. Tjandra (Rev)Yulia Wati Safitri SanjayaNo ratings yet
- AMR Kebijakan WHO - Regulator - BPOMDocument18 pagesAMR Kebijakan WHO - Regulator - BPOMPutri Febrina Rizki AmaliahNo ratings yet
- Combating The Antibiotic Resistance in PICUDocument31 pagesCombating The Antibiotic Resistance in PICUAngeline AdrianneNo ratings yet
- Materi 1 - Antimicrobial Stewardship - Prof TaralanDocument43 pagesMateri 1 - Antimicrobial Stewardship - Prof TaralanAyu RahmawatiNo ratings yet
- Seminar AB Res FARMASI - Fix TitikNDocument74 pagesSeminar AB Res FARMASI - Fix TitikNLuthfiyyaNo ratings yet
- Erwin - Antibiotic Stewardship Program - PRAUD IIIDocument11 pagesErwin - Antibiotic Stewardship Program - PRAUD IIIWidya Lestari CapawatyNo ratings yet
- Webinar PPRADocument22 pagesWebinar PPRARizqi TitisNo ratings yet
- RasproDocument63 pagesRasprofany hertinNo ratings yet
- 1.peran Manajemen PPRA RS - DR - Joni-DikonversiDocument21 pages1.peran Manajemen PPRA RS - DR - Joni-DikonversiYoan Flower100% (1)
- Antibiotic Residues in The Environment ofDocument4 pagesAntibiotic Residues in The Environment ofWahidNo ratings yet
- Booklet On Implementation of Antibiotic Stewardship ProgrammeDocument42 pagesBooklet On Implementation of Antibiotic Stewardship Programmedakmok100% (1)
- Antimicrobial Resistance in The Western Pacific Region: A Review of Surveillance and Health Systems ResponseDocument56 pagesAntimicrobial Resistance in The Western Pacific Region: A Review of Surveillance and Health Systems Response21NaiveNo ratings yet
- PF6400 - Antimicrobial StewardshipDocument63 pagesPF6400 - Antimicrobial StewardshipciaranNo ratings yet
- Materi 3 - Audit Kualitatif Dan Kasus - Hisfarsi 2023 PDFDocument57 pagesMateri 3 - Audit Kualitatif Dan Kasus - Hisfarsi 2023 PDFingrid devi carissaNo ratings yet
- Materi PERAN RS PADA PPRADocument9 pagesMateri PERAN RS PADA PPRAAndi Suwanto FamilyNo ratings yet
- Bjbs 80 11387Document11 pagesBjbs 80 11387Eli COMPAORENo ratings yet
- Antibiotic Usage in Common and Uncommon Infection in Primary Care Setting - Daerah RompinDocument91 pagesAntibiotic Usage in Common and Uncommon Infection in Primary Care Setting - Daerah RompinMonysyha AtriNo ratings yet
- Amr Concept, Causes & Response: Ministry of Health /public Health Directorate Antimicrobial Resistance Control DepartmentDocument28 pagesAmr Concept, Causes & Response: Ministry of Health /public Health Directorate Antimicrobial Resistance Control Departmentibrahimadnan040No ratings yet
- 1 Antimicrobial ResistanceDocument27 pages1 Antimicrobial ResistanceLorenz L. Llamas IIINo ratings yet
- Responsible Use of Antimicrobials in Fish Production: GuidelinesDocument21 pagesResponsible Use of Antimicrobials in Fish Production: GuidelinesDevaraj SubramanyamNo ratings yet
- Reducing Antimicrobial Use in Food AnimalsDocument4 pagesReducing Antimicrobial Use in Food AnimalsAli RazaNo ratings yet
- Gyssen DDD MethodDocument39 pagesGyssen DDD MethodDewi RinakantiNo ratings yet
- Henson 2019Document5 pagesHenson 2019Edimar Joshua FrialaNo ratings yet
- Principles of Treatment For Tuberculosis: SoedarsonoDocument40 pagesPrinciples of Treatment For Tuberculosis: SoedarsonoLolitha JuliawandaniNo ratings yet
- Microbial Pathogenesis: SciencedirectDocument8 pagesMicrobial Pathogenesis: SciencedirectMaria Silvana AlvesNo ratings yet
- Health Service Organisation Aaw 2021 Powerpoint PresentationDocument77 pagesHealth Service Organisation Aaw 2021 Powerpoint Presentationhassan shahidNo ratings yet
- Keamanan PanganDocument50 pagesKeamanan PanganmonaNo ratings yet
- Antibiotic Guardian Leaflet FINALDocument2 pagesAntibiotic Guardian Leaflet FINALStelvin SebastianNo ratings yet
- To Protect Human, Animal, Plant & Environmental Health: We Can All Help! Take Action NowDocument2 pagesTo Protect Human, Animal, Plant & Environmental Health: We Can All Help! Take Action NowFaozan FikriNo ratings yet
- Bauer 2019Document6 pagesBauer 2019RaffaharianggaraNo ratings yet
- Global Dan Nasional Problem AMR 2019Document36 pagesGlobal Dan Nasional Problem AMR 2019DewiNo ratings yet
- Intramammary Ethno-Veterinary Formulation in Bovine Mastitis Treatment For Optimization of Antibiotic UseDocument12 pagesIntramammary Ethno-Veterinary Formulation in Bovine Mastitis Treatment For Optimization of Antibiotic Usestephimarie2004No ratings yet
- Mini-Review: Antimicrobial Resistance and COVID-19 Syndemic: Impact On Public HealthDocument6 pagesMini-Review: Antimicrobial Resistance and COVID-19 Syndemic: Impact On Public HealthJhosua MendezNo ratings yet
- AMR Pocket Guide For Ministers - ArabicDocument12 pagesAMR Pocket Guide For Ministers - ArabicAhmad Al-RusasiNo ratings yet
- The Informative Value of An Overview On Antibiotic Consumption, Treatment Efficacy and Cost of Clinical Mastitis at Farm LevelDocument8 pagesThe Informative Value of An Overview On Antibiotic Consumption, Treatment Efficacy and Cost of Clinical Mastitis at Farm LeveljsolvarelaNo ratings yet
- PTO Infeksi WidyDocument28 pagesPTO Infeksi WidyNurhasna Sushmita SariNo ratings yet
- Antibiotherapy: F-Xavier Lescure Infectious Dieases Specialist Bichat Hospital, ParisDocument13 pagesAntibiotherapy: F-Xavier Lescure Infectious Dieases Specialist Bichat Hospital, ParisRaquel HerreraNo ratings yet
- Antibiotherapy: F-Xavier Lescure Infectious Dieases Specialist Bichat Hospital, ParisDocument12 pagesAntibiotherapy: F-Xavier Lescure Infectious Dieases Specialist Bichat Hospital, ParisMth TaharNo ratings yet
- Coipars ColombiaDocument12 pagesCoipars Colombiaduverney.gaviriaNo ratings yet
- Antibacterial Chemotherapy-Theory, Problems, and Practice (Oxford University Press)Document93 pagesAntibacterial Chemotherapy-Theory, Problems, and Practice (Oxford University Press)francieudo1No ratings yet
- Instabilite MeropenemDocument9 pagesInstabilite MeropenemSonguigama CoulibalyNo ratings yet
- ANTIMICROBIAL STEWARDSHIP PROGRAM Rs TajuddinDocument46 pagesANTIMICROBIAL STEWARDSHIP PROGRAM Rs Tajuddinapotek mars farmaNo ratings yet
- Antibiotik Bijak Di RS - Dr. Ronald Irwanto Natadidjaja, SpPD-KPTI, FINASIMDocument46 pagesAntibiotik Bijak Di RS - Dr. Ronald Irwanto Natadidjaja, SpPD-KPTI, FINASIMdeviamufidazNo ratings yet
- Antimicrobial Resistance of Salmonella From Poultry Meat in Brazil Results of A Nationwide SurveyDocument8 pagesAntimicrobial Resistance of Salmonella From Poultry Meat in Brazil Results of A Nationwide SurveyMatheus SouzaNo ratings yet
- Foods 11 03894Document15 pagesFoods 11 03894Hasna NoerNo ratings yet
- Michael D. Apley, DVM, PHD: Defining Antibiotic Stewardship in Veterinary and Human Medicine For The Rest of This CenturyDocument31 pagesMichael D. Apley, DVM, PHD: Defining Antibiotic Stewardship in Veterinary and Human Medicine For The Rest of This CenturyNational Press FoundationNo ratings yet
- Antimicrobial Resistance and Clinical Use in Respiratory InfectionsDocument23 pagesAntimicrobial Resistance and Clinical Use in Respiratory InfectionsWamique IzharNo ratings yet
- Martha Mamora (Adisseo) - Munas SCI 2022Document14 pagesMartha Mamora (Adisseo) - Munas SCI 2022ifaNo ratings yet
- Veterinary Internal Medicne - 2015 - Weese - ACVIM Consensus Statement On Therapeutic Antimicrobial Use in Animals andDocument12 pagesVeterinary Internal Medicne - 2015 - Weese - ACVIM Consensus Statement On Therapeutic Antimicrobial Use in Animals andkradoNo ratings yet
- Trends in Antibiotic Therapy: Rt. Rev. Prof. C.S.S. BelloDocument47 pagesTrends in Antibiotic Therapy: Rt. Rev. Prof. C.S.S. BelloanneNo ratings yet
- Microorganisms 10 01705 v2Document22 pagesMicroorganisms 10 01705 v2Joy WinchesterNo ratings yet
- C Value ParadoxDocument18 pagesC Value ParadoxKashish GuptaNo ratings yet
- Fermentation Biotechnology PDFDocument15 pagesFermentation Biotechnology PDFsadatrafia100% (1)
- Sem 1 - EVS SyllabusDocument9 pagesSem 1 - EVS SyllabusSmitali UkeyNo ratings yet
- MAT500 Paper PhylogeneticsDocument19 pagesMAT500 Paper PhylogeneticsScottMcRaeNo ratings yet
- BINUS University: Bioinformatics Road MapDocument16 pagesBINUS University: Bioinformatics Road MapIndonesian Journal of CancerNo ratings yet
- Bacteriophages in Health and DiseaseDocument297 pagesBacteriophages in Health and DiseaseCisticola100% (1)
- Mendelian and Non Mendelian GeneticsDocument28 pagesMendelian and Non Mendelian Geneticsf_ei810% (1)
- Bioinformatics I: Lecture NotesDocument180 pagesBioinformatics I: Lecture NotesDaniela GuardiaNo ratings yet
- PHD Studentship - Development of A 3D Printed Biohybrid Lung at Loughborough UniversityDocument3 pagesPHD Studentship - Development of A 3D Printed Biohybrid Lung at Loughborough UniversityOzden IsbilirNo ratings yet
- pmTFP1 PeroxisomesDocument4 pagespmTFP1 PeroxisomesAlleleBiotechNo ratings yet
- Lziff Dgqfno: G) KFN /SF/ CG' "RL - !Document18 pagesLziff Dgqfno: G) KFN /SF/ CG' "RL - !Menuka ShresthaNo ratings yet
- Bacteria in TempeDocument7 pagesBacteria in TempeHana HananiNo ratings yet
- Pharmacodynamics of AntibioticsDocument28 pagesPharmacodynamics of AntibioticsHazimMahmoudDarwishNo ratings yet
- All Genetics FRsDocument11 pagesAll Genetics FRsPineappleHeadNo ratings yet
- Genomic Dna Isolation From Human Whole Blood Samples by Non Enzymatic Salting Out MethodDocument2 pagesGenomic Dna Isolation From Human Whole Blood Samples by Non Enzymatic Salting Out MethodamandbhaskarNo ratings yet
- YeastDocument9 pagesYeastApril Mae ArcayaNo ratings yet
- An Introduction To Photosynthesis PDFDocument15 pagesAn Introduction To Photosynthesis PDFNyimas Hoirunisa100% (2)
- Application of Column Chromatography in PharmacyDocument5 pagesApplication of Column Chromatography in PharmacyJay Shah100% (2)
- 2020 Customer Updates 1Document24 pages2020 Customer Updates 1antoniogilmoreNo ratings yet
- Study of The Hydrolysis of Sugar Cane Bagasse Using Phosphoric AcidDocument11 pagesStudy of The Hydrolysis of Sugar Cane Bagasse Using Phosphoric AcidRené MartínezNo ratings yet
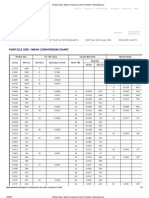
- Particle Size - Mesh Conversion Chart - Powder Technology IncDocument2 pagesParticle Size - Mesh Conversion Chart - Powder Technology IncSri Ram VikasNo ratings yet
- BiotechnologyDocument39 pagesBiotechnologyannaharNo ratings yet
- Amylase ProductionDocument5 pagesAmylase ProductionPraveen RohillaNo ratings yet
- Essentials of Genetics 8th Edition by Klug Cummings Spencer and Palladino ISBN Test BankDocument14 pagesEssentials of Genetics 8th Edition by Klug Cummings Spencer and Palladino ISBN Test Banklester100% (26)
- Mep and Civil TenderDocument471 pagesMep and Civil TenderJayadevDamodaran100% (1)
- BT1001 Biology For Engineers PDFDocument2 pagesBT1001 Biology For Engineers PDFsanthi saranyaNo ratings yet
- Modul-4 - Logistik TBDocument29 pagesModul-4 - Logistik TBlusyNo ratings yet
- More DNA Evidence Against Human Chromosome FusionDocument5 pagesMore DNA Evidence Against Human Chromosome FusionAriam MariaNo ratings yet























































































Download as pdf or txt
You might also like
- Kiran Mazumdar Shaw - 1Document15 pagesKiran Mazumdar Shaw - 1jincyalexander190% (1)
- BIOT643 Midterm Exam Summer 2016Document4 pagesBIOT643 Midterm Exam Summer 2016JayNo ratings yet
- Global Problem Amrws Ppra Kars Ed CP Compressed - 998Document28 pagesGlobal Problem Amrws Ppra Kars Ed CP Compressed - 998budi darmantaNo ratings yet
- Dr. Hari Paraton - Global Problem AMR - WS PPRA KARS Ed CPDocument28 pagesDr. Hari Paraton - Global Problem AMR - WS PPRA KARS Ed CPindriNo ratings yet
- WISELY USE OF ANTIBIOTIC - Revisi Agust 2018Document54 pagesWISELY USE OF ANTIBIOTIC - Revisi Agust 2018Dea PhillyaNo ratings yet
- Hari - Amr Problem - Praud IV 2019Document40 pagesHari - Amr Problem - Praud IV 2019rosaliafriskaNo ratings yet
- Materi DrharrypDocument38 pagesMateri DrharrypAnnisa Aisyha MalikNo ratings yet
- Materi 2 AMR KPRADocument53 pagesMateri 2 AMR KPRArizkiameliahexshaNo ratings yet
- Mdro Global Amr 2018Document7 pagesMdro Global Amr 2018rifkidwianugrahNo ratings yet
- 01265d5a f80f 401e B0fa 1f96da9503d6 Antibiotik Bijak KolegiumDocument33 pages01265d5a f80f 401e B0fa 1f96da9503d6 Antibiotik Bijak KolegiumTRI GUMILARNo ratings yet
- AMR PERSI 18 - Prof. Tjandra (Rev)Document60 pagesAMR PERSI 18 - Prof. Tjandra (Rev)Yulia Wati Safitri SanjayaNo ratings yet
- AMR Kebijakan WHO - Regulator - BPOMDocument18 pagesAMR Kebijakan WHO - Regulator - BPOMPutri Febrina Rizki AmaliahNo ratings yet
- Combating The Antibiotic Resistance in PICUDocument31 pagesCombating The Antibiotic Resistance in PICUAngeline AdrianneNo ratings yet
- Materi 1 - Antimicrobial Stewardship - Prof TaralanDocument43 pagesMateri 1 - Antimicrobial Stewardship - Prof TaralanAyu RahmawatiNo ratings yet
- Seminar AB Res FARMASI - Fix TitikNDocument74 pagesSeminar AB Res FARMASI - Fix TitikNLuthfiyyaNo ratings yet
- Erwin - Antibiotic Stewardship Program - PRAUD IIIDocument11 pagesErwin - Antibiotic Stewardship Program - PRAUD IIIWidya Lestari CapawatyNo ratings yet
- Webinar PPRADocument22 pagesWebinar PPRARizqi TitisNo ratings yet
- RasproDocument63 pagesRasprofany hertinNo ratings yet
- 1.peran Manajemen PPRA RS - DR - Joni-DikonversiDocument21 pages1.peran Manajemen PPRA RS - DR - Joni-DikonversiYoan Flower100% (1)
- Antibiotic Residues in The Environment ofDocument4 pagesAntibiotic Residues in The Environment ofWahidNo ratings yet
- Booklet On Implementation of Antibiotic Stewardship ProgrammeDocument42 pagesBooklet On Implementation of Antibiotic Stewardship Programmedakmok100% (1)
- Antimicrobial Resistance in The Western Pacific Region: A Review of Surveillance and Health Systems ResponseDocument56 pagesAntimicrobial Resistance in The Western Pacific Region: A Review of Surveillance and Health Systems Response21NaiveNo ratings yet
- PF6400 - Antimicrobial StewardshipDocument63 pagesPF6400 - Antimicrobial StewardshipciaranNo ratings yet
- Materi 3 - Audit Kualitatif Dan Kasus - Hisfarsi 2023 PDFDocument57 pagesMateri 3 - Audit Kualitatif Dan Kasus - Hisfarsi 2023 PDFingrid devi carissaNo ratings yet
- Materi PERAN RS PADA PPRADocument9 pagesMateri PERAN RS PADA PPRAAndi Suwanto FamilyNo ratings yet
- Bjbs 80 11387Document11 pagesBjbs 80 11387Eli COMPAORENo ratings yet
- Antibiotic Usage in Common and Uncommon Infection in Primary Care Setting - Daerah RompinDocument91 pagesAntibiotic Usage in Common and Uncommon Infection in Primary Care Setting - Daerah RompinMonysyha AtriNo ratings yet
- Amr Concept, Causes & Response: Ministry of Health /public Health Directorate Antimicrobial Resistance Control DepartmentDocument28 pagesAmr Concept, Causes & Response: Ministry of Health /public Health Directorate Antimicrobial Resistance Control Departmentibrahimadnan040No ratings yet
- 1 Antimicrobial ResistanceDocument27 pages1 Antimicrobial ResistanceLorenz L. Llamas IIINo ratings yet
- Responsible Use of Antimicrobials in Fish Production: GuidelinesDocument21 pagesResponsible Use of Antimicrobials in Fish Production: GuidelinesDevaraj SubramanyamNo ratings yet
- Reducing Antimicrobial Use in Food AnimalsDocument4 pagesReducing Antimicrobial Use in Food AnimalsAli RazaNo ratings yet
- Gyssen DDD MethodDocument39 pagesGyssen DDD MethodDewi RinakantiNo ratings yet
- Henson 2019Document5 pagesHenson 2019Edimar Joshua FrialaNo ratings yet
- Principles of Treatment For Tuberculosis: SoedarsonoDocument40 pagesPrinciples of Treatment For Tuberculosis: SoedarsonoLolitha JuliawandaniNo ratings yet
- Microbial Pathogenesis: SciencedirectDocument8 pagesMicrobial Pathogenesis: SciencedirectMaria Silvana AlvesNo ratings yet
- Health Service Organisation Aaw 2021 Powerpoint PresentationDocument77 pagesHealth Service Organisation Aaw 2021 Powerpoint Presentationhassan shahidNo ratings yet
- Keamanan PanganDocument50 pagesKeamanan PanganmonaNo ratings yet
- Antibiotic Guardian Leaflet FINALDocument2 pagesAntibiotic Guardian Leaflet FINALStelvin SebastianNo ratings yet
- To Protect Human, Animal, Plant & Environmental Health: We Can All Help! Take Action NowDocument2 pagesTo Protect Human, Animal, Plant & Environmental Health: We Can All Help! Take Action NowFaozan FikriNo ratings yet
- Bauer 2019Document6 pagesBauer 2019RaffaharianggaraNo ratings yet
- Global Dan Nasional Problem AMR 2019Document36 pagesGlobal Dan Nasional Problem AMR 2019DewiNo ratings yet
- Intramammary Ethno-Veterinary Formulation in Bovine Mastitis Treatment For Optimization of Antibiotic UseDocument12 pagesIntramammary Ethno-Veterinary Formulation in Bovine Mastitis Treatment For Optimization of Antibiotic Usestephimarie2004No ratings yet
- Mini-Review: Antimicrobial Resistance and COVID-19 Syndemic: Impact On Public HealthDocument6 pagesMini-Review: Antimicrobial Resistance and COVID-19 Syndemic: Impact On Public HealthJhosua MendezNo ratings yet
- AMR Pocket Guide For Ministers - ArabicDocument12 pagesAMR Pocket Guide For Ministers - ArabicAhmad Al-RusasiNo ratings yet
- The Informative Value of An Overview On Antibiotic Consumption, Treatment Efficacy and Cost of Clinical Mastitis at Farm LevelDocument8 pagesThe Informative Value of An Overview On Antibiotic Consumption, Treatment Efficacy and Cost of Clinical Mastitis at Farm LeveljsolvarelaNo ratings yet
- PTO Infeksi WidyDocument28 pagesPTO Infeksi WidyNurhasna Sushmita SariNo ratings yet
- Antibiotherapy: F-Xavier Lescure Infectious Dieases Specialist Bichat Hospital, ParisDocument13 pagesAntibiotherapy: F-Xavier Lescure Infectious Dieases Specialist Bichat Hospital, ParisRaquel HerreraNo ratings yet
- Antibiotherapy: F-Xavier Lescure Infectious Dieases Specialist Bichat Hospital, ParisDocument12 pagesAntibiotherapy: F-Xavier Lescure Infectious Dieases Specialist Bichat Hospital, ParisMth TaharNo ratings yet
- Coipars ColombiaDocument12 pagesCoipars Colombiaduverney.gaviriaNo ratings yet
- Antibacterial Chemotherapy-Theory, Problems, and Practice (Oxford University Press)Document93 pagesAntibacterial Chemotherapy-Theory, Problems, and Practice (Oxford University Press)francieudo1No ratings yet
- Instabilite MeropenemDocument9 pagesInstabilite MeropenemSonguigama CoulibalyNo ratings yet
- ANTIMICROBIAL STEWARDSHIP PROGRAM Rs TajuddinDocument46 pagesANTIMICROBIAL STEWARDSHIP PROGRAM Rs Tajuddinapotek mars farmaNo ratings yet
- Antibiotik Bijak Di RS - Dr. Ronald Irwanto Natadidjaja, SpPD-KPTI, FINASIMDocument46 pagesAntibiotik Bijak Di RS - Dr. Ronald Irwanto Natadidjaja, SpPD-KPTI, FINASIMdeviamufidazNo ratings yet
- Antimicrobial Resistance of Salmonella From Poultry Meat in Brazil Results of A Nationwide SurveyDocument8 pagesAntimicrobial Resistance of Salmonella From Poultry Meat in Brazil Results of A Nationwide SurveyMatheus SouzaNo ratings yet
- Foods 11 03894Document15 pagesFoods 11 03894Hasna NoerNo ratings yet
- Michael D. Apley, DVM, PHD: Defining Antibiotic Stewardship in Veterinary and Human Medicine For The Rest of This CenturyDocument31 pagesMichael D. Apley, DVM, PHD: Defining Antibiotic Stewardship in Veterinary and Human Medicine For The Rest of This CenturyNational Press FoundationNo ratings yet
- Antimicrobial Resistance and Clinical Use in Respiratory InfectionsDocument23 pagesAntimicrobial Resistance and Clinical Use in Respiratory InfectionsWamique IzharNo ratings yet
- Martha Mamora (Adisseo) - Munas SCI 2022Document14 pagesMartha Mamora (Adisseo) - Munas SCI 2022ifaNo ratings yet
- Veterinary Internal Medicne - 2015 - Weese - ACVIM Consensus Statement On Therapeutic Antimicrobial Use in Animals andDocument12 pagesVeterinary Internal Medicne - 2015 - Weese - ACVIM Consensus Statement On Therapeutic Antimicrobial Use in Animals andkradoNo ratings yet
- Trends in Antibiotic Therapy: Rt. Rev. Prof. C.S.S. BelloDocument47 pagesTrends in Antibiotic Therapy: Rt. Rev. Prof. C.S.S. BelloanneNo ratings yet
- Microorganisms 10 01705 v2Document22 pagesMicroorganisms 10 01705 v2Joy WinchesterNo ratings yet
- C Value ParadoxDocument18 pagesC Value ParadoxKashish GuptaNo ratings yet
- Fermentation Biotechnology PDFDocument15 pagesFermentation Biotechnology PDFsadatrafia100% (1)
- Sem 1 - EVS SyllabusDocument9 pagesSem 1 - EVS SyllabusSmitali UkeyNo ratings yet
- MAT500 Paper PhylogeneticsDocument19 pagesMAT500 Paper PhylogeneticsScottMcRaeNo ratings yet
- BINUS University: Bioinformatics Road MapDocument16 pagesBINUS University: Bioinformatics Road MapIndonesian Journal of CancerNo ratings yet
- Bacteriophages in Health and DiseaseDocument297 pagesBacteriophages in Health and DiseaseCisticola100% (1)
- Mendelian and Non Mendelian GeneticsDocument28 pagesMendelian and Non Mendelian Geneticsf_ei810% (1)
- Bioinformatics I: Lecture NotesDocument180 pagesBioinformatics I: Lecture NotesDaniela GuardiaNo ratings yet
- PHD Studentship - Development of A 3D Printed Biohybrid Lung at Loughborough UniversityDocument3 pagesPHD Studentship - Development of A 3D Printed Biohybrid Lung at Loughborough UniversityOzden IsbilirNo ratings yet
- pmTFP1 PeroxisomesDocument4 pagespmTFP1 PeroxisomesAlleleBiotechNo ratings yet
- Lziff Dgqfno: G) KFN /SF/ CG' "RL - !Document18 pagesLziff Dgqfno: G) KFN /SF/ CG' "RL - !Menuka ShresthaNo ratings yet
- Bacteria in TempeDocument7 pagesBacteria in TempeHana HananiNo ratings yet
- Pharmacodynamics of AntibioticsDocument28 pagesPharmacodynamics of AntibioticsHazimMahmoudDarwishNo ratings yet
- All Genetics FRsDocument11 pagesAll Genetics FRsPineappleHeadNo ratings yet
- Genomic Dna Isolation From Human Whole Blood Samples by Non Enzymatic Salting Out MethodDocument2 pagesGenomic Dna Isolation From Human Whole Blood Samples by Non Enzymatic Salting Out MethodamandbhaskarNo ratings yet
- YeastDocument9 pagesYeastApril Mae ArcayaNo ratings yet
- An Introduction To Photosynthesis PDFDocument15 pagesAn Introduction To Photosynthesis PDFNyimas Hoirunisa100% (2)
- Application of Column Chromatography in PharmacyDocument5 pagesApplication of Column Chromatography in PharmacyJay Shah100% (2)
- 2020 Customer Updates 1Document24 pages2020 Customer Updates 1antoniogilmoreNo ratings yet
- Study of The Hydrolysis of Sugar Cane Bagasse Using Phosphoric AcidDocument11 pagesStudy of The Hydrolysis of Sugar Cane Bagasse Using Phosphoric AcidRené MartínezNo ratings yet
- Particle Size - Mesh Conversion Chart - Powder Technology IncDocument2 pagesParticle Size - Mesh Conversion Chart - Powder Technology IncSri Ram VikasNo ratings yet
- BiotechnologyDocument39 pagesBiotechnologyannaharNo ratings yet
- Amylase ProductionDocument5 pagesAmylase ProductionPraveen RohillaNo ratings yet
- Essentials of Genetics 8th Edition by Klug Cummings Spencer and Palladino ISBN Test BankDocument14 pagesEssentials of Genetics 8th Edition by Klug Cummings Spencer and Palladino ISBN Test Banklester100% (26)
- Mep and Civil TenderDocument471 pagesMep and Civil TenderJayadevDamodaran100% (1)
- BT1001 Biology For Engineers PDFDocument2 pagesBT1001 Biology For Engineers PDFsanthi saranyaNo ratings yet
- Modul-4 - Logistik TBDocument29 pagesModul-4 - Logistik TBlusyNo ratings yet
- More DNA Evidence Against Human Chromosome FusionDocument5 pagesMore DNA Evidence Against Human Chromosome FusionAriam MariaNo ratings yet