
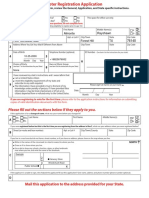
PhilHealth Claim Form1
PhilHealth Claim Form1
You might also like
- Social Pension Beneficiary FormDocument20 pagesSocial Pension Beneficiary FormRomeo Garcia, Jr.85% (48)
- Philippine Health Insurance Corporation: Republic of The PhilippinesDocument2 pagesPhilippine Health Insurance Corporation: Republic of The Philippinesangga2681No ratings yet
- The Executor's Handbook: A Step-by-Step Guide to Settling an Estate for Personal Representatives, Administrators, and Beneficiaries, Fourth EditionFrom EverandThe Executor's Handbook: A Step-by-Step Guide to Settling an Estate for Personal Representatives, Administrators, and Beneficiaries, Fourth EditionNo ratings yet
- Important Reminders:: (Claim Form)Document1 pageImportant Reminders:: (Claim Form)abejhieNo ratings yet
- CSFDocument1 pageCSFChristopher Garrata Galano Jr.50% (2)
- Claimsignatureform PDFDocument1 pageClaimsignatureform PDFClaire VillanuevaNo ratings yet
- CF 1Document2 pagesCF 1Haykal Salomon LorenaNo ratings yet
- M 1 ADocument2 pagesM 1 AtitotskyNo ratings yet
- NI4Document2 pagesNI4AnikaJohnNo ratings yet
- Ni4 PDFDocument2 pagesNi4 PDFRyan Noel BissoonNo ratings yet
- HEXA-SUNLIFE FORM 20210106 SLGFIMembersApplicationForGroupInsuranceHealthDeclaration RCBC 14OCT2021Document1 pageHEXA-SUNLIFE FORM 20210106 SLGFIMembersApplicationForGroupInsuranceHealthDeclaration RCBC 14OCT2021wrmalibiran06No ratings yet
- Latihan 8 (Tabel Lanjutan)Document2 pagesLatihan 8 (Tabel Lanjutan)Andi KurniantoNo ratings yet
- ESI FormDocument2 pagesESI Formdaskuntal2285No ratings yet
- MAP Law Will Intake Form 2015Document18 pagesMAP Law Will Intake Form 2015bash shang100% (1)
- Esi Form 1Document2 pagesEsi Form 1Dilli Rani0% (1)
- Department of Women and Child Development & Social Welfare Government of West BengalDocument2 pagesDepartment of Women and Child Development & Social Welfare Government of West BengalDark Aj0% (1)
- Pediatric Patient Registration Form TemplateDocument5 pagesPediatric Patient Registration Form TemplateHasfi YakobNo ratings yet
- Death Claim Form: CLAIMFORM DC-s Nov2016 v2 Page 1 of 3Document3 pagesDeath Claim Form: CLAIMFORM DC-s Nov2016 v2 Page 1 of 3vertine belerNo ratings yet
- New Application Form - GrandLuckyDocument3 pagesNew Application Form - GrandLuckyMuhammad RiskeyNo ratings yet
- (212202114500 PM) SASOLMED - Application - For - Membership - Fillable - NewDocument6 pages(212202114500 PM) SASOLMED - Application - For - Membership - Fillable - NewLenox D LengauNo ratings yet
- Form 13614-c Intake - Interview Quality Review Sheet 2Document4 pagesForm 13614-c Intake - Interview Quality Review Sheet 2api-593063995No ratings yet
- M 1 CDocument2 pagesM 1 CyamcarNo ratings yet
- Form - 13 (A2Z)Document2 pagesForm - 13 (A2Z)daskuntal2285No ratings yet
- Ray of Hope Membership Form ComplteDocument2 pagesRay of Hope Membership Form ComplteBrendon GovereNo ratings yet
- Application Form For Right Issue: Religare Health Insurance Company LimitedDocument2 pagesApplication Form For Right Issue: Religare Health Insurance Company LimitedSSNo ratings yet
- Annexure - Additional - Withdrawal - Details 3.0Document2 pagesAnnexure - Additional - Withdrawal - Details 3.0Vinod NairNo ratings yet
- Form ESCIDocument3 pagesForm ESCIArjun KumarNo ratings yet
- Social Pension Beneficiary FormDocument21 pagesSocial Pension Beneficiary FormRoel Almarines67% (3)
- Personal Share ApplicationDocument3 pagesPersonal Share Applicationbstinson829No ratings yet
- ClaimSignatureForm PDFDocument1 pageClaimSignatureForm PDFMuli MJNo ratings yet
- Loan Application FormDocument1 pageLoan Application FormGrely FernandezNo ratings yet
- Benjs Medicenter Patient InformationDocument1 pageBenjs Medicenter Patient InformationcharNo ratings yet
- Member Enrolment Form-GTL-without Addendum-19 Nov 2018Document2 pagesMember Enrolment Form-GTL-without Addendum-19 Nov 2018Rajesh MukkavilliNo ratings yet
- Almonte Criss nvrf-1 PDFDocument1 pageAlmonte Criss nvrf-1 PDFPandaNo ratings yet
- ESIC1Document2 pagesESIC1hr ShrimannhospitalsNo ratings yet
- Client Information Sheet Ver092018 Front.Document1 pageClient Information Sheet Ver092018 Front.Lovely TanNo ratings yet
- Patient Registration SheetDocument1 pagePatient Registration Sheetحلوم الحربيNo ratings yet
- FM-GSISOPS-OPS-ACP-01 - Application For Commencement of Pension - Rev1 - 10may2024Document2 pagesFM-GSISOPS-OPS-ACP-01 - Application For Commencement of Pension - Rev1 - 10may2024jenjen.sombiseNo ratings yet
- SGLE.03.20 : 1 General InformationDocument1 pageSGLE.03.20 : 1 General InformationCharry MarquezNo ratings yet
- PMRFDocument2 pagesPMRFKrizel Joy Serrano90% (10)
- Unisa Council Bursary Application FormDocument2 pagesUnisa Council Bursary Application FormThabisoNo ratings yet
- Emp - Code:: EDP Inward No. & Date (Supplied Free of Cost)Document7 pagesEmp - Code:: EDP Inward No. & Date (Supplied Free of Cost)John MathewNo ratings yet
- Intake/Interview & Quality Review Sheet: (October 2020) OMB Number 1545-1964Document4 pagesIntake/Interview & Quality Review Sheet: (October 2020) OMB Number 1545-1964va.amazonsellercentralNo ratings yet
- Claim Form - 2018Document2 pagesClaim Form - 2018Ronaldo De MesaNo ratings yet
- CF1 JabasDocument1 pageCF1 JabasqarlbalongNo ratings yet
- Deed of Assignment - 102018Document5 pagesDeed of Assignment - 102018Kawaii YoshinoNo ratings yet
- Application FormDocument2 pagesApplication Formmilaflor zalsosNo ratings yet
- Involuntary Servitude: Slavery Is Alive and Well in AmericaFrom EverandInvoluntary Servitude: Slavery Is Alive and Well in AmericaNo ratings yet
- Dig Deep Before You Leap: Things To Consider Before Saying "I Do!"From EverandDig Deep Before You Leap: Things To Consider Before Saying "I Do!"No ratings yet
- Rookie Year: Strategic Plan for First-Year, Brand-New and Struggling Real Estate AgentsFrom EverandRookie Year: Strategic Plan for First-Year, Brand-New and Struggling Real Estate AgentsNo ratings yet
- Immigration and Family Law: An Attorney's Toolbox of Best PracticesFrom EverandImmigration and Family Law: An Attorney's Toolbox of Best PracticesNo ratings yet
- United Healthcare Uhc Premier 1250 Cwef GoldDocument11 pagesUnited Healthcare Uhc Premier 1250 Cwef GoldgalvinwNo ratings yet
- THRIVE Summer Camp PacketDocument4 pagesTHRIVE Summer Camp PacketTana ConnerNo ratings yet
- 200704Document40 pages200704manilamedia100% (2)
- DEPED SEPT-2018 TXT - PRN PDFDocument34 pagesDEPED SEPT-2018 TXT - PRN PDFAllan PajaritoNo ratings yet
- Tables & T.code in Sap HRDocument15 pagesTables & T.code in Sap HRMAHESWARINo ratings yet
- Health Insurance - MCQ'sDocument14 pagesHealth Insurance - MCQ'ssureshbeliver005No ratings yet
- LN01 Rejda99500X 12 Principles LN11Document29 pagesLN01 Rejda99500X 12 Principles LN11Mahbubur RahmanNo ratings yet
- Revised But Not Yet CompletedDocument51 pagesRevised But Not Yet CompletedBrex Malaluan GaladoNo ratings yet
- GMC BrochureDocument11 pagesGMC BrochureDebayan SadhukhanNo ratings yet
- IMP IIMP Interview question-JLTnterview Question-JLTDocument6 pagesIMP IIMP Interview question-JLTnterview Question-JLTrajendra91No ratings yet
- Multi Purpose Parental Consent FormDocument1 pageMulti Purpose Parental Consent FormtlpinterNo ratings yet
- Towers Watson Global Medical Trends Survey Report 2014 PDFDocument14 pagesTowers Watson Global Medical Trends Survey Report 2014 PDFIrkhamWibisonoNo ratings yet
- Fenton Growth Chart CalculationsDocument6 pagesFenton Growth Chart CalculationsNahari ArifinNo ratings yet
- 1st Periodical Exam in Health 10Document2 pages1st Periodical Exam in Health 10Jhackhie Mirasol Calibo100% (2)
- The Hippocratic Underground: Civil Disobedience and Health Care ReformDocument9 pagesThe Hippocratic Underground: Civil Disobedience and Health Care ReformRebar NiemiNo ratings yet
- Latihan Asuransi KerugianDocument11 pagesLatihan Asuransi Kerugianfake ichaNo ratings yet
- Busan - South KoreaDocument118 pagesBusan - South KoreaDreamsAvenue.comNo ratings yet
- Intr On: State LifeDocument27 pagesIntr On: State LifeSarfraz AliNo ratings yet
- PlumHQ Aims To Solve India's Missing Middle Puzzle in Digital InsuranceDocument9 pagesPlumHQ Aims To Solve India's Missing Middle Puzzle in Digital InsuranceShatir LaundaNo ratings yet
- Forms of Reinsurance AgreementsDocument6 pagesForms of Reinsurance AgreementsAryan OsanNo ratings yet
- Public Health LawsDocument2 pagesPublic Health LawsDudil Goat100% (1)
- Te Unit1Document76 pagesTe Unit1troubadour2404No ratings yet
- Health Insurance Sejtrq67Document1 pageHealth Insurance Sejtrq67ahmedlakhanNo ratings yet
- Deped Cabuyao: (Claim Form 1) Revised November 2013 Series #Document1 pageDeped Cabuyao: (Claim Form 1) Revised November 2013 Series #Wehn LustreNo ratings yet
- ExamView - Chapter - 0123Document6 pagesExamView - Chapter - 0123lunaNo ratings yet
- Health Insurance Spring 2017Document2 pagesHealth Insurance Spring 2017Manideep RemalaNo ratings yet
- 2013 Scope of Appointment Form - CORBINDocument2 pages2013 Scope of Appointment Form - CORBINCorbin LindseyNo ratings yet
- Charity Care SectionDocument36 pagesCharity Care SectionRehan SadiqNo ratings yet
- RRB Group D Mock Test in Hindi Part - 10 PDFDocument44 pagesRRB Group D Mock Test in Hindi Part - 10 PDFMainu TechvisionNo ratings yet
- Shahin Kousari Amin Standard Visa Letter RequestDocument1 pageShahin Kousari Amin Standard Visa Letter RequestHamNo ratings yet

















































































Download as xls, pdf, or txt
You might also like
- Social Pension Beneficiary FormDocument20 pagesSocial Pension Beneficiary FormRomeo Garcia, Jr.85% (48)
- Philippine Health Insurance Corporation: Republic of The PhilippinesDocument2 pagesPhilippine Health Insurance Corporation: Republic of The Philippinesangga2681No ratings yet
- The Executor's Handbook: A Step-by-Step Guide to Settling an Estate for Personal Representatives, Administrators, and Beneficiaries, Fourth EditionFrom EverandThe Executor's Handbook: A Step-by-Step Guide to Settling an Estate for Personal Representatives, Administrators, and Beneficiaries, Fourth EditionNo ratings yet
- Important Reminders:: (Claim Form)Document1 pageImportant Reminders:: (Claim Form)abejhieNo ratings yet
- CSFDocument1 pageCSFChristopher Garrata Galano Jr.50% (2)
- Claimsignatureform PDFDocument1 pageClaimsignatureform PDFClaire VillanuevaNo ratings yet
- CF 1Document2 pagesCF 1Haykal Salomon LorenaNo ratings yet
- M 1 ADocument2 pagesM 1 AtitotskyNo ratings yet
- NI4Document2 pagesNI4AnikaJohnNo ratings yet
- Ni4 PDFDocument2 pagesNi4 PDFRyan Noel BissoonNo ratings yet
- HEXA-SUNLIFE FORM 20210106 SLGFIMembersApplicationForGroupInsuranceHealthDeclaration RCBC 14OCT2021Document1 pageHEXA-SUNLIFE FORM 20210106 SLGFIMembersApplicationForGroupInsuranceHealthDeclaration RCBC 14OCT2021wrmalibiran06No ratings yet
- Latihan 8 (Tabel Lanjutan)Document2 pagesLatihan 8 (Tabel Lanjutan)Andi KurniantoNo ratings yet
- ESI FormDocument2 pagesESI Formdaskuntal2285No ratings yet
- MAP Law Will Intake Form 2015Document18 pagesMAP Law Will Intake Form 2015bash shang100% (1)
- Esi Form 1Document2 pagesEsi Form 1Dilli Rani0% (1)
- Department of Women and Child Development & Social Welfare Government of West BengalDocument2 pagesDepartment of Women and Child Development & Social Welfare Government of West BengalDark Aj0% (1)
- Pediatric Patient Registration Form TemplateDocument5 pagesPediatric Patient Registration Form TemplateHasfi YakobNo ratings yet
- Death Claim Form: CLAIMFORM DC-s Nov2016 v2 Page 1 of 3Document3 pagesDeath Claim Form: CLAIMFORM DC-s Nov2016 v2 Page 1 of 3vertine belerNo ratings yet
- New Application Form - GrandLuckyDocument3 pagesNew Application Form - GrandLuckyMuhammad RiskeyNo ratings yet
- (212202114500 PM) SASOLMED - Application - For - Membership - Fillable - NewDocument6 pages(212202114500 PM) SASOLMED - Application - For - Membership - Fillable - NewLenox D LengauNo ratings yet
- Form 13614-c Intake - Interview Quality Review Sheet 2Document4 pagesForm 13614-c Intake - Interview Quality Review Sheet 2api-593063995No ratings yet
- M 1 CDocument2 pagesM 1 CyamcarNo ratings yet
- Form - 13 (A2Z)Document2 pagesForm - 13 (A2Z)daskuntal2285No ratings yet
- Ray of Hope Membership Form ComplteDocument2 pagesRay of Hope Membership Form ComplteBrendon GovereNo ratings yet
- Application Form For Right Issue: Religare Health Insurance Company LimitedDocument2 pagesApplication Form For Right Issue: Religare Health Insurance Company LimitedSSNo ratings yet
- Annexure - Additional - Withdrawal - Details 3.0Document2 pagesAnnexure - Additional - Withdrawal - Details 3.0Vinod NairNo ratings yet
- Form ESCIDocument3 pagesForm ESCIArjun KumarNo ratings yet
- Social Pension Beneficiary FormDocument21 pagesSocial Pension Beneficiary FormRoel Almarines67% (3)
- Personal Share ApplicationDocument3 pagesPersonal Share Applicationbstinson829No ratings yet
- ClaimSignatureForm PDFDocument1 pageClaimSignatureForm PDFMuli MJNo ratings yet
- Loan Application FormDocument1 pageLoan Application FormGrely FernandezNo ratings yet
- Benjs Medicenter Patient InformationDocument1 pageBenjs Medicenter Patient InformationcharNo ratings yet
- Member Enrolment Form-GTL-without Addendum-19 Nov 2018Document2 pagesMember Enrolment Form-GTL-without Addendum-19 Nov 2018Rajesh MukkavilliNo ratings yet
- Almonte Criss nvrf-1 PDFDocument1 pageAlmonte Criss nvrf-1 PDFPandaNo ratings yet
- ESIC1Document2 pagesESIC1hr ShrimannhospitalsNo ratings yet
- Client Information Sheet Ver092018 Front.Document1 pageClient Information Sheet Ver092018 Front.Lovely TanNo ratings yet
- Patient Registration SheetDocument1 pagePatient Registration Sheetحلوم الحربيNo ratings yet
- FM-GSISOPS-OPS-ACP-01 - Application For Commencement of Pension - Rev1 - 10may2024Document2 pagesFM-GSISOPS-OPS-ACP-01 - Application For Commencement of Pension - Rev1 - 10may2024jenjen.sombiseNo ratings yet
- SGLE.03.20 : 1 General InformationDocument1 pageSGLE.03.20 : 1 General InformationCharry MarquezNo ratings yet
- PMRFDocument2 pagesPMRFKrizel Joy Serrano90% (10)
- Unisa Council Bursary Application FormDocument2 pagesUnisa Council Bursary Application FormThabisoNo ratings yet
- Emp - Code:: EDP Inward No. & Date (Supplied Free of Cost)Document7 pagesEmp - Code:: EDP Inward No. & Date (Supplied Free of Cost)John MathewNo ratings yet
- Intake/Interview & Quality Review Sheet: (October 2020) OMB Number 1545-1964Document4 pagesIntake/Interview & Quality Review Sheet: (October 2020) OMB Number 1545-1964va.amazonsellercentralNo ratings yet
- Claim Form - 2018Document2 pagesClaim Form - 2018Ronaldo De MesaNo ratings yet
- CF1 JabasDocument1 pageCF1 JabasqarlbalongNo ratings yet
- Deed of Assignment - 102018Document5 pagesDeed of Assignment - 102018Kawaii YoshinoNo ratings yet
- Application FormDocument2 pagesApplication Formmilaflor zalsosNo ratings yet
- Involuntary Servitude: Slavery Is Alive and Well in AmericaFrom EverandInvoluntary Servitude: Slavery Is Alive and Well in AmericaNo ratings yet
- Dig Deep Before You Leap: Things To Consider Before Saying "I Do!"From EverandDig Deep Before You Leap: Things To Consider Before Saying "I Do!"No ratings yet
- Rookie Year: Strategic Plan for First-Year, Brand-New and Struggling Real Estate AgentsFrom EverandRookie Year: Strategic Plan for First-Year, Brand-New and Struggling Real Estate AgentsNo ratings yet
- Immigration and Family Law: An Attorney's Toolbox of Best PracticesFrom EverandImmigration and Family Law: An Attorney's Toolbox of Best PracticesNo ratings yet
- United Healthcare Uhc Premier 1250 Cwef GoldDocument11 pagesUnited Healthcare Uhc Premier 1250 Cwef GoldgalvinwNo ratings yet
- THRIVE Summer Camp PacketDocument4 pagesTHRIVE Summer Camp PacketTana ConnerNo ratings yet
- 200704Document40 pages200704manilamedia100% (2)
- DEPED SEPT-2018 TXT - PRN PDFDocument34 pagesDEPED SEPT-2018 TXT - PRN PDFAllan PajaritoNo ratings yet
- Tables & T.code in Sap HRDocument15 pagesTables & T.code in Sap HRMAHESWARINo ratings yet
- Health Insurance - MCQ'sDocument14 pagesHealth Insurance - MCQ'ssureshbeliver005No ratings yet
- LN01 Rejda99500X 12 Principles LN11Document29 pagesLN01 Rejda99500X 12 Principles LN11Mahbubur RahmanNo ratings yet
- Revised But Not Yet CompletedDocument51 pagesRevised But Not Yet CompletedBrex Malaluan GaladoNo ratings yet
- GMC BrochureDocument11 pagesGMC BrochureDebayan SadhukhanNo ratings yet
- IMP IIMP Interview question-JLTnterview Question-JLTDocument6 pagesIMP IIMP Interview question-JLTnterview Question-JLTrajendra91No ratings yet
- Multi Purpose Parental Consent FormDocument1 pageMulti Purpose Parental Consent FormtlpinterNo ratings yet
- Towers Watson Global Medical Trends Survey Report 2014 PDFDocument14 pagesTowers Watson Global Medical Trends Survey Report 2014 PDFIrkhamWibisonoNo ratings yet
- Fenton Growth Chart CalculationsDocument6 pagesFenton Growth Chart CalculationsNahari ArifinNo ratings yet
- 1st Periodical Exam in Health 10Document2 pages1st Periodical Exam in Health 10Jhackhie Mirasol Calibo100% (2)
- The Hippocratic Underground: Civil Disobedience and Health Care ReformDocument9 pagesThe Hippocratic Underground: Civil Disobedience and Health Care ReformRebar NiemiNo ratings yet
- Latihan Asuransi KerugianDocument11 pagesLatihan Asuransi Kerugianfake ichaNo ratings yet
- Busan - South KoreaDocument118 pagesBusan - South KoreaDreamsAvenue.comNo ratings yet
- Intr On: State LifeDocument27 pagesIntr On: State LifeSarfraz AliNo ratings yet
- PlumHQ Aims To Solve India's Missing Middle Puzzle in Digital InsuranceDocument9 pagesPlumHQ Aims To Solve India's Missing Middle Puzzle in Digital InsuranceShatir LaundaNo ratings yet
- Forms of Reinsurance AgreementsDocument6 pagesForms of Reinsurance AgreementsAryan OsanNo ratings yet
- Public Health LawsDocument2 pagesPublic Health LawsDudil Goat100% (1)
- Te Unit1Document76 pagesTe Unit1troubadour2404No ratings yet
- Health Insurance Sejtrq67Document1 pageHealth Insurance Sejtrq67ahmedlakhanNo ratings yet
- Deped Cabuyao: (Claim Form 1) Revised November 2013 Series #Document1 pageDeped Cabuyao: (Claim Form 1) Revised November 2013 Series #Wehn LustreNo ratings yet
- ExamView - Chapter - 0123Document6 pagesExamView - Chapter - 0123lunaNo ratings yet
- Health Insurance Spring 2017Document2 pagesHealth Insurance Spring 2017Manideep RemalaNo ratings yet
- 2013 Scope of Appointment Form - CORBINDocument2 pages2013 Scope of Appointment Form - CORBINCorbin LindseyNo ratings yet
- Charity Care SectionDocument36 pagesCharity Care SectionRehan SadiqNo ratings yet
- RRB Group D Mock Test in Hindi Part - 10 PDFDocument44 pagesRRB Group D Mock Test in Hindi Part - 10 PDFMainu TechvisionNo ratings yet
- Shahin Kousari Amin Standard Visa Letter RequestDocument1 pageShahin Kousari Amin Standard Visa Letter RequestHamNo ratings yet