
10.1055@s 0039 1688700 PDF
10.1055@s 0039 1688700 PDF
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- BPDocument8 pagesBPpsychgypsy100% (9)
- Surgical CricothyroidotomyDocument1 pageSurgical Cricothyroidotomyintan rosliNo ratings yet
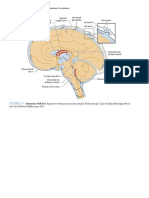
- Figure 3-7: PART I Neuroanatomy and Neuroanatomic LocalizationDocument1 pageFigure 3-7: PART I Neuroanatomy and Neuroanatomic Localizationintan rosliNo ratings yet
- Orthopaedic AnatomyDocument1 pageOrthopaedic Anatomyintan rosliNo ratings yet
- Corticosteroid Injection For de Quervain's Tenosynovitis (Review)Document19 pagesCorticosteroid Injection For de Quervain's Tenosynovitis (Review)intan rosliNo ratings yet
- Translocation NeuromaDocument1 pageTranslocation Neuromaintan rosliNo ratings yet
- Translocation NeuromaDocument1 pageTranslocation Neuromaintan rosliNo ratings yet
- 7.2 Non-Absorbable Suture MaterialsDocument1 page7.2 Non-Absorbable Suture Materialsintan rosliNo ratings yet
- Antimicrobial Resistance in LeprosyDocument6 pagesAntimicrobial Resistance in Leprosyintan rosliNo ratings yet
- Chapter 13 ProblemsDocument4 pagesChapter 13 Problemswalt richardsNo ratings yet
- Discrimination, Stigma, and Mental Health Care AccessDocument1 pageDiscrimination, Stigma, and Mental Health Care AccessCerlyn CabanitNo ratings yet
- Drug Study AmpicillinDocument3 pagesDrug Study AmpicillinJessie Batilo33% (3)
- Characterizing The Oncogenic Importance and Exploring Gene-Immune Cells Correlation of ACTB in Human CancersDocument20 pagesCharacterizing The Oncogenic Importance and Exploring Gene-Immune Cells Correlation of ACTB in Human Cancersmostafa elharranyNo ratings yet
- Operative DeliveryDocument19 pagesOperative DeliveryMtwe ZakayoNo ratings yet
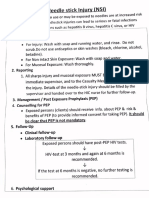
- Needle: Stick Injury (NSI)Document5 pagesNeedle: Stick Injury (NSI)dr rajoreNo ratings yet
- Thyroid ScoreDocument6 pagesThyroid ScoreleozdmNo ratings yet
- Breast ScreeningDocument87 pagesBreast ScreeningDira NidausshafaNo ratings yet
- Filmarray Panel: Blood Culture IdentificationDocument2 pagesFilmarray Panel: Blood Culture IdentificationpabquimNo ratings yet
- Drug Study-AkinetonDocument2 pagesDrug Study-AkinetonKrizia KrizhNo ratings yet
- SeminarDocument34 pagesSeminarMuhammad Faiz Satria WibowoNo ratings yet
- XN-1000 R HematologyDocument6 pagesXN-1000 R HematologyMaria Chacón CarbajalNo ratings yet
- CNM's Post Vaccine ProtocolDocument7 pagesCNM's Post Vaccine ProtocolDylroNo ratings yet
- @MBS MedicalBooksStore 2019 The PDFDocument394 pages@MBS MedicalBooksStore 2019 The PDFDsdentalNo ratings yet
- Teenage PregnancyDocument19 pagesTeenage Pregnancyreynaldo banaria jrNo ratings yet
- Cysts and CancerDocument1 pageCysts and CancerMo'ayad OkylanNo ratings yet
- Matsukawa 2017Document33 pagesMatsukawa 2017kanaNo ratings yet
- GRAM STAINING AND CLINICAL UTILITY by Dr.T.V.Rao MDDocument2 pagesGRAM STAINING AND CLINICAL UTILITY by Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- Do Not Copy Penalties Apply: The Role of Cutaneous Microbiota Harmony in Maintaining A Functional Skin BarrierDocument7 pagesDo Not Copy Penalties Apply: The Role of Cutaneous Microbiota Harmony in Maintaining A Functional Skin BarriereaudreyliaNo ratings yet
- Twenty One Pilots - CancerDocument2 pagesTwenty One Pilots - CancerRaphael SaftaNo ratings yet
- WHO Diabetes Infographic 2016Document2 pagesWHO Diabetes Infographic 2016The Independent MagazineNo ratings yet
- OT Sample Exam QuestionsDocument4 pagesOT Sample Exam Questionsagatha2108No ratings yet
- Fetal Echocardiogram ProtocolDocument4 pagesFetal Echocardiogram Protocolapi-349402240No ratings yet
- Q3-Health-D3 CotDocument4 pagesQ3-Health-D3 CotDennis MartinezNo ratings yet
- Manual HIV Tri DotDocument4 pagesManual HIV Tri DotDr.Soumen Saha100% (1)
- Certificate of Performance For Anesthesia Machine: Medicover HospitalsDocument1 pageCertificate of Performance For Anesthesia Machine: Medicover HospitalsIKON RESPONSE0% (1)
- Doctors Progress Note - Module 5Document4 pagesDoctors Progress Note - Module 5adrian nakilaNo ratings yet
- PusoDocument4 pagesPusoStephanie SundiangNo ratings yet
- Perioperative Fasting and Feeding in Adults, Obstetric, Paediatric and Bariatric Population-Practice Guidelines From The Indian Society of AnaesthesiologistsDocument29 pagesPerioperative Fasting and Feeding in Adults, Obstetric, Paediatric and Bariatric Population-Practice Guidelines From The Indian Society of Anaesthesiologistsambitiousamit1No ratings yet











































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- BPDocument8 pagesBPpsychgypsy100% (9)
- Surgical CricothyroidotomyDocument1 pageSurgical Cricothyroidotomyintan rosliNo ratings yet
- Figure 3-7: PART I Neuroanatomy and Neuroanatomic LocalizationDocument1 pageFigure 3-7: PART I Neuroanatomy and Neuroanatomic Localizationintan rosliNo ratings yet
- Orthopaedic AnatomyDocument1 pageOrthopaedic Anatomyintan rosliNo ratings yet
- Corticosteroid Injection For de Quervain's Tenosynovitis (Review)Document19 pagesCorticosteroid Injection For de Quervain's Tenosynovitis (Review)intan rosliNo ratings yet
- Translocation NeuromaDocument1 pageTranslocation Neuromaintan rosliNo ratings yet
- Translocation NeuromaDocument1 pageTranslocation Neuromaintan rosliNo ratings yet
- 7.2 Non-Absorbable Suture MaterialsDocument1 page7.2 Non-Absorbable Suture Materialsintan rosliNo ratings yet
- Antimicrobial Resistance in LeprosyDocument6 pagesAntimicrobial Resistance in Leprosyintan rosliNo ratings yet
- Chapter 13 ProblemsDocument4 pagesChapter 13 Problemswalt richardsNo ratings yet
- Discrimination, Stigma, and Mental Health Care AccessDocument1 pageDiscrimination, Stigma, and Mental Health Care AccessCerlyn CabanitNo ratings yet
- Drug Study AmpicillinDocument3 pagesDrug Study AmpicillinJessie Batilo33% (3)
- Characterizing The Oncogenic Importance and Exploring Gene-Immune Cells Correlation of ACTB in Human CancersDocument20 pagesCharacterizing The Oncogenic Importance and Exploring Gene-Immune Cells Correlation of ACTB in Human Cancersmostafa elharranyNo ratings yet
- Operative DeliveryDocument19 pagesOperative DeliveryMtwe ZakayoNo ratings yet
- Needle: Stick Injury (NSI)Document5 pagesNeedle: Stick Injury (NSI)dr rajoreNo ratings yet
- Thyroid ScoreDocument6 pagesThyroid ScoreleozdmNo ratings yet
- Breast ScreeningDocument87 pagesBreast ScreeningDira NidausshafaNo ratings yet
- Filmarray Panel: Blood Culture IdentificationDocument2 pagesFilmarray Panel: Blood Culture IdentificationpabquimNo ratings yet
- Drug Study-AkinetonDocument2 pagesDrug Study-AkinetonKrizia KrizhNo ratings yet
- SeminarDocument34 pagesSeminarMuhammad Faiz Satria WibowoNo ratings yet
- XN-1000 R HematologyDocument6 pagesXN-1000 R HematologyMaria Chacón CarbajalNo ratings yet
- CNM's Post Vaccine ProtocolDocument7 pagesCNM's Post Vaccine ProtocolDylroNo ratings yet
- @MBS MedicalBooksStore 2019 The PDFDocument394 pages@MBS MedicalBooksStore 2019 The PDFDsdentalNo ratings yet
- Teenage PregnancyDocument19 pagesTeenage Pregnancyreynaldo banaria jrNo ratings yet
- Cysts and CancerDocument1 pageCysts and CancerMo'ayad OkylanNo ratings yet
- Matsukawa 2017Document33 pagesMatsukawa 2017kanaNo ratings yet
- GRAM STAINING AND CLINICAL UTILITY by Dr.T.V.Rao MDDocument2 pagesGRAM STAINING AND CLINICAL UTILITY by Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- Do Not Copy Penalties Apply: The Role of Cutaneous Microbiota Harmony in Maintaining A Functional Skin BarrierDocument7 pagesDo Not Copy Penalties Apply: The Role of Cutaneous Microbiota Harmony in Maintaining A Functional Skin BarriereaudreyliaNo ratings yet
- Twenty One Pilots - CancerDocument2 pagesTwenty One Pilots - CancerRaphael SaftaNo ratings yet
- WHO Diabetes Infographic 2016Document2 pagesWHO Diabetes Infographic 2016The Independent MagazineNo ratings yet
- OT Sample Exam QuestionsDocument4 pagesOT Sample Exam Questionsagatha2108No ratings yet
- Fetal Echocardiogram ProtocolDocument4 pagesFetal Echocardiogram Protocolapi-349402240No ratings yet
- Q3-Health-D3 CotDocument4 pagesQ3-Health-D3 CotDennis MartinezNo ratings yet
- Manual HIV Tri DotDocument4 pagesManual HIV Tri DotDr.Soumen Saha100% (1)
- Certificate of Performance For Anesthesia Machine: Medicover HospitalsDocument1 pageCertificate of Performance For Anesthesia Machine: Medicover HospitalsIKON RESPONSE0% (1)
- Doctors Progress Note - Module 5Document4 pagesDoctors Progress Note - Module 5adrian nakilaNo ratings yet
- PusoDocument4 pagesPusoStephanie SundiangNo ratings yet
- Perioperative Fasting and Feeding in Adults, Obstetric, Paediatric and Bariatric Population-Practice Guidelines From The Indian Society of AnaesthesiologistsDocument29 pagesPerioperative Fasting and Feeding in Adults, Obstetric, Paediatric and Bariatric Population-Practice Guidelines From The Indian Society of Anaesthesiologistsambitiousamit1No ratings yet