Download as pdf or txt
You might also like
- Ecg Cheat Sheet 35Document2 pagesEcg Cheat Sheet 35jessjaylee88% (8)
- ECG InterpretationDocument95 pagesECG InterpretationNur Rahmat Wibowo100% (10)
- FRACP Written Exam Otago MCQ Book 2016Document470 pagesFRACP Written Exam Otago MCQ Book 2016Qiliang Liu100% (2)
- ECG Interpretations DR RPDocument109 pagesECG Interpretations DR RPArnis Putri RosyaniNo ratings yet
- Dysrhythmia Recognition Pocket Reference Card PDFDocument14 pagesDysrhythmia Recognition Pocket Reference Card PDFjenn1722100% (2)
- Cardiology Ekg BoardDocument87 pagesCardiology Ekg BoardPutri WijayaNo ratings yet
- Forensic Science Chapter 2 Notes: 2-1 Processing The Crime SceneDocument6 pagesForensic Science Chapter 2 Notes: 2-1 Processing The Crime SceneVonAllenBatarioNo ratings yet
- ECG PresentationDocument67 pagesECG PresentationSuresh ChevagoniNo ratings yet
- Presentasi Ws Ekg SakinahDocument40 pagesPresentasi Ws Ekg SakinahsiskaNo ratings yet
- Abnormal ECG 1Document26 pagesAbnormal ECG 1Apriliani Nur Puspita SariNo ratings yet
- Abnormal Electrocardiography: Dr. Andi Sulistyo Haribowo, SP - PDDocument133 pagesAbnormal Electrocardiography: Dr. Andi Sulistyo Haribowo, SP - PDShofiyyatunnisa' WsNo ratings yet
- Common ECGsDocument40 pagesCommon ECGsTejwani MuskanNo ratings yet
- Abnormal ECG 1Document26 pagesAbnormal ECG 1Apriliani Nur Puspita SariNo ratings yet
- ELECTROCARDIOGRAMDocument63 pagesELECTROCARDIOGRAMMbah GapinbissiNo ratings yet
- Basics and Interpretation: Sif HansdottirDocument65 pagesBasics and Interpretation: Sif Hansdottirwenny1186100% (1)
- Read ECGDocument128 pagesRead ECGrehmatakuNo ratings yet
- Technical AspectsDocument4 pagesTechnical AspectsNathan T. CheungNo ratings yet
- ARITMIA, Gangguan Irama JantungDocument37 pagesARITMIA, Gangguan Irama JantungNovriefta NugrahaNo ratings yet
- ElectrocardiogramDocument169 pagesElectrocardiogramjitendra magarNo ratings yet
- The Normal ElectrocardiogramDocument63 pagesThe Normal ElectrocardiogramPuravin Crishan VeerasamyNo ratings yet
- ECGDocument198 pagesECGKatrina Maravilla100% (1)
- Cardiology/EKG Board Review: Michael J. Bradley D.O. DME/Program Director Family Medicine ResidencyDocument87 pagesCardiology/EKG Board Review: Michael J. Bradley D.O. DME/Program Director Family Medicine ResidencyummimalikihamidNo ratings yet
- Superimposed ECG PDFDocument93 pagesSuperimposed ECG PDFEdalyn CapiliNo ratings yet
- Kuliah EKG Blok Kegawatdaruratan September 2018Document122 pagesKuliah EKG Blok Kegawatdaruratan September 2018khanzaisdiharanaNo ratings yet
- Workshop Pit IV THN 2017Document57 pagesWorkshop Pit IV THN 2017anettepardedeNo ratings yet
- 3881 - Prosedur Pendaftaran Internship Per November 2016Document57 pages3881 - Prosedur Pendaftaran Internship Per November 2016Munawir_Syam91No ratings yet
- ECG Basics Lecture 1Document116 pagesECG Basics Lecture 1AreebaNo ratings yet
- Normal ECGDocument63 pagesNormal ECGMohd Johari Mohd ShafuwanNo ratings yet
- EKG Common Clinical ArrhythmiasDocument54 pagesEKG Common Clinical ArrhythmiasFaisal AlhasNo ratings yet
- Gaje SinghDocument70 pagesGaje SinghgemergencycareNo ratings yet
- Ecg Interpretation:: The BasicsDocument40 pagesEcg Interpretation:: The BasicsRavi SharmaNo ratings yet
- PacemakerDocument156 pagesPacemakerDhruv DesaiNo ratings yet
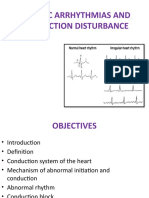
- Cardiac Arrhythmias and Conduction DisturbanceDocument42 pagesCardiac Arrhythmias and Conduction DisturbanceassumptaNo ratings yet
- Topnotch ECG Interpretation For MoonlightersDocument25 pagesTopnotch ECG Interpretation For Moonlightersmefav7778520100% (1)
- EKG 12 Leads: Internal Medicine 2010Document59 pagesEKG 12 Leads: Internal Medicine 2010M Lukman HakimNo ratings yet
- Basics of ECG: By-Pallavi ChicholikarDocument115 pagesBasics of ECG: By-Pallavi ChicholikarBhakti WashilkarNo ratings yet
- EKG Eh Kasi GanitoDocument44 pagesEKG Eh Kasi GanitoAnonymous ic2CDkFNo ratings yet
- EKG Interpretasi Dan Lethal Aritmia: Aan NuraeniDocument34 pagesEKG Interpretasi Dan Lethal Aritmia: Aan NuraeniCitra Marchelina Novilini100% (1)
- Normal Impulse Conduction: Sinoatrial NodeDocument80 pagesNormal Impulse Conduction: Sinoatrial Nodesiusiuwidyanto100% (2)
- 35ekg 1Document103 pages35ekg 1Veerapong Vattanavanit100% (2)
- Tutorial in ECG: Dr. Chew Keng Sheng Emergency Medicine Universiti Sains MalaysiaDocument56 pagesTutorial in ECG: Dr. Chew Keng Sheng Emergency Medicine Universiti Sains Malaysiafeby_valNo ratings yet
- ECG UpdatedDocument115 pagesECG Updatedmominarasool7No ratings yet
- Cardiovascular AlterationsDocument46 pagesCardiovascular Alterationsaneesnair86No ratings yet
- ECG InterpretationDocument95 pagesECG InterpretationShiela Mae Lopez100% (11)
- ECG AbnormalDocument60 pagesECG Abnormalvidishmalaviya300No ratings yet
- ECG BookDocument232 pagesECG BooklaureeateNo ratings yet
- Normal R Wave - R Wave Height Gradually Increased Up To V4 and Then DecreaseDocument6 pagesNormal R Wave - R Wave Height Gradually Increased Up To V4 and Then DecreaseNabighah ZukriNo ratings yet
- PDF DocumentDocument40 pagesPDF DocumentsalikiqbalNo ratings yet
- Ecg Basics - NAVEENDocument65 pagesEcg Basics - NAVEENNaveen MathieuNo ratings yet
- Ecg 1Document40 pagesEcg 1doctorhanifNo ratings yet
- Nursing School EKGDocument43 pagesNursing School EKGRob Dickerson100% (1)
- THE Electrocardiogram (Ecg / Ekg) : By: DR Yasir MansouriDocument83 pagesTHE Electrocardiogram (Ecg / Ekg) : By: DR Yasir Mansourirofi modiNo ratings yet
- Deborah Goldstein Georgetown University Department of Internal MedicineDocument66 pagesDeborah Goldstein Georgetown University Department of Internal MedicineAltama L. SidartaNo ratings yet
- Ecg Crit - CareDocument55 pagesEcg Crit - CarekrismatactayNo ratings yet
- NURV 456 Telemetry Interpretation StudentDocument56 pagesNURV 456 Telemetry Interpretation StudentMarie Yi100% (2)
- Ecg in Congenital Heart DiseaseDocument129 pagesEcg in Congenital Heart DiseaseAbhinav KumarNo ratings yet
- Basic EKG 2: Dr. Wattana Wongtheptien M.D. Cardiologist Chiangrai Regional HospitalDocument79 pagesBasic EKG 2: Dr. Wattana Wongtheptien M.D. Cardiologist Chiangrai Regional HospitalVeerapong Vattanavanit0% (1)
- Wswecocekgdasar2018Document34 pagesWswecocekgdasar2018Hendra AbeitNo ratings yet
- APPROACH TO ACLS RHYTHMS by Dra. Adviento 11.11.16Document92 pagesAPPROACH TO ACLS RHYTHMS by Dra. Adviento 11.11.16Rye CalderonNo ratings yet
- CardiologyDocument99 pagesCardiologySimple LyricsNo ratings yet
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookFrom EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNo ratings yet
- Law Terms PDFDocument65 pagesLaw Terms PDFtarunaggarwal11No ratings yet
- Criminal Law (Arts. 1-237)Document124 pagesCriminal Law (Arts. 1-237)MiGay Tan-Pelaez95% (19)
- Affidavit of Arrest ExampleDocument2 pagesAffidavit of Arrest ExampleVonAllenBatario100% (6)
- UPDATED - Recruiting NHS Organisations and Contact Details Website - 23-24 - 0Document11 pagesUPDATED - Recruiting NHS Organisations and Contact Details Website - 23-24 - 0Naga MuthuNo ratings yet
- Wenzhou People's HospitalDocument14 pagesWenzhou People's HospitalOmega SonnadaraNo ratings yet
- MedDocument4 pagesMedMohamed AbbasNo ratings yet
- AnKing - Soze's Step 1 Master DeckDocument139 pagesAnKing - Soze's Step 1 Master DeckFeroz RaZa SoomrOoNo ratings yet
- Case 1 KCSDocument16 pagesCase 1 KCSswaleh breik misfirNo ratings yet
- Ischemic Heart Disease PWDocument13 pagesIschemic Heart Disease PWEunica RamosNo ratings yet
- Acls EcgDocument4 pagesAcls EcgScribdTranslationsNo ratings yet
- Treatment of Heart attack-हृदय घात का इलाज-by Shri Rajiv DixitDocument5 pagesTreatment of Heart attack-हृदय घात का इलाज-by Shri Rajiv Dixitvirendrak11100% (1)
- CPR PDFDocument37 pagesCPR PDFArdhi AgustjikNo ratings yet
- Coronary Artery DiseaseDocument20 pagesCoronary Artery DiseaseAli Aborges Jr.No ratings yet
- Chapter 28 - Management of Patients With Coronary Vascular DisordersDocument10 pagesChapter 28 - Management of Patients With Coronary Vascular DisordersMichael BoadoNo ratings yet
- Ebook Electrophysiology of Arrhythmias Practical Images For Diagnosis and Ablation 2Nd Edition Reginald T Ho MD Online PDF All ChapterDocument69 pagesEbook Electrophysiology of Arrhythmias Practical Images For Diagnosis and Ablation 2Nd Edition Reginald T Ho MD Online PDF All Chaptersarah.payne692100% (7)
- CardiologyDocument23 pagesCardiologyJunaid SabirNo ratings yet
- Liver BookDocument46 pagesLiver BookKaranjit Singh100% (1)
- Atrial Septal DefectDocument37 pagesAtrial Septal DefectAndi Dewi PratiwiNo ratings yet
- Medical Writing SampleDocument2 pagesMedical Writing SampleJusteena Kaithaparambil100% (1)
- The Medical Treatment of Cardiogenic Shock: Cardiovascular DrugsDocument7 pagesThe Medical Treatment of Cardiogenic Shock: Cardiovascular DrugsCarlos QuirogaNo ratings yet
- Constrictive Pericarditis - UpToDateDocument26 pagesConstrictive Pericarditis - UpToDateSebastian CastañedaNo ratings yet
- Medical Instrumentation II - Defib and PacemakerDocument14 pagesMedical Instrumentation II - Defib and PacemakerRula BastoniNo ratings yet
- Abstrak IsicamDocument22 pagesAbstrak IsicambgusjklNo ratings yet
- Personal StatementDocument1 pagePersonal StatementAlex Burcin100% (1)
- Sun002 PDFDocument8 pagesSun002 PDFmmmaw mmNo ratings yet
- Introduction To ECG For NursingDocument75 pagesIntroduction To ECG For NursingRashid AlHamdan100% (1)
- Empa RegDocument49 pagesEmpa RegB ShahNo ratings yet
- Cardiopulmonary ResuscitationDocument42 pagesCardiopulmonary ResuscitationDe EnNo ratings yet
- Second ExamDocument8 pagesSecond ExamMohnmad Zaitoon100% (1)
- Columbia NefroDocument55 pagesColumbia Nefrol3arneyNo ratings yet
- Textbook Arrhythmia Essentials Brian Olshansky Ebook All Chapter PDFDocument53 pagesTextbook Arrhythmia Essentials Brian Olshansky Ebook All Chapter PDFeric.bond985100% (19)
- Vivi FrailDocument28 pagesVivi FrailCătălina Mihaela DascăluNo ratings yet