
Green Tea JIOH
Green Tea JIOH
You might also like
- Effects of Green Tea On Periodontal Health: A Prospective Clinical StudyDocument7 pagesEffects of Green Tea On Periodontal Health: A Prospective Clinical StudyBanyu علي تقويم BiruNo ratings yet
- Dental Research Journal: Effect of Camellia Sinensis Plant On Decreasing The Level of Halitosis: A Systematic ReviewDocument7 pagesDental Research Journal: Effect of Camellia Sinensis Plant On Decreasing The Level of Halitosis: A Systematic ReviewIka KusumawatiNo ratings yet
- An in Vivo Comparison of Plaque PH Changes in Children Aged 8-12 Years After Consumption of Milk and Green Tea With SugarDocument6 pagesAn in Vivo Comparison of Plaque PH Changes in Children Aged 8-12 Years After Consumption of Milk and Green Tea With SugarSan SanNo ratings yet
- The Beneficial Effects of Green Tea in Oral Health and DentistryDocument4 pagesThe Beneficial Effects of Green Tea in Oral Health and DentistryJuve KinetNo ratings yet
- Cabrera 2006Document22 pagesCabrera 2006Yris RosarioNo ratings yet
- Natural Extracts BenefitsDocument9 pagesNatural Extracts BenefitsCoste Iulia RoxanaNo ratings yet
- Comparative Evaluation of Effects of Rinsing With Green Tea On Streptococcus Mutans Count in Plaque With That of Chlorhexidine Mouth Wash and Plain Water A Randomized Controlled TrialDocument8 pagesComparative Evaluation of Effects of Rinsing With Green Tea On Streptococcus Mutans Count in Plaque With That of Chlorhexidine Mouth Wash and Plain Water A Randomized Controlled TrialInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Molecules: Green Tea (Camellia Sinensis) : A Review of Its Phytochemistry, Pharmacology, and ToxicologyDocument23 pagesMolecules: Green Tea (Camellia Sinensis) : A Review of Its Phytochemistry, Pharmacology, and ToxicologyRohani100% (1)
- The Antimicrobial Possibilities of Green Tea: Frontiers in Microbiology August 2014Document9 pagesThe Antimicrobial Possibilities of Green Tea: Frontiers in Microbiology August 2014Sri Rizqi Muthmainnah ARNo ratings yet
- Beneficial Effects of Green Tea A Literature Review PDFDocument10 pagesBeneficial Effects of Green Tea A Literature Review PDFJohn Caryll Mancao RollorataNo ratings yet
- Antimicrobial Effect of Green Tea To: Streptococcus MutansDocument5 pagesAntimicrobial Effect of Green Tea To: Streptococcus MutansGhafran Nailul FarchiNo ratings yet
- Effect of Green Tea and Moringa Leave Extracts ForDocument11 pagesEffect of Green Tea and Moringa Leave Extracts ForYesica Marcelina SinagaNo ratings yet
- Antifungal Efficacy of Green Tea Extract Against Candida Albicans Biofilm On Tooth SubstrateDocument7 pagesAntifungal Efficacy of Green Tea Extract Against Candida Albicans Biofilm On Tooth SubstrateDennaya Listya DiasNo ratings yet
- Green Tea Drinking Habits and Awareness Among Dental Students Author Mohamed Thameemul Ansari, M Dhanraj Ganapathy, A K AnjaliDocument14 pagesGreen Tea Drinking Habits and Awareness Among Dental Students Author Mohamed Thameemul Ansari, M Dhanraj Ganapathy, A K AnjaliTrázerNándorNo ratings yet
- Beneficialeffectsofgreentea AreviewDocument22 pagesBeneficialeffectsofgreentea AreviewAquira Nato DistorNo ratings yet
- Comparative Evaluation of Effects of Rinsing With Green Tea On Streptococcus Mutans Count in Plaque With That of Chlorhexidine Mouth Wash and Plain Water A Randomized Controlled TrialDocument8 pagesComparative Evaluation of Effects of Rinsing With Green Tea On Streptococcus Mutans Count in Plaque With That of Chlorhexidine Mouth Wash and Plain Water A Randomized Controlled TrialInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Final File 5de7dccfb95724.05158507Document5 pagesFinal File 5de7dccfb95724.05158507Steven WijayaNo ratings yet
- Green Tea and Oral Health: Vinisha PandeyDocument4 pagesGreen Tea and Oral Health: Vinisha PandeyAhmed AmerNo ratings yet
- Production of Fermented Green Tea and Its Nutrient Analysis: A Mini ReviewDocument14 pagesProduction of Fermented Green Tea and Its Nutrient Analysis: A Mini Reviewthet aungNo ratings yet
- Tea Polyphenolics and Their Effect On Neurodegenerative Disordersa ReviewDocument10 pagesTea Polyphenolics and Their Effect On Neurodegenerative Disordersa ReviewJenny Rae PastorNo ratings yet
- INDIA GreenTea Easy Bioq2Document11 pagesINDIA GreenTea Easy Bioq2aguiar.rui9472No ratings yet
- Green Tea Extract For Periodontal Health: Review ArticleDocument5 pagesGreen Tea Extract For Periodontal Health: Review ArticleHerpika DianaNo ratings yet
- Tea-Microbiota ReviewDocument15 pagesTea-Microbiota ReviewjarufiansilviaNo ratings yet
- Temperature and Time of Steeping Affect The Antioxidant Properties of White, Green, and Black Tea InfusionsDocument9 pagesTemperature and Time of Steeping Affect The Antioxidant Properties of White, Green, and Black Tea InfusionsKoreab KoeenNo ratings yet
- 1 s2.0 S2212670814002036 Main 1Document5 pages1 s2.0 S2212670814002036 Main 1Vyne OrateNo ratings yet
- 7373 Ijbas IjensDocument17 pages7373 Ijbas IjensSajilata MadathilNo ratings yet
- TeaconsumptionDocument16 pagesTeaconsumptionAmbrose66No ratings yet
- Polyherbal TeaDocument13 pagesPolyherbal Teatejasborude1234No ratings yet
- Antifungal Activities of Camellia Sinensis Crude Extract, Mixture With Milk, On Selected Pathogenic and Mycotoxic FungiDocument8 pagesAntifungal Activities of Camellia Sinensis Crude Extract, Mixture With Milk, On Selected Pathogenic and Mycotoxic FungiBIOMEDSCIDIRECT PUBLICATIONSNo ratings yet
- FoodResearch 2021Document6 pagesFoodResearch 2021Jaya KumarNo ratings yet
- Original Research: Effect of Black Tea and Green Tea On Periodontal Health Status Among Dental Students at PakistanDocument3 pagesOriginal Research: Effect of Black Tea and Green Tea On Periodontal Health Status Among Dental Students at PakistanFeny NursyaputriNo ratings yet
- 1 s2.0 S2405654520300032 MainDocument9 pages1 s2.0 S2405654520300032 MainRosalin nathNo ratings yet
- Beverages 09 00001Document11 pagesBeverages 09 00001Liên ĐinhNo ratings yet
- Herbs - The Natural Alternative To Treat The Periodontal DiseasesDocument5 pagesHerbs - The Natural Alternative To Treat The Periodontal DiseasesIJAR JOURNALNo ratings yet
- Assignment (S) Submission Form: Assoc. Prof. Dr. Ivan Ho Chun Wai ..Document7 pagesAssignment (S) Submission Form: Assoc. Prof. Dr. Ivan Ho Chun Wai ..kon zhen jieNo ratings yet
- Beneficial Effects of Green Tea: A Literature ReviewDocument9 pagesBeneficial Effects of Green Tea: A Literature ReviewYoussef FaragNo ratings yet
- Extraction of Green Tea Leaves The Use of Different Methods Their Optimization and Comparative EvaluationDocument5 pagesExtraction of Green Tea Leaves The Use of Different Methods Their Optimization and Comparative Evaluationmy eveNo ratings yet
- Effect of Green Tea On Obesity - A Survey: Research ArticleDocument3 pagesEffect of Green Tea On Obesity - A Survey: Research ArticleExpressions_healthNo ratings yet
- Centella Asiatica 6Document3 pagesCentella Asiatica 6Tazkiyatul Asma'iNo ratings yet
- Green Tea Catechin Loaded Nanodelivery Systems For The Treatment of Pandemic DiseasesDocument7 pagesGreen Tea Catechin Loaded Nanodelivery Systems For The Treatment of Pandemic DiseasesLê Chiêu- ThốngNo ratings yet
- Bbrav10i01p383 386Document5 pagesBbrav10i01p383 386Mica Suzanne PajeNo ratings yet
- A Study On Wheat Grass and Its Nutritional Value: January 2012Document10 pagesA Study On Wheat Grass and Its Nutritional Value: January 2012gurupreet singhNo ratings yet
- Evaluating The Efficacy of Green Tea and Chlorhexidine Mouthwashes in Relieving Post-Extraction Complications Like Pain and HemorrhageDocument3 pagesEvaluating The Efficacy of Green Tea and Chlorhexidine Mouthwashes in Relieving Post-Extraction Complications Like Pain and HemorrhageMukarram FaridiNo ratings yet
- LECT 2 QUÍMICA Y ACTIVIDAD DEL TE VERDE p261Document8 pagesLECT 2 QUÍMICA Y ACTIVIDAD DEL TE VERDE p261edNo ratings yet
- Korir Et Al. (2014) The Fortification of Tea With Sweeteners and Milk and Its Effect On in Vitro PDFDocument9 pagesKorir Et Al. (2014) The Fortification of Tea With Sweeteners and Milk and Its Effect On in Vitro PDFYvonne TongNo ratings yet
- 117-Front Matter File-626-4-10-20220512Document13 pages117-Front Matter File-626-4-10-20220512Nita Hasna LuthfiahNo ratings yet
- Development of Rosemary Induces Green TeaDocument4 pagesDevelopment of Rosemary Induces Green TeaEditor IJTSRDNo ratings yet
- A Research ProposalDocument6 pagesA Research ProposalVrushang Maturkar100% (1)
- Green Tea Research PaperDocument6 pagesGreen Tea Research Paperefgncpe8100% (1)
- Lamo ProjectDocument12 pagesLamo ProjectlameckomondiochiengNo ratings yet
- Medicinal Plants and Their Traditional Uses: ArticleDocument6 pagesMedicinal Plants and Their Traditional Uses: ArticleMuhammadimran AliNo ratings yet
- Kazibwe2017 PDFDocument36 pagesKazibwe2017 PDFAnindya Kharisma PutriNo ratings yet
- Review On Herbal Mouthwash For Management and Prevention of Oral DiseasesDocument9 pagesReview On Herbal Mouthwash For Management and Prevention of Oral DiseasesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- International Journal of Food Science, Nutrition and Dietetics (IJFS) ISSN 2326-3350Document10 pagesInternational Journal of Food Science, Nutrition and Dietetics (IJFS) ISSN 2326-3350Asri WidyasantiNo ratings yet
- Evaluation of Diffussivity and Acceptable Mixing Ratio For Production of Hibiscus-Moringa Tea BagsDocument10 pagesEvaluation of Diffussivity and Acceptable Mixing Ratio For Production of Hibiscus-Moringa Tea BagsAZOJETENo ratings yet
- Kombucha Fermentation Test Used For Various Types of Herbal TeasDocument9 pagesKombucha Fermentation Test Used For Various Types of Herbal TeasmagdiNo ratings yet
- Ajbms 2011 4 09Document14 pagesAjbms 2011 4 09Jaya KumarNo ratings yet
- Antioxidant Activity, Theaflavin, Total Polyphenol, and Catechin Composition of Camellia Sinensis Processing Effluents From Various Factories in KenyaDocument12 pagesAntioxidant Activity, Theaflavin, Total Polyphenol, and Catechin Composition of Camellia Sinensis Processing Effluents From Various Factories in KenyaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Beneficial Effects of Green Tea: A Literature ReviewDocument9 pagesBeneficial Effects of Green Tea: A Literature ReviewbertouwNo ratings yet
- Green PowerDocument20 pagesGreen PowerNishanth SubramaniNo ratings yet
- CV - ModelDocument5 pagesCV - ModeldanzeluNo ratings yet
- Pivot Assessment and Scoring SheetDocument5 pagesPivot Assessment and Scoring SheetElaineVidalRodriguezNo ratings yet
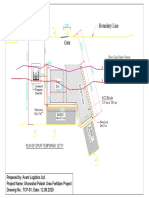
- Boundary Line: Plan of Gpuff Temporary JettyDocument1 pageBoundary Line: Plan of Gpuff Temporary Jettyshafiq_05No ratings yet
- Crab Lab ReportDocument2 pagesCrab Lab Reportapi-397859183No ratings yet
- Oral Squamous Cell Carcinoma (OSCC) : Homam Mansour Abo Orabi 201814250Document15 pagesOral Squamous Cell Carcinoma (OSCC) : Homam Mansour Abo Orabi 201814250Homam MANo ratings yet
- Replacing A Head Gasket 5A-FEDocument1 pageReplacing A Head Gasket 5A-FE985wtz8rcjNo ratings yet
- Unit 1Document16 pagesUnit 1reeta yadav0% (1)
- 2unpx203 6r2Document2 pages2unpx203 6r2Anonymous cDWQYsjd9No ratings yet
- SRA - 8601A 1 en 2Document36 pagesSRA - 8601A 1 en 2RobertNo ratings yet
- Er SopDocument19 pagesEr Sopjaybeeclaire67% (3)
- DR Bawa Garba CaseDocument10 pagesDR Bawa Garba Casemadimadi11No ratings yet
- Planning Considerations For Ice PlantsDocument5 pagesPlanning Considerations For Ice PlantsribozymesNo ratings yet
- Screening Test-EngDocument17 pagesScreening Test-EngJeffrey VallenteNo ratings yet
- Eatiing DisordersDocument69 pagesEatiing DisordersMasa MasaNo ratings yet
- Zagreb-Miler Qualitative Tests Presentation PDFDocument36 pagesZagreb-Miler Qualitative Tests Presentation PDFFernando CruzNo ratings yet
- Viruses Wanted PosterDocument2 pagesViruses Wanted Posterapi-318809591No ratings yet
- Walang Rape Sa Bontoc ReactionDocument4 pagesWalang Rape Sa Bontoc ReactionJed HernandezNo ratings yet
- COMPLETED BAB 3 - Environmental Quality Act 1974Document24 pagesCOMPLETED BAB 3 - Environmental Quality Act 1974Mohammad Fikri Bin SaidinNo ratings yet
- Family Law OutlineDocument44 pagesFamily Law OutlineBudleigh SaltertonNo ratings yet
- List of NABL Accredited Labs PDFDocument47 pagesList of NABL Accredited Labs PDFAdarsh Kumar ManwalNo ratings yet
- d000523 Doseuse RemplisseuseDocument2 pagesd000523 Doseuse RemplisseuseEnzo QuatremareNo ratings yet
- Analizador Hematologico Df50 CRPDocument41 pagesAnalizador Hematologico Df50 CRPoscarNo ratings yet
- ISO 14001-Claus-4.4.1Document2 pagesISO 14001-Claus-4.4.1Navnath TamhaneNo ratings yet
- CHEM0414ra ManilaDocument21 pagesCHEM0414ra ManilaangelomercedeblogNo ratings yet
- Bayesian-Statistics Final 20140416 3Document38 pagesBayesian-Statistics Final 20140416 3muralidharanNo ratings yet
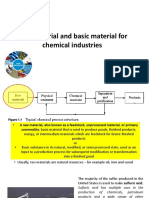
- Raw Material and Basic Material For Chemical IndustriesDocument20 pagesRaw Material and Basic Material For Chemical Industrieslaila nurul qodryNo ratings yet
- TPMC Updated Offer On 2nd List 20200110Document2 pagesTPMC Updated Offer On 2nd List 20200110gabriel240371No ratings yet
- Action Research On Students Misbehavior in ClassDocument4 pagesAction Research On Students Misbehavior in ClassAnalyn Girasol86% (7)
- Therapeutic Drug MonitoringDocument43 pagesTherapeutic Drug MonitoringMohammad AdibNo ratings yet
























































































Download as pdf or txt
You might also like
- Effects of Green Tea On Periodontal Health: A Prospective Clinical StudyDocument7 pagesEffects of Green Tea On Periodontal Health: A Prospective Clinical StudyBanyu علي تقويم BiruNo ratings yet
- Dental Research Journal: Effect of Camellia Sinensis Plant On Decreasing The Level of Halitosis: A Systematic ReviewDocument7 pagesDental Research Journal: Effect of Camellia Sinensis Plant On Decreasing The Level of Halitosis: A Systematic ReviewIka KusumawatiNo ratings yet
- An in Vivo Comparison of Plaque PH Changes in Children Aged 8-12 Years After Consumption of Milk and Green Tea With SugarDocument6 pagesAn in Vivo Comparison of Plaque PH Changes in Children Aged 8-12 Years After Consumption of Milk and Green Tea With SugarSan SanNo ratings yet
- The Beneficial Effects of Green Tea in Oral Health and DentistryDocument4 pagesThe Beneficial Effects of Green Tea in Oral Health and DentistryJuve KinetNo ratings yet
- Cabrera 2006Document22 pagesCabrera 2006Yris RosarioNo ratings yet
- Natural Extracts BenefitsDocument9 pagesNatural Extracts BenefitsCoste Iulia RoxanaNo ratings yet
- Comparative Evaluation of Effects of Rinsing With Green Tea On Streptococcus Mutans Count in Plaque With That of Chlorhexidine Mouth Wash and Plain Water A Randomized Controlled TrialDocument8 pagesComparative Evaluation of Effects of Rinsing With Green Tea On Streptococcus Mutans Count in Plaque With That of Chlorhexidine Mouth Wash and Plain Water A Randomized Controlled TrialInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Molecules: Green Tea (Camellia Sinensis) : A Review of Its Phytochemistry, Pharmacology, and ToxicologyDocument23 pagesMolecules: Green Tea (Camellia Sinensis) : A Review of Its Phytochemistry, Pharmacology, and ToxicologyRohani100% (1)
- The Antimicrobial Possibilities of Green Tea: Frontiers in Microbiology August 2014Document9 pagesThe Antimicrobial Possibilities of Green Tea: Frontiers in Microbiology August 2014Sri Rizqi Muthmainnah ARNo ratings yet
- Beneficial Effects of Green Tea A Literature Review PDFDocument10 pagesBeneficial Effects of Green Tea A Literature Review PDFJohn Caryll Mancao RollorataNo ratings yet
- Antimicrobial Effect of Green Tea To: Streptococcus MutansDocument5 pagesAntimicrobial Effect of Green Tea To: Streptococcus MutansGhafran Nailul FarchiNo ratings yet
- Effect of Green Tea and Moringa Leave Extracts ForDocument11 pagesEffect of Green Tea and Moringa Leave Extracts ForYesica Marcelina SinagaNo ratings yet
- Antifungal Efficacy of Green Tea Extract Against Candida Albicans Biofilm On Tooth SubstrateDocument7 pagesAntifungal Efficacy of Green Tea Extract Against Candida Albicans Biofilm On Tooth SubstrateDennaya Listya DiasNo ratings yet
- Green Tea Drinking Habits and Awareness Among Dental Students Author Mohamed Thameemul Ansari, M Dhanraj Ganapathy, A K AnjaliDocument14 pagesGreen Tea Drinking Habits and Awareness Among Dental Students Author Mohamed Thameemul Ansari, M Dhanraj Ganapathy, A K AnjaliTrázerNándorNo ratings yet
- Beneficialeffectsofgreentea AreviewDocument22 pagesBeneficialeffectsofgreentea AreviewAquira Nato DistorNo ratings yet
- Comparative Evaluation of Effects of Rinsing With Green Tea On Streptococcus Mutans Count in Plaque With That of Chlorhexidine Mouth Wash and Plain Water A Randomized Controlled TrialDocument8 pagesComparative Evaluation of Effects of Rinsing With Green Tea On Streptococcus Mutans Count in Plaque With That of Chlorhexidine Mouth Wash and Plain Water A Randomized Controlled TrialInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Final File 5de7dccfb95724.05158507Document5 pagesFinal File 5de7dccfb95724.05158507Steven WijayaNo ratings yet
- Green Tea and Oral Health: Vinisha PandeyDocument4 pagesGreen Tea and Oral Health: Vinisha PandeyAhmed AmerNo ratings yet
- Production of Fermented Green Tea and Its Nutrient Analysis: A Mini ReviewDocument14 pagesProduction of Fermented Green Tea and Its Nutrient Analysis: A Mini Reviewthet aungNo ratings yet
- Tea Polyphenolics and Their Effect On Neurodegenerative Disordersa ReviewDocument10 pagesTea Polyphenolics and Their Effect On Neurodegenerative Disordersa ReviewJenny Rae PastorNo ratings yet
- INDIA GreenTea Easy Bioq2Document11 pagesINDIA GreenTea Easy Bioq2aguiar.rui9472No ratings yet
- Green Tea Extract For Periodontal Health: Review ArticleDocument5 pagesGreen Tea Extract For Periodontal Health: Review ArticleHerpika DianaNo ratings yet
- Tea-Microbiota ReviewDocument15 pagesTea-Microbiota ReviewjarufiansilviaNo ratings yet
- Temperature and Time of Steeping Affect The Antioxidant Properties of White, Green, and Black Tea InfusionsDocument9 pagesTemperature and Time of Steeping Affect The Antioxidant Properties of White, Green, and Black Tea InfusionsKoreab KoeenNo ratings yet
- 1 s2.0 S2212670814002036 Main 1Document5 pages1 s2.0 S2212670814002036 Main 1Vyne OrateNo ratings yet
- 7373 Ijbas IjensDocument17 pages7373 Ijbas IjensSajilata MadathilNo ratings yet
- TeaconsumptionDocument16 pagesTeaconsumptionAmbrose66No ratings yet
- Polyherbal TeaDocument13 pagesPolyherbal Teatejasborude1234No ratings yet
- Antifungal Activities of Camellia Sinensis Crude Extract, Mixture With Milk, On Selected Pathogenic and Mycotoxic FungiDocument8 pagesAntifungal Activities of Camellia Sinensis Crude Extract, Mixture With Milk, On Selected Pathogenic and Mycotoxic FungiBIOMEDSCIDIRECT PUBLICATIONSNo ratings yet
- FoodResearch 2021Document6 pagesFoodResearch 2021Jaya KumarNo ratings yet
- Original Research: Effect of Black Tea and Green Tea On Periodontal Health Status Among Dental Students at PakistanDocument3 pagesOriginal Research: Effect of Black Tea and Green Tea On Periodontal Health Status Among Dental Students at PakistanFeny NursyaputriNo ratings yet
- 1 s2.0 S2405654520300032 MainDocument9 pages1 s2.0 S2405654520300032 MainRosalin nathNo ratings yet
- Beverages 09 00001Document11 pagesBeverages 09 00001Liên ĐinhNo ratings yet
- Herbs - The Natural Alternative To Treat The Periodontal DiseasesDocument5 pagesHerbs - The Natural Alternative To Treat The Periodontal DiseasesIJAR JOURNALNo ratings yet
- Assignment (S) Submission Form: Assoc. Prof. Dr. Ivan Ho Chun Wai ..Document7 pagesAssignment (S) Submission Form: Assoc. Prof. Dr. Ivan Ho Chun Wai ..kon zhen jieNo ratings yet
- Beneficial Effects of Green Tea: A Literature ReviewDocument9 pagesBeneficial Effects of Green Tea: A Literature ReviewYoussef FaragNo ratings yet
- Extraction of Green Tea Leaves The Use of Different Methods Their Optimization and Comparative EvaluationDocument5 pagesExtraction of Green Tea Leaves The Use of Different Methods Their Optimization and Comparative Evaluationmy eveNo ratings yet
- Effect of Green Tea On Obesity - A Survey: Research ArticleDocument3 pagesEffect of Green Tea On Obesity - A Survey: Research ArticleExpressions_healthNo ratings yet
- Centella Asiatica 6Document3 pagesCentella Asiatica 6Tazkiyatul Asma'iNo ratings yet
- Green Tea Catechin Loaded Nanodelivery Systems For The Treatment of Pandemic DiseasesDocument7 pagesGreen Tea Catechin Loaded Nanodelivery Systems For The Treatment of Pandemic DiseasesLê Chiêu- ThốngNo ratings yet
- Bbrav10i01p383 386Document5 pagesBbrav10i01p383 386Mica Suzanne PajeNo ratings yet
- A Study On Wheat Grass and Its Nutritional Value: January 2012Document10 pagesA Study On Wheat Grass and Its Nutritional Value: January 2012gurupreet singhNo ratings yet
- Evaluating The Efficacy of Green Tea and Chlorhexidine Mouthwashes in Relieving Post-Extraction Complications Like Pain and HemorrhageDocument3 pagesEvaluating The Efficacy of Green Tea and Chlorhexidine Mouthwashes in Relieving Post-Extraction Complications Like Pain and HemorrhageMukarram FaridiNo ratings yet
- LECT 2 QUÍMICA Y ACTIVIDAD DEL TE VERDE p261Document8 pagesLECT 2 QUÍMICA Y ACTIVIDAD DEL TE VERDE p261edNo ratings yet
- Korir Et Al. (2014) The Fortification of Tea With Sweeteners and Milk and Its Effect On in Vitro PDFDocument9 pagesKorir Et Al. (2014) The Fortification of Tea With Sweeteners and Milk and Its Effect On in Vitro PDFYvonne TongNo ratings yet
- 117-Front Matter File-626-4-10-20220512Document13 pages117-Front Matter File-626-4-10-20220512Nita Hasna LuthfiahNo ratings yet
- Development of Rosemary Induces Green TeaDocument4 pagesDevelopment of Rosemary Induces Green TeaEditor IJTSRDNo ratings yet
- A Research ProposalDocument6 pagesA Research ProposalVrushang Maturkar100% (1)
- Green Tea Research PaperDocument6 pagesGreen Tea Research Paperefgncpe8100% (1)
- Lamo ProjectDocument12 pagesLamo ProjectlameckomondiochiengNo ratings yet
- Medicinal Plants and Their Traditional Uses: ArticleDocument6 pagesMedicinal Plants and Their Traditional Uses: ArticleMuhammadimran AliNo ratings yet
- Kazibwe2017 PDFDocument36 pagesKazibwe2017 PDFAnindya Kharisma PutriNo ratings yet
- Review On Herbal Mouthwash For Management and Prevention of Oral DiseasesDocument9 pagesReview On Herbal Mouthwash For Management and Prevention of Oral DiseasesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- International Journal of Food Science, Nutrition and Dietetics (IJFS) ISSN 2326-3350Document10 pagesInternational Journal of Food Science, Nutrition and Dietetics (IJFS) ISSN 2326-3350Asri WidyasantiNo ratings yet
- Evaluation of Diffussivity and Acceptable Mixing Ratio For Production of Hibiscus-Moringa Tea BagsDocument10 pagesEvaluation of Diffussivity and Acceptable Mixing Ratio For Production of Hibiscus-Moringa Tea BagsAZOJETENo ratings yet
- Kombucha Fermentation Test Used For Various Types of Herbal TeasDocument9 pagesKombucha Fermentation Test Used For Various Types of Herbal TeasmagdiNo ratings yet
- Ajbms 2011 4 09Document14 pagesAjbms 2011 4 09Jaya KumarNo ratings yet
- Antioxidant Activity, Theaflavin, Total Polyphenol, and Catechin Composition of Camellia Sinensis Processing Effluents From Various Factories in KenyaDocument12 pagesAntioxidant Activity, Theaflavin, Total Polyphenol, and Catechin Composition of Camellia Sinensis Processing Effluents From Various Factories in KenyaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Beneficial Effects of Green Tea: A Literature ReviewDocument9 pagesBeneficial Effects of Green Tea: A Literature ReviewbertouwNo ratings yet
- Green PowerDocument20 pagesGreen PowerNishanth SubramaniNo ratings yet
- CV - ModelDocument5 pagesCV - ModeldanzeluNo ratings yet
- Pivot Assessment and Scoring SheetDocument5 pagesPivot Assessment and Scoring SheetElaineVidalRodriguezNo ratings yet
- Boundary Line: Plan of Gpuff Temporary JettyDocument1 pageBoundary Line: Plan of Gpuff Temporary Jettyshafiq_05No ratings yet
- Crab Lab ReportDocument2 pagesCrab Lab Reportapi-397859183No ratings yet
- Oral Squamous Cell Carcinoma (OSCC) : Homam Mansour Abo Orabi 201814250Document15 pagesOral Squamous Cell Carcinoma (OSCC) : Homam Mansour Abo Orabi 201814250Homam MANo ratings yet
- Replacing A Head Gasket 5A-FEDocument1 pageReplacing A Head Gasket 5A-FE985wtz8rcjNo ratings yet
- Unit 1Document16 pagesUnit 1reeta yadav0% (1)
- 2unpx203 6r2Document2 pages2unpx203 6r2Anonymous cDWQYsjd9No ratings yet
- SRA - 8601A 1 en 2Document36 pagesSRA - 8601A 1 en 2RobertNo ratings yet
- Er SopDocument19 pagesEr Sopjaybeeclaire67% (3)
- DR Bawa Garba CaseDocument10 pagesDR Bawa Garba Casemadimadi11No ratings yet
- Planning Considerations For Ice PlantsDocument5 pagesPlanning Considerations For Ice PlantsribozymesNo ratings yet
- Screening Test-EngDocument17 pagesScreening Test-EngJeffrey VallenteNo ratings yet
- Eatiing DisordersDocument69 pagesEatiing DisordersMasa MasaNo ratings yet
- Zagreb-Miler Qualitative Tests Presentation PDFDocument36 pagesZagreb-Miler Qualitative Tests Presentation PDFFernando CruzNo ratings yet
- Viruses Wanted PosterDocument2 pagesViruses Wanted Posterapi-318809591No ratings yet
- Walang Rape Sa Bontoc ReactionDocument4 pagesWalang Rape Sa Bontoc ReactionJed HernandezNo ratings yet
- COMPLETED BAB 3 - Environmental Quality Act 1974Document24 pagesCOMPLETED BAB 3 - Environmental Quality Act 1974Mohammad Fikri Bin SaidinNo ratings yet
- Family Law OutlineDocument44 pagesFamily Law OutlineBudleigh SaltertonNo ratings yet
- List of NABL Accredited Labs PDFDocument47 pagesList of NABL Accredited Labs PDFAdarsh Kumar ManwalNo ratings yet
- d000523 Doseuse RemplisseuseDocument2 pagesd000523 Doseuse RemplisseuseEnzo QuatremareNo ratings yet
- Analizador Hematologico Df50 CRPDocument41 pagesAnalizador Hematologico Df50 CRPoscarNo ratings yet
- ISO 14001-Claus-4.4.1Document2 pagesISO 14001-Claus-4.4.1Navnath TamhaneNo ratings yet
- CHEM0414ra ManilaDocument21 pagesCHEM0414ra ManilaangelomercedeblogNo ratings yet
- Bayesian-Statistics Final 20140416 3Document38 pagesBayesian-Statistics Final 20140416 3muralidharanNo ratings yet
- Raw Material and Basic Material For Chemical IndustriesDocument20 pagesRaw Material and Basic Material For Chemical Industrieslaila nurul qodryNo ratings yet
- TPMC Updated Offer On 2nd List 20200110Document2 pagesTPMC Updated Offer On 2nd List 20200110gabriel240371No ratings yet
- Action Research On Students Misbehavior in ClassDocument4 pagesAction Research On Students Misbehavior in ClassAnalyn Girasol86% (7)
- Therapeutic Drug MonitoringDocument43 pagesTherapeutic Drug MonitoringMohammad AdibNo ratings yet