Download as pdf or txt
You might also like
- Science 6 - Q1 - Module1 - Lesson1 - Describing MixturesDocument29 pagesScience 6 - Q1 - Module1 - Lesson1 - Describing MixturesRose Merie Joy Solmia78% (27)
- APHDocument107 pagesAPHbaby100% (2)
- MC Book Final July 2014Document383 pagesMC Book Final July 2014Latosha TrevinoNo ratings yet
- Tafe NSW: Knowledge AssessmentDocument30 pagesTafe NSW: Knowledge AssessmentDibyendu Karmakar100% (3)
- Bizhub c3350 Manual PDFDocument81 pagesBizhub c3350 Manual PDFStiven PereiraNo ratings yet
- Materi VBAC Lovamil 202Document30 pagesMateri VBAC Lovamil 202Zoeva VirdiniaNo ratings yet
- Childbirth and The Female Pelvic Floor: Christopher Maher Wesley UrogynaecologyDocument54 pagesChildbirth and The Female Pelvic Floor: Christopher Maher Wesley UrogynaecologyVeronica MendozaNo ratings yet
- Eclampsia: An Enigma: Chitra JoshiDocument4 pagesEclampsia: An Enigma: Chitra JoshiM Haris Yoga IswantoroNo ratings yet
- 1 - Midtrimester Loss - MI Aldika AkbarDocument36 pages1 - Midtrimester Loss - MI Aldika Akbaraldo susenoNo ratings yet
- A Study of Intrauterine Fetal Death in A Tertiary Care HospitalDocument4 pagesA Study of Intrauterine Fetal Death in A Tertiary Care HospitalintanNo ratings yet
- EP Classificationdraft For ReviewDocument28 pagesEP Classificationdraft For ReviewMaria MogosNo ratings yet
- Ofir 2003Document5 pagesOfir 2003Jim HawkinsNo ratings yet
- 9814-Article Text-20674-1-10-20130704Document7 pages9814-Article Text-20674-1-10-20130704lenysfaridaNo ratings yet
- Study of Vaginal Flora and Its Relationship With Preterm Labour Pain and PpromDocument5 pagesStudy of Vaginal Flora and Its Relationship With Preterm Labour Pain and PpromIJAR JOURNALNo ratings yet
- 15 JMSCRDocument5 pages15 JMSCRVani Junior LoverzNo ratings yet
- FRCDocument6 pagesFRCFino GunnersNo ratings yet
- EJHM - Volume 77 - Issue 3 - Pages 5109-5113Document5 pagesEJHM - Volume 77 - Issue 3 - Pages 5109-5113Andrian drsNo ratings yet
- Paediatrica Indonesiana: Guslihan D Tjipta, MD Riza I Nasution, MD Dachrul Aldy, MD Zakaria Siregar, MDDocument4 pagesPaediatrica Indonesiana: Guslihan D Tjipta, MD Riza I Nasution, MD Dachrul Aldy, MD Zakaria Siregar, MDIin Fadhilah Utami NewNo ratings yet
- Baru MDocument3 pagesBaru MRezky Wulandari RoniNo ratings yet
- Xternal Ephalic Ersion: E Z W ' H P C P GDocument4 pagesXternal Ephalic Ersion: E Z W ' H P C P GJuan SetiajiNo ratings yet
- 1228-Article Text-2170-1-10-20180201Document3 pages1228-Article Text-2170-1-10-20180201pavani pNo ratings yet
- Faysal Bas It,+86-89-MinDocument4 pagesFaysal Bas It,+86-89-MinIT RSMPNo ratings yet
- Newborn CareDocument57 pagesNewborn CareDIPENDRA KUMAR KUSHAWAHANo ratings yet
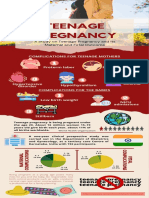
- Info GraphicDocument1 pageInfo GraphicBenjamin GabrielNo ratings yet
- Critical Appraisal Ayu RonoDocument41 pagesCritical Appraisal Ayu Ronoamarendra WardhanaNo ratings yet
- 02 Study Day 2016 - Severe Obesity Study Interim FindingsDocument26 pages02 Study Day 2016 - Severe Obesity Study Interim Findingsvrajesh pandhiNo ratings yet
- Trial of Labour After Caesarean SectionDocument37 pagesTrial of Labour After Caesarean Sectionh27nkhhtw4No ratings yet
- (25. JAMP - Shaily Sengar) 536-540Document5 pages(25. JAMP - Shaily Sengar) 536-540dpdoors19No ratings yet
- A013950104 PDFDocument4 pagesA013950104 PDFCitra Indah SariNo ratings yet
- Impact of FLAMM Scoring On Cesarean Section Rate in Previous One Lower Segment Cesarean Section PatientDocument4 pagesImpact of FLAMM Scoring On Cesarean Section Rate in Previous One Lower Segment Cesarean Section PatientSNNo ratings yet
- Ojog 2018080316254387 PDFDocument13 pagesOjog 2018080316254387 PDFyundrimartirazNo ratings yet
- Placenta Previa Maternal and Foetal OutcomeDocument4 pagesPlacenta Previa Maternal and Foetal OutcomeAkshay BeradNo ratings yet
- The Rate and Indication of Caesarean Section in ADocument7 pagesThe Rate and Indication of Caesarean Section in AdhananjayNo ratings yet
- Mat N Fet ConseqDocument6 pagesMat N Fet ConseqRaissa Metasari TantoNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument6 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- May 2020 Indications of PCS in Multiparous WomenDocument4 pagesMay 2020 Indications of PCS in Multiparous WomenTushar BahetiNo ratings yet
- Ojog 2014102311015160 PDFDocument7 pagesOjog 2014102311015160 PDFubayyumrNo ratings yet
- Study of Cases of Rupture Uterus in A Tertiary InsDocument6 pagesStudy of Cases of Rupture Uterus in A Tertiary InsErena HairunisaNo ratings yet
- Jurnal Internasional Ruptur UteriDocument5 pagesJurnal Internasional Ruptur UteriNovita MayasariNo ratings yet
- Jurnal FetoDocument4 pagesJurnal FetoAl NaifNo ratings yet
- D013531316 PDFDocument4 pagesD013531316 PDFFitri Nur DiniNo ratings yet
- A Retrospective Study On Fetomaternal Outcome in Second Stage Cesarean-SectionDocument5 pagesA Retrospective Study On Fetomaternal Outcome in Second Stage Cesarean-SectionIJAR JOURNALNo ratings yet
- Learning Outcome: Preterm BirthDocument13 pagesLearning Outcome: Preterm Birthfairodz salapudinNo ratings yet
- Newborn Assessment & Care. KabaleDocument41 pagesNewborn Assessment & Care. KabaleNinaNo ratings yet
- Predictive Value of Various Risk Factors For Preterm Labor: Original ArticleDocument5 pagesPredictive Value of Various Risk Factors For Preterm Labor: Original ArticleDuma MargarethaNo ratings yet
- Jurnal Inggris PDFDocument4 pagesJurnal Inggris PDFTom PrasNo ratings yet
- (2020) Induction of Labour at Term Increase Risk of SC For Advanced Maternal AgeDocument7 pages(2020) Induction of Labour at Term Increase Risk of SC For Advanced Maternal AgeaninditaNo ratings yet
- A Study of Primary Caesarean Section in MultiparaDocument5 pagesA Study of Primary Caesarean Section in Multiparapavani pNo ratings yet
- Episiotomy and Its Complications - A Cross Sectional Study in SecoDocument4 pagesEpisiotomy and Its Complications - A Cross Sectional Study in SecoMinimotitaNo ratings yet
- Maternal Movement For Better OutcomesDocument36 pagesMaternal Movement For Better OutcomesliverpooldoulaNo ratings yet
- Maravilla AttitudeofNursesDocument30 pagesMaravilla AttitudeofNursesSevered AppleheadNo ratings yet
- No Kode Diagnosa Utama Jumlah %Document3 pagesNo Kode Diagnosa Utama Jumlah %Ryan AkbarNo ratings yet
- In Vitro Fertilization: Indication-Procedure-MonitoringDocument68 pagesIn Vitro Fertilization: Indication-Procedure-MonitoringFathia RizkiNo ratings yet
- Failed Induction of Labor - 2022 - YmobDocument6 pagesFailed Induction of Labor - 2022 - YmobMor OB-GYNNo ratings yet
- Villous Oedema of The Placenta: A Clinicopathological StudyDocument11 pagesVillous Oedema of The Placenta: A Clinicopathological StudyYo MeNo ratings yet
- Kogi Semarang-Emerging of AIP-SurabayaDocument28 pagesKogi Semarang-Emerging of AIP-Surabayaxxxx009No ratings yet
- The Umbilic Cord Attachment Anomality and Discordant Growth of Fetus in Twin PregnancyDocument6 pagesThe Umbilic Cord Attachment Anomality and Discordant Growth of Fetus in Twin PregnancyCentral Asian StudiesNo ratings yet
- AmniosDocument15 pagesAmniosneko niNo ratings yet
- Antepartum Haemorrhage: Causes & Its Effects On Mother and Child: An EvaluationDocument5 pagesAntepartum Haemorrhage: Causes & Its Effects On Mother and Child: An EvaluationubayyumrNo ratings yet
- Considerații Anatomoclinice Și Terapeutice Pe Seama Limfangioamelor LaDocument19 pagesConsiderații Anatomoclinice Și Terapeutice Pe Seama Limfangioamelor LaMariaNo ratings yet
- ENC Lecture2Document46 pagesENC Lecture2Fachmi Putera Susila SinuratNo ratings yet
- Placenta IsuogDocument40 pagesPlacenta IsuogKARINA BASTIDAS IBARRA100% (1)
- Essential Newborn Care: Prof. S N Singh PediatricsDocument46 pagesEssential Newborn Care: Prof. S N Singh PediatricsauliaNo ratings yet
- Pregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsFrom EverandPregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsNo ratings yet
- Sonographic Differentiation Between Blighted Ovum and Early Viable PregnancyDocument6 pagesSonographic Differentiation Between Blighted Ovum and Early Viable Pregnancypuji arisNo ratings yet
- in Room Dining MenuDocument18 pagesin Room Dining Menupuji arisNo ratings yet
- CPG Gyne VulvarDocument9 pagesCPG Gyne Vulvarpuji arisNo ratings yet
- Bukan Mapping ICU 11 April: NO Nama Diagnosis Sekarang Lab TerapiDocument3 pagesBukan Mapping ICU 11 April: NO Nama Diagnosis Sekarang Lab Terapipuji arisNo ratings yet
- Maternal and Fetal Factors in Pregnancy With Oligohydramnios and Maternal and Perinatal OutcomeDocument4 pagesMaternal and Fetal Factors in Pregnancy With Oligohydramnios and Maternal and Perinatal Outcomepuji arisNo ratings yet
- Ams 12 28530 PDFDocument7 pagesAms 12 28530 PDFpuji arisNo ratings yet
- During Compaction: Void SpacesDocument21 pagesDuring Compaction: Void SpacesMinilik Tikur SewNo ratings yet
- Creative Writing MelcsDocument3 pagesCreative Writing MelcsArnel Navales100% (7)
- Caustinerf ForteDocument5 pagesCaustinerf Fortefadli_nugraha6109No ratings yet
- Government Engineering College Dahod: Dadhichi HostelDocument5 pagesGovernment Engineering College Dahod: Dadhichi HostelSandip MouryaNo ratings yet
- A Feminist Reading of Selected Poems of Kishwar Naheed: Huzaifa PanditDocument15 pagesA Feminist Reading of Selected Poems of Kishwar Naheed: Huzaifa PanditShivangi DubeyNo ratings yet
- Drum WorkbookDocument6 pagesDrum WorkbookSteph Dela MujerNo ratings yet
- Serva Cementing 113015 LR Pages PDFDocument16 pagesServa Cementing 113015 LR Pages PDFAnonymous uKoNmLxkNo ratings yet
- EMMVEE - On-Grid PV Modules - DatasheetDocument2 pagesEMMVEE - On-Grid PV Modules - Datasheetmk gandhiNo ratings yet
- MSDS WP 950C30Document3 pagesMSDS WP 950C30IB KNo ratings yet
- Technical Manual For Design and Construction of Road Tunnels-2010 PDFDocument648 pagesTechnical Manual For Design and Construction of Road Tunnels-2010 PDFAsim Amin100% (1)
- License Renewal Guide - 2023Document37 pagesLicense Renewal Guide - 2023edrian.ranjo.guerrero0916No ratings yet
- 2023 Physics Study NotesDocument2 pages2023 Physics Study NotesPrapti SharmaNo ratings yet
- You As An Entrepreneur: SOFTNET Information Technology Center IncDocument7 pagesYou As An Entrepreneur: SOFTNET Information Technology Center IncVirnadette OlinaresNo ratings yet
- CO2 Absorption1Document8 pagesCO2 Absorption1arun manchekarNo ratings yet
- MassDocument2 pagesMassapi-222745762No ratings yet
- Parameters For IPG-83H40PL-BDocument5 pagesParameters For IPG-83H40PL-BJack DanielsNo ratings yet
- Sunpower 405, 410 y 415 WDocument2 pagesSunpower 405, 410 y 415 WArmandoVelazcoRangelNo ratings yet
- Chapter 8 Sheetpiles and CofferdamsDocument10 pagesChapter 8 Sheetpiles and CofferdamsYIBELTAL EBABU100% (2)
- Basic Similarity TheoremsDocument21 pagesBasic Similarity TheoremsRose Anne MetranNo ratings yet
- Bloom Ks2-Maths-Blooms-Taxonomy-Meet-The-Bloom-Superheroes-Desk-Mat - Ver - 3Document1 pageBloom Ks2-Maths-Blooms-Taxonomy-Meet-The-Bloom-Superheroes-Desk-Mat - Ver - 3hongbongNo ratings yet
- Post Office Custom Declaration FormDocument1 pagePost Office Custom Declaration Formw2vijayNo ratings yet
- Form 1 Admission Application (SE2)Document4 pagesForm 1 Admission Application (SE2)trueNo ratings yet
- EA Requirements For The Accreditation of Flexible Scopes: Publication ReferenceDocument8 pagesEA Requirements For The Accreditation of Flexible Scopes: Publication ReferenceBrandon EricksonNo ratings yet
- Truth and Falsehood in IslamDocument3 pagesTruth and Falsehood in IslamZiad Cassim (anti-Sufi)No ratings yet
- Budesonide (Drug Study)Document3 pagesBudesonide (Drug Study)Franz.thenurse6888No ratings yet
- The Encyclopedia of Drug AbuseDocument417 pagesThe Encyclopedia of Drug AbuseOmnia Wanies100% (2)