Download as pdf or txt
You might also like
- Reading Test 01 - E2Lang PDFDocument25 pagesReading Test 01 - E2Lang PDFMuhammad Haneef100% (12)
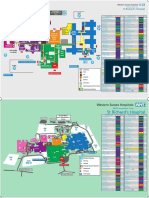
- ST Richards Floor PlanDocument2 pagesST Richards Floor PlanMarc33% (3)
- Guidelines For Inpatient Pharmacy PracticeDocument68 pagesGuidelines For Inpatient Pharmacy PracticeAmir Ihsan100% (1)
- ERC ALS Lecture 1 IntroductionDocument10 pagesERC ALS Lecture 1 IntroductioniamyourgasmanNo ratings yet
- Biology ProjectDocument12 pagesBiology Projectapi-380313126100% (2)
- The Effect of Depression On College Students Academic Performance FinalDocument3 pagesThe Effect of Depression On College Students Academic Performance FinalIvy Jean Ybera-PapasinNo ratings yet
- External Auditory Canal Osteoma A Case ReportDocument4 pagesExternal Auditory Canal Osteoma A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Unusual Presentation of Adamantinoma With Synchronous 2024 International JouDocument5 pagesUnusual Presentation of Adamantinoma With Synchronous 2024 International JouRonald QuezadaNo ratings yet
- Ijohns 2018081616134070Document5 pagesIjohns 2018081616134070alifaNo ratings yet
- Recurrent Aneurysmal Bone Cyst of The Mandibular Condyle With Soft Tissue ExtensionDocument5 pagesRecurrent Aneurysmal Bone Cyst of The Mandibular Condyle With Soft Tissue ExtensionlalajanNo ratings yet
- International Journal of Surgery Case ReportsDocument4 pagesInternational Journal of Surgery Case ReportsElisabeth TikalakaNo ratings yet
- A Case of Synovial Hemangioma of The KneeDocument5 pagesA Case of Synovial Hemangioma of The KneeAnjana g rNo ratings yet
- 1 s2.0 S1878875018300159 MainDocument9 pages1 s2.0 S1878875018300159 MainAlexandreNo ratings yet
- Endoskopik 2.brankialDocument5 pagesEndoskopik 2.brankialDogukan DemirNo ratings yet
- A Rare Case of Myopericytoma of The Base of Right Index Finger Managed With en Bloc ExcisionDocument2 pagesA Rare Case of Myopericytoma of The Base of Right Index Finger Managed With en Bloc ExcisionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Resection of Sinonasal Hemangiopericytoma Through Transnasal Endoscopic MethodDocument5 pagesResection of Sinonasal Hemangiopericytoma Through Transnasal Endoscopic MethodInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Article in Press: Journal of Oral and Maxillofacial Surgery, Medicine, and PathologyDocument6 pagesArticle in Press: Journal of Oral and Maxillofacial Surgery, Medicine, and PathologyOMFS FKG UnimusNo ratings yet
- Intradiploic Meningioma of The Orbit A Case ReportDocument3 pagesIntradiploic Meningioma of The Orbit A Case ReportNurzulifa 15 104No ratings yet
- 0610case1 Metastatic MelanomaDocument4 pages0610case1 Metastatic MelanomawillygopeNo ratings yet
- reverse posterior interosseous flap 2Document7 pagesreverse posterior interosseous flap 2Cleff FlowersNo ratings yet
- Case Report: Iatrogenic Intraspinal Epidermoid CystDocument3 pagesCase Report: Iatrogenic Intraspinal Epidermoid CystWilda HanimNo ratings yet
- Median Sternotomy ProcedureDocument5 pagesMedian Sternotomy ProcedureNelly NehNo ratings yet
- 10 1016@j Jormas 2018 04 017Document19 pages10 1016@j Jormas 2018 04 017María Fernanda EstévezNo ratings yet
- Maxillary Sinus Osteoma: Two Cases and Review of The LiteratureDocument5 pagesMaxillary Sinus Osteoma: Two Cases and Review of The LiteraturelibraNo ratings yet
- Cavernous Hemangioma PDFDocument2 pagesCavernous Hemangioma PDFChristian WilliamNo ratings yet
- TN 2Document5 pagesTN 2faty basalamahNo ratings yet
- Early Outcome After The Use of The Triceps Fascia Flap in Interposition Elbow Arthroplasty A Novel Method in The Treatment of Post-Traumatic Elbow StiffnessDocument6 pagesEarly Outcome After The Use of The Triceps Fascia Flap in Interposition Elbow Arthroplasty A Novel Method in The Treatment of Post-Traumatic Elbow StiffnessJohannes CordeNo ratings yet
- Arthroscopy of The Inferior Compartment of The Temporomandibular Joint - A New PerspectiveDocument5 pagesArthroscopy of The Inferior Compartment of The Temporomandibular Joint - A New PerspectiveFatima Karoline DultraNo ratings yet
- 17 Lopez MartinDocument4 pages17 Lopez MartinAmber KhokharNo ratings yet
- Painful Knee 2024 International Journal of Surgery Case ReportsDocument6 pagesPainful Knee 2024 International Journal of Surgery Case ReportsRonald QuezadaNo ratings yet
- A Case Report of A Drop Foot Developed After Common Femoral Artery Cannulation For Venoarterial Extracorporeal Membrane OxygenationDocument4 pagesA Case Report of A Drop Foot Developed After Common Femoral Artery Cannulation For Venoarterial Extracorporeal Membrane OxygenationAnon0123No ratings yet
- Embolización Angiografica ArtDocument5 pagesEmbolización Angiografica ArtIsamar AlvarezNo ratings yet
- Toetva BrazilDocument6 pagesToetva BrazildenoanandiNo ratings yet
- Bilateral Peroneal Tubercle Osteochondroma of The Calcaneus: CaseDocument3 pagesBilateral Peroneal Tubercle Osteochondroma of The Calcaneus: CaseAntony CevallosNo ratings yet
- What Should We Be Careful of Ankle Arthroscopy?: or Thopaedic Surger yDocument9 pagesWhat Should We Be Careful of Ankle Arthroscopy?: or Thopaedic Surger yJaysellePuguonTabijeNo ratings yet
- 1 s2.0 S2210261217304431 MainDocument4 pages1 s2.0 S2210261217304431 MainChristopher BermeoNo ratings yet
- Surgical Removal of Spinal Tumors: Article by James Willey, Cst/Cfa, and Mark V. Iarkins, M DDocument8 pagesSurgical Removal of Spinal Tumors: Article by James Willey, Cst/Cfa, and Mark V. Iarkins, M DLuwiNo ratings yet
- Osteoma NepalDocument5 pagesOsteoma NepalRafael Lemos de SouzaNo ratings yet
- Interstitial Incisional Hernia Following Appendectomy: Case ReportDocument2 pagesInterstitial Incisional Hernia Following Appendectomy: Case ReportSCJUBv Chirurgie INo ratings yet
- Treatment of Large Recurrent Aneurysmal Bone Cysts of Mandible: Transosseous Intralesional Embolization As An Adjunct To ResectionDocument6 pagesTreatment of Large Recurrent Aneurysmal Bone Cysts of Mandible: Transosseous Intralesional Embolization As An Adjunct To ResectionlalajanNo ratings yet
- Management of Non-Metastatic Pelvic Bone Giant Cell Tumour by Resection, Extended Curettage and Reconstruction With Autograft and Allograft - A Case ReportDocument5 pagesManagement of Non-Metastatic Pelvic Bone Giant Cell Tumour by Resection, Extended Curettage and Reconstruction With Autograft and Allograft - A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Manenti (2016) - Internal Thoracic Artery HistologyDocument4 pagesManenti (2016) - Internal Thoracic Artery HistologyVanessaNo ratings yet
- Intracranial Epidermoid CystDocument3 pagesIntracranial Epidermoid CystWildaHanimNo ratings yet
- Fulltext - Smjo v3 1059Document3 pagesFulltext - Smjo v3 1059Rachell AchellNo ratings yet
- J.Operative Approaches To The Pineal Region Tumors.1998Document4 pagesJ.Operative Approaches To The Pineal Region Tumors.1998Kysy CodonNo ratings yet
- Koh 2014Document6 pagesKoh 2014Ayan KusariNo ratings yet
- Osteoid Osteoma: CT-guided Radiofrequency Ablation: Original StudyDocument6 pagesOsteoid Osteoma: CT-guided Radiofrequency Ablation: Original StudyNurul FatimahNo ratings yet
- Hand Tumours: Allens TestDocument74 pagesHand Tumours: Allens TestfiestaNo ratings yet
- AmputationDocument16 pagesAmputationElmeldah TwaraNo ratings yet
- EDAMS Nota Tecnica GoodDocument4 pagesEDAMS Nota Tecnica GoodnaimNo ratings yet
- 9Document7 pages9Soal KoasNo ratings yet
- Regional Anesthesia and Eye SurgeryDocument7 pagesRegional Anesthesia and Eye SurgeryharumNo ratings yet
- The Septum Inguinalis: A Clue To Hernia Genesis?: Journal of Investigative SurgeryDocument10 pagesThe Septum Inguinalis: A Clue To Hernia Genesis?: Journal of Investigative SurgeryTeja LaksanaNo ratings yet
- Tracheobronchial Injuries. Conservative TreatmenTDocument5 pagesTracheobronchial Injuries. Conservative TreatmenTTaufik Gumilar WahyudinNo ratings yet
- Minimal Invasive Surgery in Head andDocument12 pagesMinimal Invasive Surgery in Head andArchanaShenoyNo ratings yet
- A New Technique For Reconstructions of LDocument19 pagesA New Technique For Reconstructions of LHenrique NetoNo ratings yet
- Minor Ipsilateral Simple Limbal Epithelial Transplantation (mini-SLET) For Pterygium TreatmentDocument3 pagesMinor Ipsilateral Simple Limbal Epithelial Transplantation (mini-SLET) For Pterygium TreatmentChandra Wulan Heningtyas PriyakusumaNo ratings yet
- Acta Orthopaedica Et Traumatologica Turcica: C. Sahin, Y. Oc, N. Ediz, M. Alt Inay, A.H. BayrakDocument6 pagesActa Orthopaedica Et Traumatologica Turcica: C. Sahin, Y. Oc, N. Ediz, M. Alt Inay, A.H. BayrakPoji RazaliNo ratings yet
- Ameloblast PerifericoDocument4 pagesAmeloblast Perifericofernanda tragolafNo ratings yet
- Medial Orbital Epidermoid Cyst: Case ReportDocument3 pagesMedial Orbital Epidermoid Cyst: Case ReportTeodorNo ratings yet
- Morbitity of Bicoronal FlapsDocument8 pagesMorbitity of Bicoronal Flapsmehul7patel-10No ratings yet
- Epithelioid Hemangioendothelioma of The Infundibular-Hypothalamic Region: Case Report and Literature ReviewDocument6 pagesEpithelioid Hemangioendothelioma of The Infundibular-Hypothalamic Region: Case Report and Literature ReviewcarlosNo ratings yet
- 1 s2.0 S2210261217306788 MainDocument4 pages1 s2.0 S2210261217306788 Mainnandaaa aprilNo ratings yet
- Minimally Invasive Approach For Extraforaminal Synovial Cyst L5-S1Document7 pagesMinimally Invasive Approach For Extraforaminal Synovial Cyst L5-S1Tatiana RoaNo ratings yet
- 4 Meningoencefalocele PDFDocument4 pages4 Meningoencefalocele PDFOmar Lopez ArbolayNo ratings yet
- Surgery of the Cranio-Vertebral JunctionFrom EverandSurgery of the Cranio-Vertebral JunctionEnrico TessitoreNo ratings yet
- Nej MP 2302676Document3 pagesNej MP 2302676anggiNo ratings yet
- Psychometrical Properties of The Turkish Transla 2019 Acta Orthopaedica Et TDocument5 pagesPsychometrical Properties of The Turkish Transla 2019 Acta Orthopaedica Et TanggiNo ratings yet
- Nej MC 2200133Document3 pagesNej MC 2200133anggiNo ratings yet
- Many Authors in Business Management Research Papers Wrongly Calculate Central Tendency Just Like Wang Et Al. (2019) - This Leads To A Disaster.Document6 pagesMany Authors in Business Management Research Papers Wrongly Calculate Central Tendency Just Like Wang Et Al. (2019) - This Leads To A Disaster.Scholarly CriticismNo ratings yet
- In Search of A Better Equation - Performance and Equity in Estimates of Kidney FunctionDocument4 pagesIn Search of A Better Equation - Performance and Equity in Estimates of Kidney FunctionanggiNo ratings yet
- Acta Orthopaedica Et Traumatologica Turcica: Cemil Ozal, Gonca Ari, Mintaze Kerem GunelDocument4 pagesActa Orthopaedica Et Traumatologica Turcica: Cemil Ozal, Gonca Ari, Mintaze Kerem GunelanggiNo ratings yet
- Mid Term Results With An Anatomic Stemless Shoulde 2019 Acta Orthopaedica EtDocument5 pagesMid Term Results With An Anatomic Stemless Shoulde 2019 Acta Orthopaedica EtanggiNo ratings yet
- Superficial Radial Nerve Compression Due To Fibrom 2019 Acta Orthopaedica EtDocument3 pagesSuperficial Radial Nerve Compression Due To Fibrom 2019 Acta Orthopaedica EtanggiNo ratings yet
- Gastrointestinal Nursing Volume 7 Issue 1 2009 (Doi 10.12968/gasn.2009.7.1.39369) Cox, Carol Steggall, Martin - A Step By-Step Guide To Performing A Complete Abdominal ExaminationDocument7 pagesGastrointestinal Nursing Volume 7 Issue 1 2009 (Doi 10.12968/gasn.2009.7.1.39369) Cox, Carol Steggall, Martin - A Step By-Step Guide To Performing A Complete Abdominal ExaminationanggiNo ratings yet
- Nej MSR 1707974Document5 pagesNej MSR 1707974anggiNo ratings yet
- Nej Mic M 1701787Document1 pageNej Mic M 1701787anggiNo ratings yet
- A Woman Considering Contralateral Prophylactic MastectomyDocument4 pagesA Woman Considering Contralateral Prophylactic MastectomyanggiNo ratings yet
- Nej Mic M 1703542Document1 pageNej Mic M 1703542anggiNo ratings yet
- Health, Wealth, and The U.S. Senate: EditorialDocument2 pagesHealth, Wealth, and The U.S. Senate: EditorialanggiNo ratings yet
- Nej MC 1709128Document3 pagesNej MC 1709128anggiNo ratings yet
- Nej MR A 1512592Document8 pagesNej MR A 1512592anggiNo ratings yet
- Nej MP 1700713Document3 pagesNej MP 1700713anggiNo ratings yet
- The Maternal Health Compact: Rural Health C AreDocument2 pagesThe Maternal Health Compact: Rural Health C AreanggiNo ratings yet
- A Case Study On Colon MassDocument29 pagesA Case Study On Colon MassDahlia D. SuelloNo ratings yet
- Nursing Care Management of Client With Hypokalemia ACTUAL 1Document4 pagesNursing Care Management of Client With Hypokalemia ACTUAL 1Angel Nieto PengsonNo ratings yet
- Heart Lung MachineDocument20 pagesHeart Lung MachineDeepak DennisonNo ratings yet
- Eportfolio Resume CVDocument4 pagesEportfolio Resume CVapi-577441503No ratings yet
- PHYSIOTHERAPY BELLS PALSY (Dr.L.RAMADASS - PT 9500333960)Document62 pagesPHYSIOTHERAPY BELLS PALSY (Dr.L.RAMADASS - PT 9500333960)Ram DeekshaNo ratings yet
- Decaf Coffee - Good or BadDocument5 pagesDecaf Coffee - Good or BadAdam70sdNo ratings yet
- Introduction To STYEDocument10 pagesIntroduction To STYESumit KumarNo ratings yet
- Imci 1Document90 pagesImci 1Miguel Vergel100% (1)
- Action Plan UPDATEDDocument2 pagesAction Plan UPDATEDStephanie Villanueva AdvinculaNo ratings yet
- J Esthet Restor Dent - 2020 - Vargas - A Systematic Approach To Contouring and Polishing Anterior Resin CompositeDocument7 pagesJ Esthet Restor Dent - 2020 - Vargas - A Systematic Approach To Contouring and Polishing Anterior Resin CompositeScarleth Stephania Perez CastilloNo ratings yet
- Wiki Eval StratDocument6 pagesWiki Eval Stratapi-282459867No ratings yet
- What Is Coronary Bypass Surgery?: HeartDocument2 pagesWhat Is Coronary Bypass Surgery?: HeartSebastian BujorNo ratings yet
- A National Trauma Care System: Integrating Military and Civilian Trauma Systems To Achieve Zero Preventable Deaths After InjuryDocument431 pagesA National Trauma Care System: Integrating Military and Civilian Trauma Systems To Achieve Zero Preventable Deaths After Injuryepraetorian100% (1)
- Tamiflu PDFDocument28 pagesTamiflu PDFSopheak NGNo ratings yet
- Value of Bronchoscopy and Thoracoscopy in Respiratory MedicineDocument36 pagesValue of Bronchoscopy and Thoracoscopy in Respiratory MedicineMokwe Xavier CharlesNo ratings yet
- Glycated Hemoglobin: Dr. Anisha Mathew JRDocument28 pagesGlycated Hemoglobin: Dr. Anisha Mathew JRanimathzNo ratings yet
- Tracheostomy CareDocument3 pagesTracheostomy CareJohn Rendel LopezNo ratings yet
- Facial NerveDocument80 pagesFacial Nerverasagna reddyNo ratings yet
- Application of Lean Six Sigma Tools To Minimize Length of Stay For Ophthalmology Day Case Surgery PDFDocument18 pagesApplication of Lean Six Sigma Tools To Minimize Length of Stay For Ophthalmology Day Case Surgery PDFM HNo ratings yet
- What Are AntibioticsDocument31 pagesWhat Are Antibiotics1211988610No ratings yet
- Twin Force Bite CorrectorDocument26 pagesTwin Force Bite CorrectorMohammed ElgendyNo ratings yet
- Opd SampleDocument3 pagesOpd Samplesajid ansariNo ratings yet
- 05 N141 31673Document21 pages05 N141 31673priya thakurNo ratings yet
- (2014-10) Solomon Islands GBR Assessment ReportDocument26 pages(2014-10) Solomon Islands GBR Assessment ReportDennis MokNo ratings yet