Professional Documents
Culture Documents
Rodes Cabau 2015 Effect of Clopidogrel and Aspirin V
Rodes Cabau 2015 Effect of Clopidogrel and Aspirin V
Uploaded by
adriaran101Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Rodes Cabau 2015 Effect of Clopidogrel and Aspirin V
Rodes Cabau 2015 Effect of Clopidogrel and Aspirin V
Uploaded by
adriaran101Copyright:
Available Formats
Research
Original Investigation
Effect of Clopidogrel and Aspirin vs Aspirin Alone on Migraine
Headaches After Transcatheter Atrial Septal Defect Closure
The CANOA Randomized Clinical Trial
Josep Rodés-Cabau, MD; Eric Horlick, MD; Reda Ibrahim, MD; Asim N. Cheema, MD; Marino Labinaz, MD; Najaf Nadeem, MD; Mark Osten, MD;
Mélanie Côté, MSc; Josep Ramon Marsal, MSc; Donald Rivest, MD; Alier Marrero, MD; Christine Houde, MD
Supplemental content at
IMPORTANCE The occurrence of new-onset migraine attacks is a complication of jama.com
transcatheter atrial septal defect (ASD) closure. It has been suggested that clopidogrel may
reduce migraine attacks after ASD closure.
OBJECTIVE To assess the efficacy of clopidogrel, used in addition to taking aspirin, for the
prevention of migraine attacks following ASD closure.
DESIGN, SETTING, AND PARTICIPANTS Randomized, double-blind clinical trial performed in 6
university hospitals in Canada. Participants were 171 patients with an indication for ASD
closure and no history of migraine.
INTERVENTIONS Patients were randomized (1:1) to receive dual antiplatelet therapy
(aspirin + clopidogrel [the clopidogrel group], n = 84) vs single antiplatelet therapy
(aspirin + placebo [the placebo group], n = 87) for 3 months following transcatheter ASD
closure. The first patient was enrolled in December 2008, and the last follow-up was
completed in February 2015.
MAIN OUTCOMES AND MEASURES The primary efficacy outcome was the monthly number of
migraine days within the 3 months following ASD closure in the entire study population. The
incidence and severity of new-onset migraine attacks, as evaluated by the Migraine Disability
Assessment questionnaire, were prespecified secondary end points. A zero-inflated Poisson
regression model was used for data analysis.
RESULTS The mean (SD) age of the participants was 49 (15) years and 62% (106) were
women. Patients in the clopidogrel group had a reduced mean (SD) number of monthly
migraine days within the 3 months following the procedure (0.4 [95% CI, 0.07 to 0.69] days)
vs the placebo group (1.4 [95% CI, 0.54 to 2.26] days; difference, −1.02 days [95% CI, −1.94 to
−0.10 days]; incident risk ratio [IRR], 0.61 [95% CI, 0.41 to 0.91]; P = .04) and a lower
incidence of migraine attacks following ASD closure (9.5% for the clopidogrel group vs 21.8%
for the placebo group; difference, −12.3% [95% CI, −23% to −1.6%]; odds ratio [OR], 0.38
[95% CI, 0.15 to 0.89]; P = .03). Among patients with migraines, those in the clopidogrel
group had less-severe migraine attacks (zero patients with moderately or severely disabling
migraine attacks vs 37% [7 patients] in the placebo group; difference, −36.8% [95% CI,
−58.5% to −15.2%]; P = .046). There were no between-group differences in the rate of
patients with at least 1 adverse event (16.7% [14 patients] in the clopidogrel group vs 21.8%
[19 patients] in the placebo group; difference, −5.2% [95% CI, −17% to 6.6%]; P = .44).
CONCLUSIONS AND RELEVANCE Among patients who underwent transcatheter ASD closure,
the use of clopidogrel and aspirin, compared with aspirin alone, resulted in a lower monthly
frequency of migraine attacks over 3 months. Further studies are needed to assess
Author Affiliations: Author
generalizability and durability of this effect. affiliations are listed at the end of this
article.
TRIAL REGISTRATION clinicaltrials.gov Identifier: NCT00799045 Corresponding Author: Josep
Rodés-Cabau, MD, Quebec Heart
and Lung Institute, Laval University,
JAMA. 2015;314(20):2147-2154. doi:10.1001/jama.2015.13919 Quebec City, QC G1V 4G5, Canada
Published online November 9, 2015. (josep.rodes@criucpq.ulaval.ca).
(Reprinted) 2147
Copyright 2015 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 08/05/2019
Research Original Investigation Clopidogrel and Aspirin vs Aspirin Alone in Treating Migraine Headaches
T
he occurrence of new-onset migraine attacks has been anticoagulation receiving intravenous heparin. Transtho-
reported in approximately 15% of patients following racic echocardiography was performed at hospital discharge
transcatheter atrial septal defect (ASD) closure, with the and at 3 months following the procedure.
majority of initial episodes occurring within the days to weeks Patients were randomized (1:1) before the ASD closure pro-
following the procedure.1-10 cedure to receive either aspirin (80 mg/d) plus placebo (the pla-
Antithrombotic therapy following transcatheter ASD clo- cebo group) or aspirin (80 mg/d) plus clopidogrel (75 mg/d) (the
sure remains empirical, with aspirin for 6 months being com- clopidogrel group). Random block sizes were used to conceal
monly prescribed. Preliminary observational retrospective treatment allocation from the patients, and randomization was
studies have suggested an association with lower incidence and stratified by clinical center. The treatment was initiated (with-
severity of migraine headaches following ASD closure when out loading dose) within 24 hours prior to ASD closure and con-
ticlopidine or clopidogrel is added to aspirin treatment.7-10 Sub- tinued for 3 months thereafter. A headache diary was given to
sequently there has been a widespread use of dual antiplate- each patient at the time of randomization. Patients were asked
let therapy following ASD closure, although no randomized to indicate, on a daily basis, the occurrence of headache epi-
data have confirmed such observations. The objective of this sodes and describe the characteristics, duration, severity, and
study was to assess the effect of clopidogrel on preventing the medication used for headache relief. The occurrence of head-
occurrence and reducing the number of new-onset migraine ache episodes was also assessed at 1- and 3-month follow-up
headache episodes following transcatheter ASD closure in pa- using a structured migraine headache questionnaire, which in-
tients with no history of migraine headaches. cluded the Migraine Disability Assessment (MIDAS) question-
naire (grade I [score of 0-5] indicates little or no disability, grade
II [score, 6-10] mild disability, grade III [score, 11-20] moder-
ate disability, and grade IV [score ≥21] severe disability). The
Methods questionnaires were provided by the study coordinator of each
Study Design and Patients participating center. All questionnaires and headache diaries
This was a randomized, double-blind clinical trial. CANOA were evaluated by 2 neurologists blinded to procedural de-
(Clopidogrel for the Prevention of New-Onset Migraine Head- tails and treatment allocation. If headache episodes oc-
ache Following Transcatheter Closure of Atrial Septal De- curred, the diagnosis of migraine attacks was established ac-
fects) was conducted in 6 centers in Canada, and it was ap- cording to the International Headache Society criteria.11 Also,
proved by Health Canada and the local ethics committee of each migraine attacks were further classified as with or without aura.
participating center. All patients provided written informed
consent for trial participation (trial protocol reported in Efficacy Outcomes
Supplement 1). The primary efficacy outcome was the monthly number of
The study included patients aged 18 years and older with new-onset migraine attacks within the 3 months following ASD
a clinical indication for transcatheter ASD closure. Within the closure in the entire study population. Secondary efficacy end
60 days prior to undergoing the procedure, each patient com- points were the incidence of new-onset migraine attacks, total
pleted a structured migraine headache questionnaire (eAp- number of migraine attacks during the first month and 3-month
pendix 1 in Supplement 1), which was subsequently evalu- period following ASD closure (the entire population and pa-
ated by a neurologist to determine whether a history of tients with migraine attacks only), monthly number of new-
migraine headaches was present. Patients with a history of mi- onset migraine attacks within 3 months following ASD clo-
graine headaches, based on the International Headache Soci- sure in patients with migraine attacks only, severity of migraine
ety criteria,11 were excluded. Other exclusion criteria were al- attacks as evaluated by the MIDAS questionnaire at 3-month
lergy or intolerance to any of the antithrombotic drugs used follow-up, and time to first migraine episode. Secondary safety
in the study (aspirin, clopidogrel), need for anticoagulation end points included the incidence of adverse events (re-
therapy, previous stroke, pregnancy or breastfeeding, not using corded at 1- and 3-month follow-up) including death, tran-
an effective method of birth control in premenopausal women, sient ischemic attack, stroke, bleeding complications, and ad-
use of ASD closure devices other than the Amplatzer Septal Oc- verse drug reactions.
cluder device (St Jude Medical), unsuccessful ASD closure (de- There were no changes to methods or trial outcomes af-
fined as no device implanted at the time of the procedure), and ter the trial commenced.
failure to provide informed consent.
The transcatheter ASD closure procedure has been de- Statistical Analyses
scribed in detail in prior studies.12 The procedure was per- Based on previous studies,3,4,9 we anticipated an incidence of
formed though transfemoral venous approach under guid- 15% of new-onset migraine attacks following ASD closure, with
ance of echocardiography (transesophageal or intracardiac). a median (interquartile range [IQR]) number of 5 (IQR, 1-23) mi-
Following the measurement of the ASD size by echocardiog- graine days per month within the 3 months following the pro-
raphy, a further assessment of the ASD size was performed by cedure among patients with migraine attacks. The addition of
inflation of a sizing balloon within the ASD defect, which de- clopidogrel therapy was expected to reduce the incidence and
termined the size of the ASD closure device. Device implan- number of migraine headaches by at least 50%.3,7 Consider-
tation was performed using current techniques. The proce- ing that a substantial number of patients were not expected
dures were performed while the patient was under full to have migraine attacks following ASD closure, the mean num-
2148 JAMA November 24, 2015 Volume 314, Number 20 (Reprinted) jama.com
Copyright 2015 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 08/05/2019
Clopidogrel and Aspirin vs Aspirin Alone in Treating Migraine Headaches Original Investigation Research
ber of migraine days per month by patient (including those who
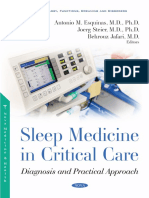
Figure 1. Flowchart of the CANOA Study Population
did not have migraine attacks) was modeled by a mixture of
zero-truncated Poisson distribution and zero-constant distri-
291 Patients assessed for eligibility
bution, which was calculated with a logistic model (SAS Proc
Genmod program).13 The power of the test was computed for 71 Excluded (history of migraines)
several sample sizes by Monte Carlo simulations, and a total
number of 70 patients per group were estimated to provide 220 Randomized
80% power to detect differences between groups. To account
for a potential dropout rate of approximately 10%, the sample
109 Randomized to receive aspirin 111 Randomized to receive aspirin
size was increased to 160 patients. + clopidogrel + placebo
Qualitative variables were expressed as percentages and 84 Received intervention as 87 Received intervention as
randomized randomized
quantitative variables as mean (SD) or median (IQR). Qualita- 25 Did not receive intervention 24 Did not receive intervention
tive variables were compared using the χ2 or Fisher exact test. 10 ASD closure unsuccessful 9 ASD closure unsuccessful
6 ASD closure not attempted 11 ASD closure not attempted
Comparison of numerical baseline and procedural variables and 9 Informed consent 4 Informed consent
migraine variables (number of migraine days) within the group withdrawn withdrawn
of patients with new-onset migraine attacks was performed
Follow-up Follow-up
using the t test or Mann-Whitney rank-sum test depending on 8 Did not complete treatment 8 Did not complete treatment
variable distribution. Comparison of the mean number of 5 Adverse events (treatment 4 Adverse events (treatment
stopped by investigator) stopped by investigator)
monthly migraine days and total number of migraine days at 3 Reasons unknown (treatment 4 Reasons unknown (treatment
1- and 3-month follow-up in the entire study population (with stopped by patient) stopped by patient)
and without migraines) were performed using the zero-
inflated Poisson (ZIP) regression model. ZIP models provide 84 Included in primary analysis 87 Included in primary analysis
the methodology to explain the excess zeros by modeling the
data as a mixture of 2 separate distributions: first, a Poisson ASD indicates atrial septal defect.
distribution to model the counts among the patients who had
at least 1 migraine attack; and second, a logistic regression to because the patient declined to continue in the study after ASD
model the occurrence (or not) of new-onset migraine epi- closure (n = 13). The final study population consisted of 171 pa-
sodes. The effects estimated are incident risk ratios (IRRs) for tients: 87 in the placebo group, and 84 patients in the clopi-
the Poisson distribution, which can be interpreted as the ra- dogrel group. A total of 155 patients (91%) were adherent with
tio of expected mean number of migraine days per month dur- the treatment during the study period (>80% of tablets taken
ing the 3 months compared between the placebo and clopi- as scheduled during the study period, as determined by tab-
dogrel groups and the odds ratio (OR) for the logistic model. let count). The treatment was temporarily or definitely stopped
Additionally, the effect of the treatment on the new-onset mi- by the investigator due to adverse events in 9 patients and by
graine attacks was estimated using logistic regression. For the the patients (for unknown reasons) in 7 patients.
other 2 secondary end points (total migraine days at the first The baseline and procedural characteristics of the study
month and at 3 months), a ZIP model was also used. population, according to treatment allocation, are reported in
Excluding the patients nonadherent to allocated treat- Table 1. The mean (SD) age of the study population was 49 (15)
ment, the efficacy analyses were repeated. Differences were years, and 106 (62%) patients were women. The mean size of
considered statistically significant at P values of less than .05 the ASD was 16.3 (5.5) mm, as measured by transesophageal
(2-tailed). No type-I error from multiple comparisons of sec- echocardiography, and 20.9 (5.7) mm by balloon measure-
ondary outcomes was addressed in the analyses and the re- ment. The median device size was 22 (IQR, 18-26) mm. There
sults from these analyses should be interpreted as explor- were no significant between-group differences regarding base-
atory. The data were analyzed using SAS version 9.1.3 and line and procedural characteristics.
RStudio version 0.98.953. A total of 27 patients (15.8%) had the diagnosis of new-
onset migraine attacks within the 3 months following the pro-
cedure (14 [52%] of them with aura). In these patients, the me-
dian number of total migraine days was 12 (IQR, 6-20), and the
Results median monthly number of migraine days was 4 (IQR, 2-7). The
The flow of patient participation through the trial is shown in primary and secondary efficacy end points for the entire study
Figure 1. Patients were enrolled from December 2008 to No- population are shown in Table 2. The mean (95% CI) number
vember 2014, and the last patient follow-up was completed in of monthly migraine days (primary outcome) was lower in the
February 2015. A total of 291 patients diagnosed with an ASD clopidogrel group (0.4 [95% CI, 0.07 to 0.69] days) than in the
for whom transcatheter ASD closure was planned were placebo group (1.4 [95% CI, 0.54 to 2.26] days; difference, −1.02
screened. Of these, 71 patients (24%) were excluded because days [95% CI, −1.94 to −0.10]; IRR, 0.61 [95% CI, 0.41 to 0.91];
of a history of migraine attacks and were included in a pro- P = .04). The incidence of new-onset migraine attacks was
spective migraine registry. Additionally, 49 patients were ex- lower in the clopidogrel group (9.5% [8] of patients) than in
cluded at the time of the procedure because device implanta- the placebo group (21.8% [19] of patients; difference, −12.3%
tion was not attempted (n = 17), was unsuccessful (n = 19), or [95% CI, −23% to −1.6%]; OR, 0.38 [95% CI, 0.15 to 0.89];
jama.com (Reprinted) JAMA November 24, 2015 Volume 314, Number 20 2149
Copyright 2015 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 08/05/2019
Research Original Investigation Clopidogrel and Aspirin vs Aspirin Alone in Treating Migraine Headaches
tient in the placebo group received preventive medication (ami-
Table 1. Baseline and Procedural Characteristics of the Study Population
tripyline) during the study period. A total of 77 patients had
Treatment Group, No (%)a nonmigraine headaches within the 3 months following the
Aspirin + Clopidogrel Aspirin + Placebo transcatheter ASD closure procedure, 41 patients (49%) in the
(n = 84) (n = 87)
Age, mean (SD), y 49 (16) 48 (15)
aspirin + clopidogrel group, and 36 patients (41%) in the aspi-
rin group, P = .36.
Male sex 36 (42.9) 29 (33.3)
The main outcomes, excluding the nonadherent patients
Smoker 11 (12.9) 11 (13.1)
(ie, <80% of treatment tablets taken as scheduled during the
Hypertension 20 (23.8) 24 (27.6)
study period, n = 16), are shown in eTables 1 and 2 in
Diabetes 5 (5.9) 8 (9.2)
Supplement 2. A total of 155 patients were adherent with the
New York Heart Association class
treatment during the study period (76 in the clopidogrel group,
I 68 (82.9) 61 (73.5)
79 in the placebo group). The mean (SD) number of migraine
II 12 (14.6) 19 (22.9)
days per month within the 3 months following ASD closure was
III or IV 2 (2.4) 3 (3.6)
lower in the clopidogrel group (0.4 [1.4] days) than in the pla-
Pulmonary pressure, mean (SD), 20.4 (5.6) 22.4 (6.3) cebo group (1.6 [4.3] days; difference, −1.2 days [95% CI, −2.2
mm Hg
Qp/Qs ratio, mean (SD) 1.93 (0.84) 1.89 (0.81)
to −0.19]; IRR, 0.58 [95% CI, 0.38 to 0.90]; P = .02). Also, the
incidence of migraine attacks was lower in the clopidogrel
Atrial septal aneurysm 11 (15.5) 11 (16.4)
group (9.2% [7] of patients) than in the aspirin group (24.1%
ASD size, mean (SD), mm
[19] of patients; difference, −14.8% [95% CI, −26.3% to −3.4%];
Measured by TEE 15.7 (5.7) 16.9 (5.7)
OR, 0.32 [95% CI, 0.13 to 0.81]; P = .02).
Measured by balloon 20.3 (6.3) 21.7 (5.3)
The occurrence and type of adverse events during the trial,
Device size, median (IQR), mm 22 (18-26) 22 (19-28)
according to treatment allocation, are shown in Table 4. There
Hospitalization length, 1 (1-1) 1 (1-1)
median (IQR), d were no deaths or stroke events during the entire study pe-
Residual shunt 27 (32.1) 26 (29.8) riod. One patient in the placebo group experienced a tran-
(hospital discharge) sient ischmic attack. There were no between-group differ-
b
Mild 26 (30.1) 25 (28.7) ences in the occurrence of bleeding complications (no major
Moderate to severec 1 (1.2) 1 (1.1) bleeding events; and for minor bleeding, 5.9% in the clopido-
Residual shunt (3-mo follow-up) 8 (12.7) 9 (10.3) grel group vs 1.2% in the placebo group [difference, 4.8% {95%
Mildb 8 (12.7) 8 (9.2) CI, −0.7% to 10.3%}]; P = .11). The rate of patients with any ad-
Moderate to severec 0 1 (1.1) verse event throughout the study period was similar be-
Abbreviations: ASD, atrial septal defect; IQR, interquartile range; tween groups (16.7% [14 patients] in the clopidogrel group vs
Qp/Qs, pulmonary flow/systemic flow ratio; 21.8% [19 patients] in the placebo group [difference, −5.2%
TEE, transesophageal echocardiography. [95% CI, −17.0% to 6.6%]; P = .44).
a
Values are reported as No. (%) unless otherwise indicated.
b
Mild if color jet width (Doppler echocardiography) is 2 mm or less.14
c
Moderate to severe if color jet width (Dopler echocardiography) is greater
than 2 mm.14 Discussion
Dual antiplatelet therapy (aspirin + clopidogrel) following
P = .03. The secondary efficacy end points for the group of pa- transcatheter ASD closure was associated with a statistically
tients with migraine attacks following ASD closure (n = 27) are significant reduction in the occurrence and number of new-
shown in Table 3. In the presence of migraine attacks follow- onset migraine headaches within the 3 months following the
ing ASD closure, the addition of clopidogrel was associated with procedure. Among patients with migraine attacks, those on
a reduced migraine severity (as evaluated by the MIDAS ques- dual antiplatelet therapy tended to experience less-severe mi-
tionnaire [zero patients in the clopidogrel group had moder- graine attacks. No significant increase in adverse events was
ate or severe disabling migraine attacks vs 36.8% {7 patients} observed with the use of dual vs single antiplatelet therapy.
in the placebo group; difference, −36.8% {95% CI, −58.5% to Transcatheter ASD closure has been well established as the
−15.2%}]; P = .046). There were no between-group differ- treatment of choice for most patients with hemodynamically
ences regarding the type of migraine (aura vs no aura), mi- significant ASD. This treatment offers a very high success rate
graine duration, or time to first migraine episode. Figure 2 together with an extremely low rate of complications (includ-
shows the timing of the first and subsequent migraine at- ing cerebrovascular events), and the minimally invasive ap-
tacks during the 3 months following ASD closure according to proach, when compared with surgery, allows a much more
treatment allocation. In the clopidogrel group, 6 patients (75%) rapid recovery.14 This combination of high success rate, low
received paracetamol during the migraine episodes. In the as- rate of complications, and more rapid recovery rate is of par-
pirin group, 16 patients (84%) received analgesic therapy dur- ticular importance considering that most adult patients re-
ing the migraine attacks, distributed as follows: acetamino- ceiving this treatment are of the working age. However, a limi-
phen/paracetamol (10 patients), ibuprofen (4 patients), tation of transcatheter ASD closure is the occurrence of
ibuprofen + acetaminophen/paracetamol (1 patient), and apo- migraine attacks—affecting approximately 15% patients and ex-
tramadol + acetaminophen/paracetamol (1 patient). One pa- tending to approximately 1 week per month during the first
2150 JAMA November 24, 2015 Volume 314, Number 20 (Reprinted) jama.com
Copyright 2015 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 08/05/2019
Clopidogrel and Aspirin vs Aspirin Alone in Treating Migraine Headaches Original Investigation Research
Table 2. Occurrence and Number of New-Onset Migraine Attacks Within the 3 Months Following ASD Closure
Treatment Group (95% CI)
Aspirin + Aspirin +
Clopidogrel Placebo Difference IRR OR
(n = 84) (n = 87) (95% CI) (95% CI)a P Value (95%CI)b P Value
Migraine days, mean (SD) [95% CI]
Days per mo (primary outcome) 0.4 (1.4) 1.4 (4.1) −1.02 0.61 .04 0.39 .02
[0.07 to 0.69] [0.54 to 2.26] (−1.94 to −0.10) (0.41 to 0.91) (0.16 to 0.95)
Days (first mo) 0.5 (2.2) 1.5 (4.5) −1.01 0.84 .34 0.33 .02
[0.02 to 0.96] [0.57 to 2.43] (−2.06 to 0.04) (0.59 to 1.20) (0.13 to 0.83)
Total migraine days at 3 mo 1.0 (4.1) 3.8 (10.6) −2.74 0.61 <.001 0.38 .03
[0.12 to 1.88] [1.5 to 5.95] (−5.14 to −0.34) (0.48 to 0.77) (0.16 to 0.92)
New-onset migraine attacks, No. (%) 8 (9.5) 19 (21.8) −12.3% 0.38 .03
(−23.0% to −1.6%) (0.15 to 0.89)
With aura 3 (37.5) 11 (57.9) −20.4% .33
(−60.6% to 19.8%)
Abbreviations: IRR, incidence risk ratio; OR, odds ratio.
a
Zero-inflated Poisson regression model (number of migraine attacks).
b
Zero-inflated Poisson regression model (probability of migraine attacks).
Table 3. Migraine Characteristics in Patients With Migraine Headaches
Treatment Group
Aspirin + Clopidogrel Aspirin + Placebo Difference
(n = 8) (n = 19) (95% CI) P Value
Migraine, median (IQR)
Days per mo 3.5 (2 to 5) 5 (2 to 8) −2.5 (−7.7 to 2.7) .39
Days (first mo) 3.5 (1 to 9) 4 (2 to 9) −1.8 (−7.9 to 4.2) .31
Days (3 mo) 7 (5 to 14.5) 13 (6 to 20) −6.8 (−20.1 to 6.5) .30
Migraine duration, median (IQR), 4 (3.5 to 5.5) 4 (3 to 6) −2.4 (−6.6 to 1.7) .94
hours per attack
Aura, No. (%) 3 (37.5) 11 (57.9) −20.4% (−60.6% to 19.8%) .33
Time to first migraine attack, 7 (5 to 15) 4 (2 to 15) 4.4 (−8.1 to 17.0) .42
median (IQR), days from procedure
MIDAS, No. (%)
I-II 8 (100) 12 (63.2) .046
−36.8% (−58.5% to −15.2%)
III-IVa 0 7 (36.8)
Abbreviations: IQR, interquartile range; MIDAS, Migraine Disability Assessment.
a
Moderate or severe disabling migraine attacks.
months following the procedure.1-10 This limitation repre- clopidogrel treatment should be 3 months or longer follow-
sents a significant burden of medical consultations in addi- ing ASD closure will need to be determined in future studies.
tion to missed work or school days and reduced productivity. Also, no loading dose of clopidogrel was used in this trial; the
The present study, which to our knowledge is the first ran- potential additional effect of a loading dose of clopidogrel on
domized trial in this field, confirmed prior observations on the the prevention of migraine headaches following ASD closure
incidence of migraine attacks following transcatheter ASD clo- needs to be further evaluated.
sure and demonstrated the usefulness of dual antiplatelet An association between interatrial shunts and migraine has
therapy for preventing and reducing, by more than 50%, the been put forward in various observational studies,15-17 and a
burden of such migraine episodes following the procedure. significant reduction of migraine attacks following percuta-
However, the reduction in monthly migraine days in the en- neous shunt closure has also been suggested.15,16 The random-
tire study population (0.4 days in the clopidogrel broup vs 1.4 ized trials evaluating the effects of atrial shunt closure on pa-
days in the placebo group) may appear modest due to the high tients with migraine headaches have provided controversial
number of patients with no migraine headaches after the pro- results, with negative or borderline primary outcomes and
cedure. Moreover, the addition of clopidogrel therapy re- some positive secondary outcomes like in the PRIMA trial.18,19
duced the severity of migraine episodes, with no patient in the Although the pathophysiology linking interatrial shunts and
dual antiplatelet therapy group presenting moderately or se- chronic migraine headaches is probably different from the one
verely disabling headache episodes compared with more than linking ASD closure with new-onset migraines, the results of
one-third of the patients receiving single antiplatelet therapy this trial should be considered when designing or analyzing the
(aspirin only). No increase in adverse events was observed with results of past, current, and future studies assessing the effi-
the addition of clopidogrel. Whether the optimal duration of cacy of interatrial shunt closure for the treatment of mi-
jama.com (Reprinted) JAMA November 24, 2015 Volume 314, Number 20 2151
Copyright 2015 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 08/05/2019
Research Original Investigation Clopidogrel and Aspirin vs Aspirin Alone in Treating Migraine Headaches
Figure 2. Timing of the First and Subsequent Migraine Attacks During the 3 Months Following ASD Closure
Aspirin + clopidogrel (8 individuals) Aspirin + clopidogrel
First migraine episode
Subsequent migraine episodes
Individual
Aspirin + placebo
First migraine episode
Subsequent migraine episodes
0 15 30 45 60 75 90
Days
Aspirin + placebo (19 individuals)
Individual
0 15 30 45 60 75 90 The first vertical column of data
Days markers on the left indicates day 1.
Day 0 was the day of ASD closure.
Table 4. Adverse Events at 3-Month Follow-up
Treatment Group, No. (%)
Aspirin + Clopidogrel Aspirin + Placebo Difference
Adverse Eventsa (n = 84) (n = 87) (95% CI) P Value
a
Zero patients in either group
Transient ischemic attack 0 1 (1.2) −1.1 (−3.4 to 1.1) >.99
experienced adverse events of
b
Minor bleeding 5 (5.9) 1 (1.2) 4.8 (−0.7 to 10.3) .11 death, pericardial effusion, device
Access site complications 0 1 (1.2) −1.1 (−3.4 to 1.1) >.99 embolization, need for cardiac
surgery, device thrombosis, or
Phlebitis 0 1 (1.2) −1.1 (−3.4 to 1.1) >.99
stroke during the study period.
Atrial fibrillation 2 (2.4) 5 (5.8) −3.4 (−9.2 to 2.5) .44 b
Minor adverse events associated
Palpitations 4 (4.8) 6 (6.9) −2.1 (−9.1 to 4.9) .75 with bleeding included epistaxis
Vertigo 0 2 (2.3) −2.3 (−5.4 to 0.9) .49 (n = 4), gingival bleeding (n = 1), and
minor hematuria (n = 1). There were
Cutaneous rash 3 (3.6) 2 (2.3) 1.3 (−3.8 to 6.3) .68
zero major bleeding adverse events.
graines. The addition of clopidogrel to the treatment of pa- subsets of patients,20,26 but 2 randomized studies failed to dem-
tients allocated to the transcatheter shunt closure group must onstrate a significant effect of warfarin or clopidogrel on migraine
be considered as a potential confounding factor that may lead attacks.27,28 The present study showed that in the presence of
to overestimating the real effect of shunt closure in such pa- a specific trigger, clopidogrel may be highly effective in the pre-
tients. Spencer et al20 showed a significant positive effect of vention of migraine attacks. The occurrence of increased plate-
clopidogrel therapy on migraine patients with a patent fora- let aggregation following ASD closure has been demonstrated,29
men ovale before transcatheter closure. Migraine trials in this and this may have increased the release of substances such as
setting should consider adjusting for clopidogrel therapy in case serotonin or proinflammatory cytokines like interleukins 1, 6,
of unbalanced treatment between groups. and 8 and tumor necrosis factor α, which have been linked to
The effects of a specific antithrombotic regimen, such as the migraine attacks.23-25
use of clopidogrel on the occurrence of migraine attacks, pro- Apart from its antiplatelet effects, clopidogrel has also
vide further insight into the potential role of platelet-coagulation proven antioxidant and anti-inflammatory properties.30 Sev-
activation and prothrombotic status in the pathogenesis of mi- eral studies have also shown improved endothelial function
graine. The association between migraine and ischemic stroke and nitric oxide bioavailability with the use of clopidogrel.31-33
has been well established,21,22 and several studies have linked The vasoprotective effects through adenosine phosphate re-
migraine attacks with abnormalities of platelet morphology and ceptor blockade may also have played a role in the prevention
function and also with coagulation disorders.23-26 Some stud- of migraine attacks.34 Further studies to evaluate the patho-
ies have shown a reduction in migraine attacks with the use of physiology linking clopidogrel with antimigraine effects are
anticoagulation or antiplatelet (clopidogrel) therapy in specific warranted. Also, it remains to be elucidated whether the ef-
2152 JAMA November 24, 2015 Volume 314, Number 20 (Reprinted) jama.com
Copyright 2015 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 08/05/2019
Clopidogrel and Aspirin vs Aspirin Alone in Treating Migraine Headaches Original Investigation Research
fects of clopidogrel on migraine attacks are a class effect or a longer-term follow-up are needed to determine the tran-
specific to that medication. sient vs permanent behavior of new-onset migraine head-
aches after ASD closure.
Limitations
No platelet reactivity examinations were performed to evalu-
ate clopidogrel resistance,35 and thus it remains unknown
whether the patients with migraine attacks in the dual anti-
Conclusions
platelet group had some degree of clopidogrel resistance. These Among patients who underwent transcatheter ASD closure,
results were obtained in patients undergoing ASD closure with the use of clopidogrel and aspirin, compared with aspirin
the Amplatzer Septal Occluder device and may not apply to alone, resulted in a lower monthly frequency of migraine
other transcatheter ASD closure devices. Migraine headaches attacks over 3 months. Further studies are needed to assess
following ASD closure may decrease over time36; studies with generalizability and durability of this effect.
ARTICLE INFORMATION education, and administrative support from St Jude 9. Rodés-Cabau J, Mineau S, Marrero A, et al.
Published Online: November 9, 2015. Medical. The other authors report no disclosures. Incidence, timing, and predictive factors of
doi:10.1001/jama.2015.13919. Funding/Support: This study was funded by new-onset migraine headache attack after
unrestricted grants from Sanofi and St Jude Medical transcatheter closure of atrial septal defect or
Author Affiliations: Department of Cardiology, patent foramen ovale. Am J Cardiol. 2008;101(5):
Quebec Heart and Lung Institute, Quebec City, and a grant from the Foundation of the Quebec
Heart and Lung Institute. 688-692.
Quebec, Canada (Rodés-Cabau, Côté); Department
of Cardiology, Toronto General Hospital, Toronto, Role of the Funder/Sponsor: There was no role of 10. Kato Y, Kobayashi T, Ishido H, Hayashi T,
Ontario, Canada (Horlick, Osten); Department of any organization or sponsor in any of the following: Furuya D, Tanahashi N. Migraine attacks after
Cardiology, Montreal Heart Institute, Montreal, design and conduct of the study, collection, transcatheter closure of atrial septal defect.
Quebec, Canada (Ibrahim); Department of management, analysis, and interpretation of the Cephalalgia. 2013;33(15):1229-1237.
Cardiology, St. Michael’s Hospital, Toronto, Ontario, data, preparation, review, and approval of the 11. Headache Classification Subcommittee of the
Canada (Cheema); Department of Cardiology, manuscript, and decision to submit the manuscript International Headache Society. The International
Ottawa Heart Institute, Ottawa, Ontario, Canada for publication. Classification of Headache Disorders: 2nd edition.
(Labinaz); Department of Cardiology, Queen Cephalalgia. 2004; 24(suppl 1): 9-160.
Elizabeth II Health Sciences Centre, Halifax, Nova REFERENCES 12. Kazmouz S, Kenny D, Cao QL, Kavinsky CJ,
Scotia, Canada (Nadeem); Epidemiology Unit of the 1. Rodés-Cabau J, Molina C, Serrano-Munuera C, Hijazi ZM. Transcatheter closure of secundum atrial
Cardiology Department, Vall d'Hebron Hospital, et al. Migraine with aura related to the septal defects. J Invasive Cardiol. 2013;25(5):257-264.
Universitat Autonoma de Barcelona, Barcelona, percutaneous closure of an atrial septal defect.
Spain (Marsal); Department of Neurology, Hôtel 13. Palta M. Quantitative Methods in Population
Catheter Cardiovasc Interv. 2003;60(4):540-542. Health: Extensions of Ordinary Regression. Hoboken,
Dieu de Lévis, Quebec City, Quebec, Canada
(Rivest); Department of Neurology, Centre 2. Fernández-Mayoralas DM, Fernández-Jaén A, NJ: Wiley; 2003.
Hospitalier Universitaire Georges. L Dumont, Muñoz-Jareño N, Gutiérrez-Larraya F, Calleja-Pérez 14. Du ZD, Hijazi ZM, Kleinman CS, Silverman NH,
Moncton, New Brunswick, Canada (Marrero); B, San Antonio Arce V. Migraine symptoms related Larntz K; Amplatzer Investigators. Comparison
Department of Pediatric Cardiology, Centre to the percutaneous closure of an ostium between transcatheter and surgical closure of
Hospitalier Universitaire de Québec, Quebec City, secundum atrial septal defect: report of four secundum atrial septal defect in children and
Quebec, Canada (Houde). paediatric cases and review of the literature. adults: results of a multicenter nonrandomized trial.
Cephalalgia. 2007;27(6):550-556. J Am Coll Cardiol. 2002;39(11):1836-1844.
Author Contributions: Dr Rodés-Cabau and Ms
Côté had full access to all the data in the study and 3. Mortelmans K, Post M, Thijs V, Herroelen L, 15. Lip PZ, Lip GY. Patent foramen ovale and
take responsibility for the integrity of the data and Budts W. The influence of percutaneous atrial migraine attacks: a systematic review. Am J Med.
the accuracy of the data analysis. septal defect closure on the occurrence of migraine. 2014;127(5):411-420.
Study concept and design: Rodés-Cabau. Eur Heart J. 2005;26(15):1533-1537.
16. Luermans JG, Post MC, Temmerman F, et al.
Acquisition, analysis, or interpretation of data: 4. Yew G, Wilson NJ. Transcatheter atrial septal Is a predominant left-to-right shunt associated with
Rodés-Cabau, Horlick, Ibrahim, Cheema, Labinaz, defect closure with the Amplatzer septal occluder: migraine?: a prospective atrial septal defect closure
Nadeem, Osten, Coté, Marsal, Rivest, Marrero, five-year follow-up. Catheter Cardiovasc Interv. study. Catheter Cardiovasc Interv. 2009;74(7):
Houde. 2005;64(2):193-196. 1078-1084.
Drafting of the manuscript: Rodés-Cabau, Coté, 5. Wei SH, Fan PC, Kuo PH, Chiou LC, Wang JK.
Marsal. 17. Kato Y, Hayashi T, Kobayashi T, Tanahashi N.
Calcitonin gene-related peptide and size of the Migraine prevalence in patients with atrial septal
Critical revision of the manuscript for important atrial septal defect in new-onset migraine after
intellectual content: Rodés-Cabau, Horlick, Ibrahim, defect. J Headache Pain. 2013;14:63.
transcatheter closure: results of a preliminary study.
Cheema, Labinaz, Nadeem, Osten, Marsal, Rivest, Headache. 2012;52(6):985-992. 18. Dowson A, Mullen MJ, Peatfield R, et al.
Marrero, Houde. Migraine Intervention With STARFlex Technology
Statistical analysis: Coté, Marsal. 6. Castellini P, Lambru G, Manzoni GC, Torelli P. (MIST) trial: a prospective, multicenter,
Obtained funding: Rodés-Cabau. Atrial septal defect closure and migraine with aura: double-blind, sham-controlled trial to evaluate the
Administrative, technical, or material support: is there a correlation? Neurol Sci. 2009;30(4): effectiveness of patent foramen ovale closure with
Rodés-Cabau, Ibrahim, Cheema, Labinaz, Nadeem, 339-342. STARFlex septal repair implant to resolve refractory
Osten, Marsal, Rivest. 7. Sharifi M, Dehghani M, Mehdipour M, migraine headache. Circulation. 2008;117(11):
Study supervision: Rodés-Cabau, Horlick, Ibrahim, Al-Bustami O, Emrani F, Burks J. Intense migraines 1397-1404.
Nadeem, Osten, Marrero, Houde. secondary to percutaneous closure of atrial septal 19. Hildick-Smith D. Percutaneous closure of patent
Conflict of Interest Disclosures: All authors have defects. J Interv Cardiol. 2005;18(3):181-183. foramen ovale in migraine with aura—a randomized
completed and submitted the ICMJE Form for 8. Wilmshurst PT, Nightingale S, Walsh KP, prospective study (PRIMA trial). Transcatheter
Disclosure of Potential Conflicts of Interest. Dr Morrison WL. Clopidogrel reduces migraine with Cardiovascular Therapeutics Meeting, Washington,
Horlick reports receipt of honoraria for lectures aura after transcatheter closure of persistent DC, March 2014. http://www.sac.org.ar/wp-content
outside the submitted work from St Jude Medical foramen ovale and atrial septal defects. Heart. /uploads/2014/09/tct-2014-prima-a-prospective
and an institutional unrestricted grant for research, 2005;91(9):1173-1175. -randomized-trial.pdf. Accessed October, 2, 2015.
jama.com (Reprinted) JAMA November 24, 2015 Volume 314, Number 20 2153
Copyright 2015 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 08/05/2019
Research Original Investigation Clopidogrel and Aspirin vs Aspirin Alone in Treating Migraine Headaches
20. Spencer BT, Qureshi Y, Sommer RJ. 27. Wammes-van der Heijden EA, Smidt MH, double-blind, randomized study. Atherosclerosis.
A retrospective review of clopidogrel as primary Tijssen CC, van’t Hoff AR, Lenderink AW, Egberts 2008;196(2):689-695.
therapy for migraineurs with right to left shunt AC. Effect of low-intensity acenocoumarol on 32. Giachini FR, Leite R, Osmond DA, et al.
lesions. Cephalalgia. 2014;34(11):933-937. frequency and severity of migraine attacks. Anti-platelet therapy with clopidogrel prevents
21. Kurth T, Diener HC. Migraine and stroke: Headache. 2005;45(2):137-143. endothelial dysfunction and vascular remodeling in
perspectives for stroke physicians. Stroke. 2012;43 28. Chambers JB, Seed PT, Ridsdale L. Clopidogrel aortas from hypertensive rats. PLoS One. 2014;9(3):
(12):3421-3426. as prophylactic treatment for migraine: a pilot e91890.
22. Mawet J, Kurth T, Ayata C. Migraine and stroke: randomised, controlled study. Cephalalgia. 2014;34 33. Zhang YZ, Chen BL, Zhang W, Cao X.
in search of shared mechanisms. Cephalalgia. (14):1163-1168. Non-antiplatelet effect of clopidogrel: improving
2015;35(2):165-181. 29. Pan G, Xie ZF, Zhang Y, Long SC, Xu XP, endothelial function in Chinese healthy subjects
23. Borgdorff P, Tangelder GJ. Migraine: possible Zhang ZW. Platelet activation through the efficacy with different CYP2C19 genotype. Clin Exp
role of shear-induced platelet aggregation with of aspirin in congenital heart disease patients Pharmacol Physiol. 2015;42(1):22-26.
serotonin release. Headache. 2012;52(8):1298-1318. undergoing transcatheter closure of atrial septal 34. Tietjen GE. The role of the endothelium in
defects or ventricular septal defects. Genet Test Mol migraine. Cephalalgia. 2011;31(6):645-647.
24. Sarchielli P, Alberti A, Coppola F, et al. Biomarkers. 2014;18(12):832-838.
Platelet-activating factor (PAF) in internal jugular 35. Linden MD, Tran H, Woods R, Tonkin A.
venous blood of migraine without aura patients 30. Heitzer T, Rudolph V, Schwedhelm E, et al. High platelet reactivity and antiplatelet therapy
assessed during migraine attacks. Cephalalgia. Clopidogrel improves systemic endothelial nitric resistance. Semin Thromb Hemost. 2012;38(2):
2004;24(8):623-630. oxide bioavailability in patients with coronary artery 200-212.
disease: evidence for antioxidant and
25. Danese E, Montagnana M, Lippi G. Platelets antiinflammatory effects. Arterioscler Thromb Vasc 36. Voet A, Luermans JG, Thijs V, et al. New-onset
and migraine. Thromb Res. 2014;134(1):17-22. Biol. 2006;26(7):1648-1652. and persistent migraine early after percutaneous
26. Maggioni F, Bruno M, Mainardi F, Lisotto C, atrial septal defect closure disappear at follow-up.
31. Warnholtz A, Ostad MA, Velich N, et al. A single Acta Clin Belg. 2008; 63(4):262-268.
Zanchin G. Migraine responsive to warfarin: an loading dose of clopidogrel causes dose-dependent
update on anticoagulant possible role in migraine improvement of endothelial dysfunction in patients
prophylaxis. Neurol Sci. 2012;33(6):1447-1449. with stable coronary artery disease: results of a
2154 JAMA November 24, 2015 Volume 314, Number 20 (Reprinted) jama.com
Copyright 2015 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 08/05/2019
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Anticancer A New Way of LifeDocument5 pagesAnticancer A New Way of Lifenmgaby21No ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Physician To Population Ratios Physician Supply StandardsDocument5 pagesPhysician To Population Ratios Physician Supply StandardsjackeldescargadorNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- PHAR1014 W1 AKD Summary: Explain & Compare The Pathophysiology, Symptoms Presentation of Acute Kidney DiseaseDocument4 pagesPHAR1014 W1 AKD Summary: Explain & Compare The Pathophysiology, Symptoms Presentation of Acute Kidney DiseaseNancy ZengNo ratings yet
- 46s - Contraception TBL (Pearson - Dillon)Document13 pages46s - Contraception TBL (Pearson - Dillon)adriaran101No ratings yet
- GI Quiz 2 Study MapDocument3 pagesGI Quiz 2 Study Mapadriaran101No ratings yet
- Proteopathic Tau Seeding Predicts Tauopathy in Vivo: SignificanceDocument10 pagesProteopathic Tau Seeding Predicts Tauopathy in Vivo: Significanceadriaran101No ratings yet
- Active Study StrategiesDocument2 pagesActive Study Strategiesadriaran101No ratings yet
- N R P C ' H: Eurology Esidency Rogram Oordinator S AndbookDocument36 pagesN R P C ' H: Eurology Esidency Rogram Oordinator S Andbookadriaran101No ratings yet
- How To Make Anki Actually Shuffle CardsDocument2 pagesHow To Make Anki Actually Shuffle Cardsadriaran101No ratings yet
- 4 Pass Method For Success in Medical SchoolDocument2 pages4 Pass Method For Success in Medical Schooladriaran101No ratings yet
- Intervertebral Disc Degeneration Prevalence, Risk Factors and Treatments MasudDocument297 pagesIntervertebral Disc Degeneration Prevalence, Risk Factors and Treatments MasudAlban KrasniqiNo ratings yet
- Michael Angelo A. Nombre (BSN-2D) : "Medical Abbreviations On Pharmacy Prescriptions"Document25 pagesMichael Angelo A. Nombre (BSN-2D) : "Medical Abbreviations On Pharmacy Prescriptions"clint xavier odangoNo ratings yet
- OT HistoriesDocument14 pagesOT HistoriesFatimah AmirNo ratings yet
- PHECC Field Guide 2011Document125 pagesPHECC Field Guide 2011Michael B. San JuanNo ratings yet
- Serological Response To Myxomatosis Vaccination by Different Inoculations Systems On Farm RabbitsDocument12 pagesSerological Response To Myxomatosis Vaccination by Different Inoculations Systems On Farm RabbitsCamilaNo ratings yet
- Jack DanielDocument11 pagesJack DanielJack PresadoNo ratings yet
- Reiss Sandborn 2015 Role of Psychosocial CareDocument6 pagesReiss Sandborn 2015 Role of Psychosocial CareAgata AgniNo ratings yet
- AMC Medical FormDocument3 pagesAMC Medical FormSafiullah AhmadNo ratings yet
- Myoma Pathophysio, Gordon's NCPDocument13 pagesMyoma Pathophysio, Gordon's NCPicesexy100% (1)
- ASPAK Alkes IGDDocument2 pagesASPAK Alkes IGDAdra AdeNo ratings yet
- Sleep Medicine in Critical CareDocument335 pagesSleep Medicine in Critical CareDragutin PetrićNo ratings yet
- Therapeutics Handbook 2014 - 140804Document384 pagesTherapeutics Handbook 2014 - 140804Eriet HidayatNo ratings yet
- INstruction For Use Clover A1c Self PDFDocument33 pagesINstruction For Use Clover A1c Self PDFrossy tejaningsih100% (1)
- Viva Questions of Final Professional ExaminationDocument48 pagesViva Questions of Final Professional ExaminationFaisol KabirNo ratings yet
- Immunomodulators For AsthmaDocument7 pagesImmunomodulators For AsthmadarmariantoNo ratings yet
- Marlius Namala Merchiory: Course CertificateDocument1 pageMarlius Namala Merchiory: Course CertificateMarlius MerchioryNo ratings yet
- Arrhythmias Teacher GuideDocument12 pagesArrhythmias Teacher GuideMayer Rosenberg100% (3)
- Gene TherapyDocument19 pagesGene TherapyJhayce Christian S. CapanayanNo ratings yet
- Syllabus of PBM in OncologyDocument6 pagesSyllabus of PBM in OncologyMohd Anas SheikhNo ratings yet
- Allegations Against The Princess Alexandra Hospital by DR Romesh SenewiratneDocument17 pagesAllegations Against The Princess Alexandra Hospital by DR Romesh SenewiratneDr Romesh Arya ChakravartiNo ratings yet
- Naturopathy StandardDocument52 pagesNaturopathy Standardsujith stephenNo ratings yet
- Infectious Diseases For InternsDocument60 pagesInfectious Diseases For InternsMaya SwariNo ratings yet
- 2020 06 18 Coronavirus Covid 19 Infection in PregnancyDocument61 pages2020 06 18 Coronavirus Covid 19 Infection in PregnancyIndah AulliaNo ratings yet
- 3 AmphetaminesDocument4 pages3 AmphetaminesNouman Safdar AliNo ratings yet
- Ophthalmology Easy GuideDocument46 pagesOphthalmology Easy Guidesri sinaga0% (1)
- Chapter IiDocument11 pagesChapter IiKadek IstaNo ratings yet
- Biokimia II Kel 10 - Inborn Error of Lipid MetabolismDocument34 pagesBiokimia II Kel 10 - Inborn Error of Lipid MetabolismYafie Al IslamiNo ratings yet