Download as pdf or txt
You might also like
- Decision TreeDocument185 pagesDecision TreeNathan D. Croy50% (2)
- Diagnosis of Systemic Lupus ErythematosusDocument6 pagesDiagnosis of Systemic Lupus ErythematosusMuhammad Akhram ResmanaNo ratings yet
- NeuropathologyDocument66 pagesNeuropathologyKaramsi Gopinath NaikNo ratings yet
- Wacp Primary Curriculum For Psychiatry PDFDocument5 pagesWacp Primary Curriculum For Psychiatry PDFowusuesselNo ratings yet
- Lesson 2: Implementing A Curriculum Daily in The ClassroomsDocument3 pagesLesson 2: Implementing A Curriculum Daily in The ClassroomsSherwin Almojera100% (3)
- 3 Vector Worksheet PDFDocument3 pages3 Vector Worksheet PDFnabil anwar16 Anwar Year 10100% (1)
- Betahistine Used in VertigoDocument8 pagesBetahistine Used in VertigoMuhammad Faisal EffendiNo ratings yet
- 4 5827873873068033714Document1,947 pages4 5827873873068033714s.oana90No ratings yet
- Functional Neurological Disorder and Multiple SclerosisDocument10 pagesFunctional Neurological Disorder and Multiple SclerosisFrancisco Javier Fierro RestrepoNo ratings yet
- Cardio Day 3 TemplateDocument24 pagesCardio Day 3 TemplateMikeNo ratings yet
- Increased ICP: A) HeadacheDocument5 pagesIncreased ICP: A) Headachemohamed nagyNo ratings yet
- Infections PDFDocument40 pagesInfections PDFLoyla Rose100% (1)
- An Approach To Integrating Interprofessional Education in Collaborative Mental Health CareDocument6 pagesAn Approach To Integrating Interprofessional Education in Collaborative Mental Health Careanas tasyaNo ratings yet
- Antithrombotic Therapy For VTE Disease CHEST Guideline and Expert Panel ReportDocument38 pagesAntithrombotic Therapy For VTE Disease CHEST Guideline and Expert Panel ReportAdriana VasilicaNo ratings yet
- MAKING SENSE OF PSYCHIATRY: An Insecure ProfessionDocument24 pagesMAKING SENSE OF PSYCHIATRY: An Insecure ProfessionPaul Minot MDNo ratings yet
- Pharmacology (1) - 104-122Document19 pagesPharmacology (1) - 104-122Dental LecturesMMQNo ratings yet
- Alzheimer 'S Disease Profiled by Uid and Imaging Markers: Tau PET Best Predicts Cognitive DeclineDocument11 pagesAlzheimer 'S Disease Profiled by Uid and Imaging Markers: Tau PET Best Predicts Cognitive DeclineChouaib OujhainNo ratings yet
- Antipsychotics HandoutDocument25 pagesAntipsychotics HandoutTeddy Kurniady ThaherNo ratings yet
- Cranial Nerve Nuclei of Brain StemDocument6 pagesCranial Nerve Nuclei of Brain StemThanat PetchrodNo ratings yet
- Sleep Disorders (Diasomnia) : Diasomnia - Difficulties Falling Asleep or WakingDocument11 pagesSleep Disorders (Diasomnia) : Diasomnia - Difficulties Falling Asleep or Wakingfunny-arianNo ratings yet
- 01 - Pharmacotherapy Pearls For Emergency Neurological Life Support PDFDocument26 pages01 - Pharmacotherapy Pearls For Emergency Neurological Life Support PDFawinsyNo ratings yet
- Disorders of LobesDocument55 pagesDisorders of LobesdrprasantNo ratings yet
- Conversion Disorder (2018)Document12 pagesConversion Disorder (2018)Maria Von ShaftNo ratings yet
- Management of Severe Sepsis: Learning ObjectivesDocument5 pagesManagement of Severe Sepsis: Learning ObjectivesVictoriano Valiente100% (1)
- PsychopharmacologyDocument31 pagesPsychopharmacologyCon BernardinoNo ratings yet
- Reinhard L. Friede M.D. (Auth.) - Developmental Neuropathology-Springer Vienna (1975) PDFDocument535 pagesReinhard L. Friede M.D. (Auth.) - Developmental Neuropathology-Springer Vienna (1975) PDFMuhammad HabiburrahmanNo ratings yet
- AntipsychoticsDocument22 pagesAntipsychoticsvinodksahuNo ratings yet
- CV Notes PDFDocument60 pagesCV Notes PDFAnna DangNo ratings yet
- Neurotransmitter Release and ProcessDocument14 pagesNeurotransmitter Release and ProcessRain TolentinoNo ratings yet
- Chest Pain PresentationDocument24 pagesChest Pain PresentationAnonymous 17awurSUNo ratings yet
- Pharmacology Journal: Endocrine DrugsDocument50 pagesPharmacology Journal: Endocrine DrugsezezzaNo ratings yet
- Ischemic Stroke: Practice Essentials, Background, AnatomyDocument27 pagesIschemic Stroke: Practice Essentials, Background, AnatomyIndira Ulfa DunandNo ratings yet
- High Yield Topics For The Shelf - 2022 PsychDocument3 pagesHigh Yield Topics For The Shelf - 2022 PsychTonNo ratings yet
- Brain Stimulation in Psychiatry by Kellner PDFDocument1 pageBrain Stimulation in Psychiatry by Kellner PDFNajia ChoudhuryNo ratings yet
- Ect NotesDocument3 pagesEct NotesStudentNo ratings yet
- Bad Guidelines Management of Adults With Delusional InfestationDocument18 pagesBad Guidelines Management of Adults With Delusional InfestationRBGBGB RBGNo ratings yet
- Top 200 DrugsDocument4 pagesTop 200 DrugsEsther AhnNo ratings yet
- Tau Opa ThiesDocument22 pagesTau Opa ThiesIrina OdajiuNo ratings yet
- CEU Dissociative DisordersDocument63 pagesCEU Dissociative DisordersErika Louise MiChelle Cua NavasNo ratings yet
- Negative Symptoms in SchizophreniaDocument15 pagesNegative Symptoms in Schizophreniasyahrizon thomasNo ratings yet
- Concepts of Addictive Substances and Behaviours Across Time and SpaceDocument323 pagesConcepts of Addictive Substances and Behaviours Across Time and SpaceApip HilmiNo ratings yet
- Acute Ischemic Stroke: Etiology, Pathophysiology, Clinical Features, Diagnostics, TreatmentDocument7 pagesAcute Ischemic Stroke: Etiology, Pathophysiology, Clinical Features, Diagnostics, TreatmentAfrah AbdulNo ratings yet
- Cardiovascular Pharmacology: Ana Sharmaine S. Uera, MD DR PJGMRMC Anesthesiology Department 1st Year ResidentDocument68 pagesCardiovascular Pharmacology: Ana Sharmaine S. Uera, MD DR PJGMRMC Anesthesiology Department 1st Year ResidentLalay CabanagNo ratings yet
- Neet PsychiatryDocument304 pagesNeet PsychiatryASHISHNo ratings yet
- Evaluation of Fever in The Returning TravelerDocument10 pagesEvaluation of Fever in The Returning TravelerAnonymous ZUaUz1wwNo ratings yet
- Psychiatric History & MSE: Bivin JB Department of Psychiatric Nursing Mar Baselios College of NursingDocument56 pagesPsychiatric History & MSE: Bivin JB Department of Psychiatric Nursing Mar Baselios College of NursingHardeep KaurNo ratings yet
- DepressionDocument15 pagesDepressionapi-391526991No ratings yet
- PNES ClinicalApproachesDocument19 pagesPNES ClinicalApproachesClaudia100% (1)
- Lewy Body Dementias Dementia With Lewy Bodies And.9Document29 pagesLewy Body Dementias Dementia With Lewy Bodies And.9Cristina GhizdavetNo ratings yet
- Approach To A Patient With AtaxiaDocument66 pagesApproach To A Patient With AtaxiaBobeică S MihailNo ratings yet
- Stroke IskemikDocument237 pagesStroke IskemikVania ValentinaNo ratings yet
- Methylphenidate Side Effect Profile Is Influenced by Genetic Variation in The Attention-Deficit/Hyperactivity Disorder-Associated CES1 GeneDocument10 pagesMethylphenidate Side Effect Profile Is Influenced by Genetic Variation in The Attention-Deficit/Hyperactivity Disorder-Associated CES1 GeneMerari Lugo Ocaña100% (1)
- Pharmacotherapy of Alzheimers DiseaseDocument69 pagesPharmacotherapy of Alzheimers DiseaseCAROL ANN PATITICONo ratings yet
- ParkinsonDiseaseFarter2017Document103 pagesParkinsonDiseaseFarter2017DISKA YUNIAROHIMNo ratings yet
- Dual Diagnosis - Clinical and Therapeutic Aspects (Maremmani 03)Document92 pagesDual Diagnosis - Clinical and Therapeutic Aspects (Maremmani 03)antonelloveltriNo ratings yet
- Psychomotor Therapy and Psychiatry Whats in A NamDocument9 pagesPsychomotor Therapy and Psychiatry Whats in A NamBrigitte MauriNo ratings yet
- Post Stroke SyndromeDocument7 pagesPost Stroke SyndromeLilEdwiNgNo ratings yet
- Parkinson Disease Farter 2016Document91 pagesParkinson Disease Farter 2016Hsn Tuyết HàNo ratings yet
- Neurobiology of Anxiety Disorders: Michael J. Meaney, Michael R. Liebowitz, and E. David LeonardoDocument43 pagesNeurobiology of Anxiety Disorders: Michael J. Meaney, Michael R. Liebowitz, and E. David LeonardoOscar René Hernández PérezNo ratings yet
- Critical Care for Anorexia Nervosa: The MARSIPAN Guidelines in PracticeFrom EverandCritical Care for Anorexia Nervosa: The MARSIPAN Guidelines in PracticeNo ratings yet
- PsychiatryFrom EverandPsychiatryAsher B. SimonNo ratings yet
- GastroenterologyFrom EverandGastroenterologyBruce E. SandsNo ratings yet
- @MBS MedicalBooksStore 2020 HeadDocument238 pages@MBS MedicalBooksStore 2020 HeadtamiNo ratings yet
- Pharmacologic Trends of Heart Failure: Hector O. Ventura EditorDocument178 pagesPharmacologic Trends of Heart Failure: Hector O. Ventura EditortamiNo ratings yet
- Endocameleon Hopkins Telescope: Change Your Viewing Angle, Not Your EndoscopeDocument2 pagesEndocameleon Hopkins Telescope: Change Your Viewing Angle, Not Your EndoscopetamiNo ratings yet
- Journal AnestesiDocument5 pagesJournal AnestesitamiNo ratings yet
- Perioperative Management of Patients Infected With The Novel CoronavirusDocument10 pagesPerioperative Management of Patients Infected With The Novel CoronavirustamiNo ratings yet
- Posterior Axilla Sling TractioDocument5 pagesPosterior Axilla Sling TractiotamiNo ratings yet
- JournalDocument12 pagesJournaltamiNo ratings yet
- The Practice Guidelines For Primary Care of Acute Abdomen 2015Document37 pagesThe Practice Guidelines For Primary Care of Acute Abdomen 2015tamiNo ratings yet
- Risk Factors For Obstetric FisDocument9 pagesRisk Factors For Obstetric FistamiNo ratings yet
- 4 5-Appendicectomy PDFDocument12 pages4 5-Appendicectomy PDFtamiNo ratings yet
- Alvarado Score in Acute Appendicitis: Revisited: Original Research ArticleDocument4 pagesAlvarado Score in Acute Appendicitis: Revisited: Original Research ArticletamiNo ratings yet
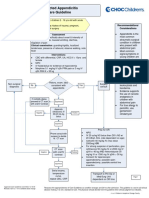
- Suspected Appendicitis Care GuidelineDocument3 pagesSuspected Appendicitis Care GuidelinetamiNo ratings yet
- Cronicon: Review Article Approach To Acute Abdomen in The Primary Health Care SettingDocument6 pagesCronicon: Review Article Approach To Acute Abdomen in The Primary Health Care SettingtamiNo ratings yet
- The Best Casinos Perform Slots in VegasvzyijDocument2 pagesThe Best Casinos Perform Slots in Vegasvzyijpumaorchid83No ratings yet
- Fei 2017Document6 pagesFei 2017PRADHAP DNo ratings yet
- Quarter1 WK 4 - WHLPLAN - ARLENE CATHERINE T. ASIA - 2021-2022Document12 pagesQuarter1 WK 4 - WHLPLAN - ARLENE CATHERINE T. ASIA - 2021-2022Bernard T. AsiaNo ratings yet
- Executive Summary: Fast Moving Consumer Goods (FMCG) '. FMCG Products Are Those That GetDocument26 pagesExecutive Summary: Fast Moving Consumer Goods (FMCG) '. FMCG Products Are Those That GetKinjal BhanushaliNo ratings yet
- MCES Envelop 1Document36 pagesMCES Envelop 1ralpdulayliboonNo ratings yet
- Python MySQL ConnectivityDocument26 pagesPython MySQL ConnectivityTaniya SwainNo ratings yet
- Jewish NumerologyDocument3 pagesJewish NumerologyDivino Henrique SantanaNo ratings yet
- Rosenbaum CJMDocument16 pagesRosenbaum CJMRamart HDNo ratings yet
- WRIT PETITION Revised and Formatted Draft 7.7.2016 2Document54 pagesWRIT PETITION Revised and Formatted Draft 7.7.2016 2Satyam PathakNo ratings yet
- R.c.c.road EstimateDocument5 pagesR.c.c.road EstimateUJJWAL SUTHARNo ratings yet
- Voting System Using Face RecognitionDocument18 pagesVoting System Using Face RecognitionbalaNo ratings yet
- Pre Bar Labor Standards 1Document165 pagesPre Bar Labor Standards 1PJ HongNo ratings yet
- Rough Draft - Project 3Document12 pagesRough Draft - Project 3api-593346566No ratings yet
- Antazo Vs DobladaDocument6 pagesAntazo Vs DobladaCel C. CaintaNo ratings yet
- Press Kit by PMH Atwater PDFDocument13 pagesPress Kit by PMH Atwater PDFAlina RadoiasNo ratings yet
- 1A Grammar Question Formation PDFDocument4 pages1A Grammar Question Formation PDFTijana CurcicNo ratings yet
- Wes Craven Interview - "The Man Who Created Freddy Krueger Is Back With Renewed Respect"Document6 pagesWes Craven Interview - "The Man Who Created Freddy Krueger Is Back With Renewed Respect"Frank LoveceNo ratings yet
- Letter From LTC Instructors of Texas To House MembersDocument3 pagesLetter From LTC Instructors of Texas To House MembersJohn CrumpNo ratings yet
- Arthur Edward Waite - The Pictorial Key To The TarotDocument111 pagesArthur Edward Waite - The Pictorial Key To The TarotFran DossinNo ratings yet
- Rune Name Letter Meaning InterpretationDocument3 pagesRune Name Letter Meaning InterpretationRiley EsaNo ratings yet
- Is BYOD Good For BusinessDocument4 pagesIs BYOD Good For BusinessNguyễn QuỳnhNo ratings yet
- Holland's RIASEC Model As An Integrative Framework For IndividualDocument18 pagesHolland's RIASEC Model As An Integrative Framework For IndividualNorashady Mohd NoorNo ratings yet
- Электрические схемы 2005 год LRL 21 38 53 501Document249 pagesЭлектрические схемы 2005 год LRL 21 38 53 501Dmitrii Panasiuk100% (1)
- General System TheoryDocument307 pagesGeneral System TheoryCarlos Luiz100% (3)
- Carlos Runcie-Tanaka: The Passion and Pulse of ClayDocument4 pagesCarlos Runcie-Tanaka: The Passion and Pulse of ClayScolli Huaranga GalarzaNo ratings yet
- Heroes Are Made Not BornDocument2 pagesHeroes Are Made Not BornYoong iiNo ratings yet
- Worksheet For Chris Bailey Hyperfocus Secrets For Better Productivity Episode 247Document12 pagesWorksheet For Chris Bailey Hyperfocus Secrets For Better Productivity Episode 247Abigail LorenzanaNo ratings yet
- A Longitudinal Study of Team Conflict PPR 1Document4 pagesA Longitudinal Study of Team Conflict PPR 1shahbaz sheikhNo ratings yet