Download as pdf or txt
You might also like
- Theater in SocietyDocument13 pagesTheater in SocietyPaul Sargei AzurinNo ratings yet
- Adult Placement Test: Scegli L'alternativa Corretta Per Completare Gli SpaziDocument2 pagesAdult Placement Test: Scegli L'alternativa Corretta Per Completare Gli SpaziGanchimeg Shiirev100% (1)
- (Eduard M. Bazelyan, Yuri P. Raizer) LightningDocument328 pages(Eduard M. Bazelyan, Yuri P. Raizer) LightningJavier SanchezNo ratings yet
- CCROPP Best Pract Obesity Prev TMT PDFDocument288 pagesCCROPP Best Pract Obesity Prev TMT PDFharunnuranNo ratings yet
- Detection of Pathogenic Bacteria From Septic Patients Using 16s Ribosomal RNA Gene-Targeted Metagenomic SequencingDocument8 pagesDetection of Pathogenic Bacteria From Septic Patients Using 16s Ribosomal RNA Gene-Targeted Metagenomic Sequencingfaraz.mirza1No ratings yet
- Rannikko Et Al-2018-Journal of Internal MedicineDocument9 pagesRannikko Et Al-2018-Journal of Internal MedicineFelipe MNo ratings yet
- Hemodialysis Catheter-Related Bloodstream InfectionsDocument7 pagesHemodialysis Catheter-Related Bloodstream InfectionsHGZ 83 MoreliaNo ratings yet
- Liquid Biopsy: Is There An Advantage To Analyzing Circulating Exosomal Dna Compared To Cfdna or Are They The Same?Document4 pagesLiquid Biopsy: Is There An Advantage To Analyzing Circulating Exosomal Dna Compared To Cfdna or Are They The Same?Muhammad Javed GabaNo ratings yet
- 2017 HepatologyDocument148 pages2017 HepatologyrdLuis1No ratings yet
- CP Final KeynoteDocument20 pagesCP Final KeynoteLiana Ysabelle CasusiNo ratings yet
- 2018 Article 3308Document10 pages2018 Article 3308Maisyaroh SaragihNo ratings yet
- Captura de Tela 2024-03-27 À(s) 14.15.05Document7 pagesCaptura de Tela 2024-03-27 À(s) 14.15.05Tamiris SantanaNo ratings yet
- Limitation Graft BiopsyDocument11 pagesLimitation Graft BiopsyWEE LENG GANNo ratings yet
- Cureus 0012 00000007812Document6 pagesCureus 0012 00000007812taufik.abdiNo ratings yet
- COVID-19 y Parametros de CoagulacionDocument4 pagesCOVID-19 y Parametros de CoagulacionSMIBA MedicinaNo ratings yet
- Ipp 6 E08Document6 pagesIpp 6 E08retnoNo ratings yet
- A Stabilizing Reagent Prevents Cell-Free DNA ContaDocument6 pagesA Stabilizing Reagent Prevents Cell-Free DNA ContaEdsel SiababaNo ratings yet
- 2019-Circulating Tumor DNA For Early Cancer DetectionDocument14 pages2019-Circulating Tumor DNA For Early Cancer Detectionvivitri.dewiNo ratings yet
- D'alessandro 2020Document5 pagesD'alessandro 2020Flip Flop ChartNo ratings yet
- Procalcitonin Is It The End of Road To Sepsis Diagnosis - February - 2022 - 6546541022 - 2629943Document2 pagesProcalcitonin Is It The End of Road To Sepsis Diagnosis - February - 2022 - 6546541022 - 2629943RateeshNo ratings yet
- Pum1 and Rnase P Genes As Potential Cell-Free Dna Markers inDocument10 pagesPum1 and Rnase P Genes As Potential Cell-Free Dna Markers inArissa KohataNo ratings yet
- Procalcitonin Levels in Surgical Patients at Risk of CandidemiaDocument6 pagesProcalcitonin Levels in Surgical Patients at Risk of CandidemiaKeziaNo ratings yet
- JCM 09 01543 v2Document16 pagesJCM 09 01543 v2Flip Flop ChartNo ratings yet
- Flowcytometry Dna Analysis in CancerDocument36 pagesFlowcytometry Dna Analysis in CancerAstri Arri FebriantiNo ratings yet
- The Challenge of Kidney Damage During Interventional Cardiology ProceduresDocument6 pagesThe Challenge of Kidney Damage During Interventional Cardiology ProceduresIJAR JOURNALNo ratings yet
- Ijbsv 16 P 1551Document12 pagesIjbsv 16 P 1551Flip Flop ChartNo ratings yet
- Blastic Plasmacytoid Dendritic Cell NeoplasmeCurrent InsightsDocument10 pagesBlastic Plasmacytoid Dendritic Cell NeoplasmeCurrent InsightsPaúl Otañez MolinaNo ratings yet
- A 6 mRNA Host Response Classifier in Whole Blood Predicts Outcomes in COVID 19 and Other Acute Viral InfectionsDocument16 pagesA 6 mRNA Host Response Classifier in Whole Blood Predicts Outcomes in COVID 19 and Other Acute Viral Infectionsbrhpcn2rrfNo ratings yet
- Presepsin Values As Markers of Severity of SepsisDocument7 pagesPresepsin Values As Markers of Severity of Sepsisfaraz.mirza1No ratings yet
- Accepted Manuscript: Impact of Pre-Transplant Donor BK Viruria in Kidney Transplant RecipientsDocument23 pagesAccepted Manuscript: Impact of Pre-Transplant Donor BK Viruria in Kidney Transplant RecipientsMarianaNo ratings yet
- Kidney Biopsy Findings in Patients With COVID-19 2020Document10 pagesKidney Biopsy Findings in Patients With COVID-19 2020Glenda DuarteNo ratings yet
- CrisperDocument9 pagesCrispertanviaggrawalNo ratings yet
- Delta Neutrophil Index As An Early MDocument9 pagesDelta Neutrophil Index As An Early MFariz NurNo ratings yet
- Biomolecular Detection and Quantification: SciencedirectDocument23 pagesBiomolecular Detection and Quantification: SciencedirectSYED MAAZ TARIQNo ratings yet
- 2020 July - Clinical, Radiological and Laboratory Characteristics and Risk Factors For Severity and Mortality of 289 Hospitalized COVID-19 PatientsDocument18 pages2020 July - Clinical, Radiological and Laboratory Characteristics and Risk Factors For Severity and Mortality of 289 Hospitalized COVID-19 PatientspoopooheadNo ratings yet
- DetectionDocument9 pagesDetectionHarshvardhan RavalNo ratings yet
- The Research of The Application of A New Urinary BDocument7 pagesThe Research of The Application of A New Urinary BNealNo ratings yet
- Identification of A 14-Lncrna Signature and Construction of A Prognostic Nomogram Predicting Overall Survival of Gastric CancerDocument14 pagesIdentification of A 14-Lncrna Signature and Construction of A Prognostic Nomogram Predicting Overall Survival of Gastric CancerAriani ArinNo ratings yet
- Novel Blood and Tissue-Based Mitochondrial D-Loop Mutations Detected2Document8 pagesNovel Blood and Tissue-Based Mitochondrial D-Loop Mutations Detected2bdanaei75No ratings yet
- Circulating Tumor DNA and Radiological Tumor VolumDocument7 pagesCirculating Tumor DNA and Radiological Tumor Volumnaomireyes01No ratings yet
- Braz Jr. Infect Dis 2021Document4 pagesBraz Jr. Infect Dis 2021cdsaludNo ratings yet
- Neutrophil Dysfunction, Immature Granulocytes, and Cell-FreeDocument9 pagesNeutrophil Dysfunction, Immature Granulocytes, and Cell-Freei chen chenNo ratings yet
- Gastroenterology: World Journal ofDocument14 pagesGastroenterology: World Journal ofrahul krishnanNo ratings yet
- Persistence of Zika Virus in Body Fluids - Final Report: Original ArticleDocument10 pagesPersistence of Zika Virus in Body Fluids - Final Report: Original ArticleGalo Eduardo Acosta Oleas 1716247414No ratings yet
- The Incidence of Leukemia and Mortality From Sepsis in Patients With Severe Congenital Neutropenia Receiving Long-Term G-CSF TherapyDocument9 pagesThe Incidence of Leukemia and Mortality From Sepsis in Patients With Severe Congenital Neutropenia Receiving Long-Term G-CSF TherapyqqqqwerrataNo ratings yet
- Silva-Filho Et Al. 2014Document7 pagesSilva-Filho Et Al. 2014azyytieNo ratings yet
- 48497487development of A Real-Time PCR Assay For20160901-31954-5rom1y-Libre - pdf147277084Document6 pages48497487development of A Real-Time PCR Assay For20160901-31954-5rom1y-Libre - pdf147277084milixza botacioNo ratings yet
- Predictive Accuracy of The Quick Sepsis-Related Organ Failure Assessment Score in Brazil: A Prospective Multicenter StudyDocument10 pagesPredictive Accuracy of The Quick Sepsis-Related Organ Failure Assessment Score in Brazil: A Prospective Multicenter StudyAlexandre CavalcantiNo ratings yet
- PCR-based Sepsis@ Quick Test Is Superior in Comparison With Blood Culture For Identification of Sepsis-Causative PathogensDocument7 pagesPCR-based Sepsis@ Quick Test Is Superior in Comparison With Blood Culture For Identification of Sepsis-Causative Pathogensfaraz.mirza1No ratings yet
- Fcell 09 661272Document11 pagesFcell 09 661272Bikash Ranjan SamalNo ratings yet
- International Journal of Infectious Diseases: Dougbeh-Chris Nyan, Kevin L. SwinsonDocument7 pagesInternational Journal of Infectious Diseases: Dougbeh-Chris Nyan, Kevin L. SwinsonapalanavedNo ratings yet
- 1 s2.0 S009042951930963X Main PDFDocument8 pages1 s2.0 S009042951930963X Main PDFCris FischerNo ratings yet
- Suspected of Genetic Alterations of Germinal Origin in Liquid BiopsyDocument30 pagesSuspected of Genetic Alterations of Germinal Origin in Liquid BiopsyanttihakliNo ratings yet
- Diagnostic Yield of Cytopathology in Evaluating Pericardial Effusions: Clinicopathologic Analysis of 419 SpecimensDocument10 pagesDiagnostic Yield of Cytopathology in Evaluating Pericardial Effusions: Clinicopathologic Analysis of 419 SpecimensAnca CucuNo ratings yet
- Appearances Can Be DeceivingDocument5 pagesAppearances Can Be DeceivingRoger TNo ratings yet
- W Biod05Document13 pagesW Biod05Эма СэмNo ratings yet
- Tang Et Al. - 2020 - Abnormal Coagulation Parameters Are Associated With Poor Prognosis in Patients With Novel Coronavirus PneumoniaDocument4 pagesTang Et Al. - 2020 - Abnormal Coagulation Parameters Are Associated With Poor Prognosis in Patients With Novel Coronavirus PneumoniaAlexandre Campos Moraes AmatoNo ratings yet
- RequestedDocument9 pagesRequestedGaurav MauryaNo ratings yet
- DeteksionDocument9 pagesDeteksionkasandraharahapNo ratings yet
- 2020 07 16 20153916v1 FullDocument11 pages2020 07 16 20153916v1 Fullangel.paternina423No ratings yet
- Schell 2012Document9 pagesSchell 2012PUPUT PUJIANTINo ratings yet
- 39 12 1861Document5 pages39 12 1861calixto hernandezNo ratings yet
- Jurnal 7Document4 pagesJurnal 7Ariqa AzzhraNo ratings yet
- Fast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeFrom EverandFast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeNo ratings yet
- Olsen 2016Document9 pagesOlsen 2016Felipe MNo ratings yet
- Hoye 2018Document11 pagesHoye 2018Felipe MNo ratings yet
- BSR 39 bsr20181335 PDFDocument11 pagesBSR 39 bsr20181335 PDFFelipe MNo ratings yet
- Tavakolpour 2018Document8 pagesTavakolpour 2018Felipe MNo ratings yet
- Regev 2018Document9 pagesRegev 2018Felipe MNo ratings yet
- Torabi 2018Document9 pagesTorabi 2018Felipe MNo ratings yet
- Groen 2018Document12 pagesGroen 2018Felipe MNo ratings yet
- Para Leitura 4Document9 pagesPara Leitura 4Felipe MNo ratings yet
- Para Leitura 3Document12 pagesPara Leitura 3Felipe MNo ratings yet
- Lehmann Werman 2016Document9 pagesLehmann Werman 2016Felipe MNo ratings yet
- Neurology2018881847 PDFDocument9 pagesNeurology2018881847 PDFFelipe MNo ratings yet
- Unique RNA Signature of Different Lesion Types in The Brain White Matter in Progressive Multiple SclerosisDocument17 pagesUnique RNA Signature of Different Lesion Types in The Brain White Matter in Progressive Multiple SclerosisFelipe MNo ratings yet
- Kappa Free Light Chains Is A Valid Tool in The Diagnostics of MS: A Large Multicenter StudyDocument12 pagesKappa Free Light Chains Is A Valid Tool in The Diagnostics of MS: A Large Multicenter StudyFelipe MNo ratings yet
- 10.1007@s00415 018 9106 2 PDFDocument7 pages10.1007@s00415 018 9106 2 PDFFelipe MNo ratings yet
- 10 1111@ane 13078 PDFDocument17 pages10 1111@ane 13078 PDFFelipe MNo ratings yet
- Rannikko Et Al-2018-Journal of Internal MedicineDocument9 pagesRannikko Et Al-2018-Journal of Internal MedicineFelipe MNo ratings yet
- Mirna Contributions To Pediatric-Onset Multiple Sclerosis Inferred From GwasDocument9 pagesMirna Contributions To Pediatric-Onset Multiple Sclerosis Inferred From GwasFelipe MNo ratings yet
- 10 1016@j Msard 2019 02 004 PDFDocument25 pages10 1016@j Msard 2019 02 004 PDFFelipe MNo ratings yet
- 10 1016@j Jns 2019 06 022Document5 pages10 1016@j Jns 2019 06 022Felipe MNo ratings yet
- Microbial Pathogenesis: SciencedirectDocument8 pagesMicrobial Pathogenesis: SciencedirectFelipe MNo ratings yet
- 1 s2.0 S1011134408001784 Main PDFDocument7 pages1 s2.0 S1011134408001784 Main PDFFelipe MNo ratings yet
- Lncrnas Associated With Multiple Sclerosis Expressed in The Th1 Cell LineageDocument10 pagesLncrnas Associated With Multiple Sclerosis Expressed in The Th1 Cell LineageFelipe MNo ratings yet
- AldunateDocument23 pagesAldunateFelipe MNo ratings yet
- JOI160156supp1 Prod PDFDocument18 pagesJOI160156supp1 Prod PDFFelipe MNo ratings yet
- 2018 72 Moesm1 Esm PDFDocument33 pages2018 72 Moesm1 Esm PDFFelipe MNo ratings yet
- Biochemical and Biophysical Research Communications: Christin Fischer, Thomas KleinschmidtDocument5 pagesBiochemical and Biophysical Research Communications: Christin Fischer, Thomas KleinschmidtFelipe MNo ratings yet
- Michael SC Conlon, Joseph M Caswell, Stacey A Santi, Barbara Ballantyne, Margaret L Meigs, Andrew Knight, Craig C Earle and Mark HartmanDocument10 pagesMichael SC Conlon, Joseph M Caswell, Stacey A Santi, Barbara Ballantyne, Margaret L Meigs, Andrew Knight, Craig C Earle and Mark HartmanFelipe MNo ratings yet
- Antimicrob. Agents Chemother. 2009 Llarrull 4051 63Document13 pagesAntimicrob. Agents Chemother. 2009 Llarrull 4051 63Felipe MNo ratings yet
- The Vaginal Microbiome, Vaginal Anti-Microbial Defence Mechanisms and The Clinical Challenge of Reducing Infection-Related Preterm BirthDocument6 pagesThe Vaginal Microbiome, Vaginal Anti-Microbial Defence Mechanisms and The Clinical Challenge of Reducing Infection-Related Preterm BirthFelipe MNo ratings yet
- Solar Disinfection of Water For Diarrhoeal Prevention in Southern IndiaDocument4 pagesSolar Disinfection of Water For Diarrhoeal Prevention in Southern IndiaFelipe MNo ratings yet
- Salaria v. Buenviaje G.R. No. L 45642 DIGESTDocument2 pagesSalaria v. Buenviaje G.R. No. L 45642 DIGESTMikee BornforThis MirasolNo ratings yet
- 4 Ways To Strengthen Our Relationship With GodDocument5 pages4 Ways To Strengthen Our Relationship With GodDanNo ratings yet
- Chapter 1: The Study of Accounting Information SystemsDocument36 pagesChapter 1: The Study of Accounting Information SystemsAliah CyrilNo ratings yet
- Wealth of Nations QuestionsDocument3 pagesWealth of Nations QuestionssantanaNo ratings yet
- RIOSA v. TabacoDocument3 pagesRIOSA v. Tabacochappy_leigh118No ratings yet
- How One Ought To LiveDocument4 pagesHow One Ought To LiveVictor HoustonNo ratings yet
- December 06Document36 pagesDecember 06Quy DangNo ratings yet
- UntitledDocument1 pageUntitledErwinNo ratings yet
- Course Catalogue: Robot Programming and MaintenanceDocument18 pagesCourse Catalogue: Robot Programming and MaintenanceClaudiu RaduNo ratings yet
- Lavendia Portfolio PR2 ABM12 4Document28 pagesLavendia Portfolio PR2 ABM12 4PresydenteNo ratings yet
- Labour Court of LesothoDocument10 pagesLabour Court of LesothoAndré Le RouxNo ratings yet
- Material Safety Data SheetDocument12 pagesMaterial Safety Data SheetDEEP PATELNo ratings yet
- Cold Mail Samples For Non-STEM GraduatesDocument8 pagesCold Mail Samples For Non-STEM GraduatesKifayat HussainNo ratings yet
- The First Term English Exam Level: 3am Duration:1h30 TextDocument2 pagesThe First Term English Exam Level: 3am Duration:1h30 Textaicha yayoucheNo ratings yet
- PE 2 (Rhythmic (SyllabusDocument2 pagesPE 2 (Rhythmic (SyllabusJoseph MazoNo ratings yet
- Dashamgranth ChhandasDocument12 pagesDashamgranth ChhandassomapriyNo ratings yet
- KCC Application Form 1Document14 pagesKCC Application Form 1ashish trivediNo ratings yet
- St. Paul Lutheran Church: From The Pastor's Desk StudyDocument7 pagesSt. Paul Lutheran Church: From The Pastor's Desk Studyapi-26565051No ratings yet
- Unity and Diversity in New Testament TheologyDocument9 pagesUnity and Diversity in New Testament Theologyseth Effah hillNo ratings yet
- DLL 9 3rd w1Document4 pagesDLL 9 3rd w1Ramon FrejasNo ratings yet
- Capital Budgeting: Financial ManagementDocument22 pagesCapital Budgeting: Financial ManagementKaRin MerRoNo ratings yet
- Group 3 - Written ReportDocument12 pagesGroup 3 - Written ReportMarielle AnneNo ratings yet
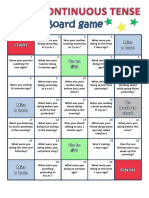
- Past Continuous Board GameDocument1 pagePast Continuous Board GameAngélica Cetina100% (1)
- Eu 4Document21 pagesEu 4Guy SajerNo ratings yet
- Artists & Illustrators - 2016-01 PDFDocument84 pagesArtists & Illustrators - 2016-01 PDFheraasku7194100% (4)
- G.R. No. 207950, September 22, 2014Document8 pagesG.R. No. 207950, September 22, 2014Amicus CuriaeNo ratings yet