Download as docx, pdf, or txt
You might also like
- Bailey & Scott's Diagnostic Microbiology, 13th Edition-Pages-1011-1034Document24 pagesBailey & Scott's Diagnostic Microbiology, 13th Edition-Pages-1011-1034JhanKarloFloresFlores0% (2)
- Chapter 19 Microbial Diseases of The Skin and WoundsDocument8 pagesChapter 19 Microbial Diseases of The Skin and WoundsGRACE MAR CABAHUG100% (1)
- Respiratory, USMLE ENDPOINT BY DR AHMED SHEBLDocument91 pagesRespiratory, USMLE ENDPOINT BY DR AHMED SHEBLDaNy Chiriac100% (3)
- Family Life Cycle PDFDocument2 pagesFamily Life Cycle PDFDon'tAsK TheStupidOnes100% (1)
- OxygenationDocument57 pagesOxygenationscent0730100% (3)
- Calorimetry Problems KeyDocument2 pagesCalorimetry Problems KeyDon'tAsK TheStupidOnesNo ratings yet
- Science of Vaccine DamageDocument35 pagesScience of Vaccine DamageLeonard Michlin50% (2)
- Tonsillitis, Peritonsillarand Lateralpharyngeal Abscesses: Jonathan M. Tagliareni,, Earl I. ClarksonDocument8 pagesTonsillitis, Peritonsillarand Lateralpharyngeal Abscesses: Jonathan M. Tagliareni,, Earl I. ClarksonAlfianRismawanNo ratings yet
- Respiratory System: Larynx EpiglottisDocument12 pagesRespiratory System: Larynx Epiglottisangel sychingNo ratings yet
- Rhinitis Is A Common Disease Worldwide Characterized by at Least One Symptom Between Nasal ObstructionDocument10 pagesRhinitis Is A Common Disease Worldwide Characterized by at Least One Symptom Between Nasal ObstructionWii YangNo ratings yet
- Respiratory SystemDocument43 pagesRespiratory SystemMaxxdlc 16No ratings yet
- Anatomy of AirwayDocument50 pagesAnatomy of AirwayHari Om ChaurasiyaNo ratings yet
- Pathohys II-respiratory DiseasesDocument89 pagesPathohys II-respiratory DiseasesSophia AbdullahNo ratings yet
- Head and Neck Triangles, Sub Mandibular, Parotid RegionDocument71 pagesHead and Neck Triangles, Sub Mandibular, Parotid RegionCupid MohNo ratings yet
- The PharynxDocument40 pagesThe PharynxDr-Firas Nayf Al-ThawabiaNo ratings yet
- Mycobacterium Avium and Mycobacterium Bovis Have Been Rarely Associated With TheDocument15 pagesMycobacterium Avium and Mycobacterium Bovis Have Been Rarely Associated With ThemaricelNo ratings yet
- Fundamental Concepts of Anesthesiology: Dr. Weiwei LiuDocument31 pagesFundamental Concepts of Anesthesiology: Dr. Weiwei Liusimple livingNo ratings yet
- (Lib-Ebooks Com) 240820202341 PDFDocument193 pages(Lib-Ebooks Com) 240820202341 PDFDr. Hisham Abdul MajeedNo ratings yet
- Ebook Respiratory Physiology Mosby Physiology Series PDF Full Chapter PDFDocument67 pagesEbook Respiratory Physiology Mosby Physiology Series PDF Full Chapter PDFkyle.heffner607100% (38)
- Respiratory SystemDocument5 pagesRespiratory SystemJay QuilnetNo ratings yet
- Case Study PneumoniaDocument13 pagesCase Study Pneumonialavparedes93% (44)
- Anatomy and Physiology of Respiratory SystemDocument21 pagesAnatomy and Physiology of Respiratory Systemsameeha semiNo ratings yet
- Respiratory SystemDocument38 pagesRespiratory SystemNashreen QtqtNo ratings yet
- The Respiratory SystemDocument61 pagesThe Respiratory SystemLuna JadeNo ratings yet
- Block 11 Tutorial Scenario C Mrs. A, A 29-Years Old House WifeDocument26 pagesBlock 11 Tutorial Scenario C Mrs. A, A 29-Years Old House Wiferio archuletaNo ratings yet
- Pcap C Case StudyDocument21 pagesPcap C Case StudyKate PedzNo ratings yet
- OXYGENATIONDocument10 pagesOXYGENATIONnicoleNo ratings yet
- Respiratory Physiology Mosby Physiology Series 2Nd Edition Edition Michelle M Cloutier All ChapterDocument67 pagesRespiratory Physiology Mosby Physiology Series 2Nd Edition Edition Michelle M Cloutier All Chaptervincent.pathak166100% (14)
- K1 - Upper and Lower Resp System - Sindhu Wisesa - ReK1Document74 pagesK1 - Upper and Lower Resp System - Sindhu Wisesa - ReK1Dessy Dwi ZNo ratings yet
- Medical Surgical Nursing Lecture 234 Pages Pg. 333 566Document189 pagesMedical Surgical Nursing Lecture 234 Pages Pg. 333 566Crystal Ann TadiamonNo ratings yet
- Dont BreathDocument43 pagesDont BreathDhruv GoswamiNo ratings yet
- Disorder of Respiratory SystemDocument89 pagesDisorder of Respiratory SystemDarine Nasr100% (1)
- Airway Anatomy &assessmentDocument44 pagesAirway Anatomy &assessmentAya AlefeshatNo ratings yet
- Pulmonology: Dr. Okon MRCSDocument28 pagesPulmonology: Dr. Okon MRCSEdwin OkonNo ratings yet
- LBM 5 THT SGD 15Document42 pagesLBM 5 THT SGD 15Akhmad Ulil AlbabNo ratings yet
- гортаньDocument47 pagesгортаньканизаNo ratings yet
- Embryology: Lung DevelopmentDocument91 pagesEmbryology: Lung DevelopmentPrarthanaNo ratings yet
- 2- الجاهزة20.02.2022 lower Respiratory system physiologyDocument32 pages2- الجاهزة20.02.2022 lower Respiratory system physiologybessan alfqeatNo ratings yet
- Respiratory SystemDocument72 pagesRespiratory SystemElaine Victoria ElizanNo ratings yet
- Benumof Anatomia Via AereaDocument11 pagesBenumof Anatomia Via AereaMaria RicardoNo ratings yet
- Broncho PneumoniaDocument23 pagesBroncho Pneumoniaanon-84769398% (43)
- Respiratory InfectionsDocument88 pagesRespiratory Infectionsambreensaba.btconNo ratings yet
- BRONCHIECTASISDocument40 pagesBRONCHIECTASISAnujNo ratings yet
- The Respiratory System: Raymund Christopher R. Dela Peña, RN, RM, MAN Clinical Faculty UNP-College of NursingDocument95 pagesThe Respiratory System: Raymund Christopher R. Dela Peña, RN, RM, MAN Clinical Faculty UNP-College of NursingrnrmmanphdNo ratings yet
- Pharyanx IDocument28 pagesPharyanx Ij8bhfmc6s9No ratings yet
- Anaphy Chapter 23 Respiratory System Doran MLS 1 FDocument9 pagesAnaphy Chapter 23 Respiratory System Doran MLS 1 FayenaNo ratings yet
- Subject Seminar ON Approach To StridorDocument68 pagesSubject Seminar ON Approach To StridorAimhigh_PPM100% (1)
- Upper Respiratory TractDocument6 pagesUpper Respiratory TractGeraldine Gallaron - CasipongNo ratings yet
- By (PG in ENT) : DR B.SowmyaDocument87 pagesBy (PG in ENT) : DR B.Sowmyadrchinna100% (1)
- Pharynx: Dr. U OfforDocument29 pagesPharynx: Dr. U OfforugochukwuNo ratings yet
- Upper Respiratory Tract AnatomyDocument61 pagesUpper Respiratory Tract Anatomyيحيى اسماعيل الجميليNo ratings yet
- Acute Respiratory InfectionsDocument145 pagesAcute Respiratory InfectionsManuel VIc O. Lacaya100% (1)
- Medical-Surgical-Nursing-2 2Document433 pagesMedical-Surgical-Nursing-2 2Pearly Rose V. ManlapasNo ratings yet
- High Resolution and High Definition Anorectal ManometryFrom EverandHigh Resolution and High Definition Anorectal ManometryMassimo BelliniNo ratings yet
- Thoracic Radiology: A Guide for BeginnersFrom EverandThoracic Radiology: A Guide for BeginnersIacopo CarboneNo ratings yet
- Pulmonary Manifestations of Primary Immunodeficiency DiseasesFrom EverandPulmonary Manifestations of Primary Immunodeficiency DiseasesSeyed Alireza MahdavianiNo ratings yet
- For Portfolio LS2 ScienceDocument7 pagesFor Portfolio LS2 ScienceDon'tAsK TheStupidOnesNo ratings yet
- For Portfolio LS6 Digital CitizenshipDocument4 pagesFor Portfolio LS6 Digital CitizenshipDon'tAsK TheStupidOnesNo ratings yet
- For Portfolio LS1 EnglishDocument5 pagesFor Portfolio LS1 EnglishDon'tAsK TheStupidOnesNo ratings yet
- Welcome General Chemistry For Engineering and TechnologistDocument9 pagesWelcome General Chemistry For Engineering and TechnologistDon'tAsK TheStupidOnesNo ratings yet
- Lesson 2 - Water, CarbohydratesDocument22 pagesLesson 2 - Water, CarbohydratesDon'tAsK TheStupidOnesNo ratings yet
- For Portfolio LS3 Mathematical and Problem Solving SkillsDocument8 pagesFor Portfolio LS3 Mathematical and Problem Solving SkillsDon'tAsK TheStupidOnesNo ratings yet
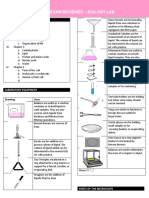
- Prelim Exam Reviewer - Biology Lab: by Team Meow Meow (Halimeow and 3 Headed Creature)Document7 pagesPrelim Exam Reviewer - Biology Lab: by Team Meow Meow (Halimeow and 3 Headed Creature)Don'tAsK TheStupidOnesNo ratings yet
- Principles of Biology I Lab ManualDocument75 pagesPrinciples of Biology I Lab ManualDon'tAsK TheStupidOnesNo ratings yet
- Quiz 1-ChemDocument2 pagesQuiz 1-ChemDon'tAsK TheStupidOnesNo ratings yet
- Quiz 2 - ChemDocument3 pagesQuiz 2 - ChemDon'tAsK TheStupidOnesNo ratings yet
- Lesson 1 - WHAT IS BIOLOGYDocument5 pagesLesson 1 - WHAT IS BIOLOGYDon'tAsK TheStupidOnesNo ratings yet
- Global Warming: Public Health Impacts and SolutionsDocument45 pagesGlobal Warming: Public Health Impacts and SolutionsDon'tAsK TheStupidOnesNo ratings yet
- Gibbs WorksheetDocument4 pagesGibbs WorksheetDon'tAsK TheStupidOnesNo ratings yet
- Int Ener SolnsDocument3 pagesInt Ener SolnsDon'tAsK TheStupidOnesNo ratings yet
- UNIVERSAL COLLEGE OF PARANAQUE. FinalsDocument26 pagesUNIVERSAL COLLEGE OF PARANAQUE. FinalsDon'tAsK TheStupidOnesNo ratings yet
- Bomb Calorimetry Practice ProblemsDocument2 pagesBomb Calorimetry Practice ProblemsDon'tAsK TheStupidOnesNo ratings yet
- RubellaDocument10 pagesRubellaKiran Kumar100% (1)
- Journal v12 n1 2020Document120 pagesJournal v12 n1 2020Fakhrizal AkbarNo ratings yet
- MeaslesDocument1 pageMeaslesDavid HylandNo ratings yet
- Mump EmedicineDocument15 pagesMump Emedicinekeyla_shineeeNo ratings yet
- White Paper Measles AIM v1.9Document40 pagesWhite Paper Measles AIM v1.9rush999No ratings yet
- 6 Human Diseases That Cause by VirusesDocument7 pages6 Human Diseases That Cause by VirusesJefry JapNo ratings yet
- Assessment 7Document5 pagesAssessment 7api-525782290No ratings yet
- Arbeitsheft 2018Document147 pagesArbeitsheft 2018Pamela MusabelliuNo ratings yet
- Me A S L E S: Aka Rubeola/ MorbilliDocument20 pagesMe A S L E S: Aka Rubeola/ MorbilliDayan CabrigaNo ratings yet
- CITY STAR December 2019 EditionDocument20 pagesCITY STAR December 2019 Editioncity star newspaperNo ratings yet
- Part4 Evidence1 CozineDocument2 pagesPart4 Evidence1 Cozineapi-286143658No ratings yet
- Communicable Diseases Exam Style Questions and Mark SchemeDocument16 pagesCommunicable Diseases Exam Style Questions and Mark SchemeSharonNo ratings yet
- High Dose Vitamin A ProtocolDocument17 pagesHigh Dose Vitamin A Protocolcosmopolita1No ratings yet
- Checklist - IMCI-Sick Young ChildDocument3 pagesChecklist - IMCI-Sick Young ChildAriel Delos ReyesNo ratings yet
- Knowledge, Attitude and Practice of Mothers Toward Children's Obligatory VaccinationDocument7 pagesKnowledge, Attitude and Practice of Mothers Toward Children's Obligatory VaccinationkrishnasreeNo ratings yet
- Planning of Individual and Family Health Nursing Care: Montibon Edelainne Joyce B Pila, Liza Aingelica BDocument25 pagesPlanning of Individual and Family Health Nursing Care: Montibon Edelainne Joyce B Pila, Liza Aingelica BLiza AingelicaNo ratings yet
- Personal Life EssayDocument8 pagesPersonal Life Essayafabfzoqr100% (2)
- Aczm Multiple Choice Exam Questions: HerpetofaunaDocument12 pagesAczm Multiple Choice Exam Questions: HerpetofaunaSergioVelezFNo ratings yet
- Research Essay: Hanoi UniversityDocument8 pagesResearch Essay: Hanoi UniversityHoàng Thị Thuỳ DươngNo ratings yet
- GCSE Biology Paper 1 2022 r6zr18Document54 pagesGCSE Biology Paper 1 2022 r6zr18joel1122wwNo ratings yet
- 42 National Science Olympiad: 9 March 2006 Questions and Solutions: BiologyDocument55 pages42 National Science Olympiad: 9 March 2006 Questions and Solutions: Biologymartynapet100% (2)
- Elements of EPIDocument2 pagesElements of EPIMichelle Gambol50% (2)
- Health Q3 M2Document15 pagesHealth Q3 M2olameonfrixandrei486No ratings yet
- Foundations in Microbiology: TalaroDocument76 pagesFoundations in Microbiology: Talaromertx013No ratings yet
- Measles: Late Winter, Early Spring and Rainy SeasonDocument10 pagesMeasles: Late Winter, Early Spring and Rainy SeasonReah Jayzel AlkuinoNo ratings yet
- AnnobibliDocument7 pagesAnnobibliapi-317692053No ratings yet
- Measles FM S 05072013Document42 pagesMeasles FM S 05072013Suhazeli AbdullahNo ratings yet