Download as docx, pdf, or txt
You might also like
- Amosup Member PrivilegesDocument64 pagesAmosup Member PrivilegesAMOSUPWeb80% (56)
- Medical Examination For Players Above Age of 12Document16 pagesMedical Examination For Players Above Age of 12Fakhrur Al IzzaNo ratings yet
- FANCAS AssessmentDocument19 pagesFANCAS AssessmentNelly Q. NisaNo ratings yet
- Knee Surgery: The Essential Guide to Total Knee RecoveryFrom EverandKnee Surgery: The Essential Guide to Total Knee RecoveryRating: 5 out of 5 stars5/5 (1)
- Blood Gas Analysis Ppt-3Document32 pagesBlood Gas Analysis Ppt-3Kresna Dharma SuryanaNo ratings yet
- Amputee CaseDocument33 pagesAmputee CaseIka Ayu ParamitaNo ratings yet
- Pre-Competition Medical Assessment ReportDocument23 pagesPre-Competition Medical Assessment ReportIati Raymond ChishiriNo ratings yet
- Impengement SyndromeDocument39 pagesImpengement Syndromewahyu_sitaNo ratings yet
- Case Report: Rehabilitation Program in A Patient With Congenital Dysplasia and Subluxation of The HipDocument26 pagesCase Report: Rehabilitation Program in A Patient With Congenital Dysplasia and Subluxation of The HipNatalia LoredanaNo ratings yet
- Muscle Origin and InsertionDocument3 pagesMuscle Origin and Insertionelengenesse_ajmNo ratings yet
- Short Case II: Jufri Febrianto, MDDocument16 pagesShort Case II: Jufri Febrianto, MDsingle_ladyNo ratings yet
- 1.20 (Surgery) Orthopedics Sports - PediatricsDocument8 pages1.20 (Surgery) Orthopedics Sports - PediatricsLeo Mari Go LimNo ratings yet
- Fifa Pcma FormDocument15 pagesFifa Pcma Formyousra AhmedNo ratings yet
- Brachial Plexus Palsy: RiasfDocument42 pagesBrachial Plexus Palsy: RiasfRiaFernandesNo ratings yet
- Schuster AthleticPelvisDocument26 pagesSchuster AthleticPelvisTheScribbl3rNo ratings yet
- Case Report Brachial Plexus Injury Post Ganglionic C5-C6Document25 pagesCase Report Brachial Plexus Injury Post Ganglionic C5-C6Anisa AnisatusholihahNo ratings yet
- Case Report Rehabilitation Program in A Patient With Left Intertrochanteric Femoral FractureDocument26 pagesCase Report Rehabilitation Program in A Patient With Left Intertrochanteric Femoral FractureNatalia LoredanaNo ratings yet
- Case Fraktur FinishDocument12 pagesCase Fraktur FinishNovaria Puspita SamudraNo ratings yet
- MR ILA Ankylosing Spondylitis DR EN 020424Document42 pagesMR ILA Ankylosing Spondylitis DR EN 020424damargilangNo ratings yet
- 1.18 (Surgery) General Orthopedics, Open Fractures, Compartment SyndromeDocument5 pages1.18 (Surgery) General Orthopedics, Open Fractures, Compartment SyndromeLeo Mari Go Lim100% (1)
- Carpal Tunnel Syndrome: by A. A. Sagung Mas CahyandariDocument37 pagesCarpal Tunnel Syndrome: by A. A. Sagung Mas CahyandariAnang FajarNo ratings yet
- Case Report Rehabilitation Program in A Patient With A Displaced Femoral Neck FractureDocument26 pagesCase Report Rehabilitation Program in A Patient With A Displaced Femoral Neck FractureNatalia LoredanaNo ratings yet
- Case Report Rehabilitation Program in A Patient With Femoral Neck FractureDocument26 pagesCase Report Rehabilitation Program in A Patient With Femoral Neck FractureNatalia LoredanaNo ratings yet
- Nueva Ecija University of Science and Technology College of Nursing Patient Care RecordDocument16 pagesNueva Ecija University of Science and Technology College of Nursing Patient Care RecordLEENLARALANCENo ratings yet
- Brachial Plexus Injury-26-10-23 - 112203Document29 pagesBrachial Plexus Injury-26-10-23 - 112203Barath Kumar SinghNo ratings yet
- Evaluation of The Patient With Hip PainDocument12 pagesEvaluation of The Patient With Hip PainDea LeeteukNo ratings yet
- Philippine Orthopedic Center Lecture NotesDocument7 pagesPhilippine Orthopedic Center Lecture Notesxteovisio100% (2)
- Acromioplasty Rehab ProtocolDocument3 pagesAcromioplasty Rehab ProtocolJay RammaNo ratings yet
- Lateral Epicondylitis PresentationDocument16 pagesLateral Epicondylitis Presentationapi-317395769No ratings yet
- SCI RehabilitationDocument15 pagesSCI RehabilitationSubrata BorahNo ratings yet
- Bicipital TenditisDocument5 pagesBicipital TenditisKrystal Shine BalabboNo ratings yet
- ContractureDocument45 pagesContracturePramitha Yustia100% (1)
- BAAPSDocument147 pagesBAAPSGaurav Patodia100% (1)
- Osteoarthritis Genu: Gutama Arya Pringga, DRDocument21 pagesOsteoarthritis Genu: Gutama Arya Pringga, DRvirginiaNo ratings yet
- Halaman PengesahanDocument16 pagesHalaman PengesahanEga NoristaNo ratings yet
- Case Report Case Report On The Clinical Results of A Combined Cellular Therapy For Chronic Spinal Cord Injured PatientsDocument5 pagesCase Report Case Report On The Clinical Results of A Combined Cellular Therapy For Chronic Spinal Cord Injured PatientsGustavo MovigliaNo ratings yet
- Lateral Epicondylitis (Tennis Elbow) : By:Ida Yuanita, MDDocument37 pagesLateral Epicondylitis (Tennis Elbow) : By:Ida Yuanita, MDAnang FajarNo ratings yet
- Initial Evaluation General InformationDocument7 pagesInitial Evaluation General InformationJoanna EdenNo ratings yet
- Orthopedi C Braces: NCM 116 RLEDocument44 pagesOrthopedi C Braces: NCM 116 RLEAlex Delos SantosNo ratings yet
- Closed Fracture of Midshaft Femur FracturesDocument33 pagesClosed Fracture of Midshaft Femur FracturesLana AdilaNo ratings yet
- Cervical Root SyndromeDocument48 pagesCervical Root SyndromeAnang FajarNo ratings yet
- Shoulder AnatomyDocument8 pagesShoulder AnatomyPraneeth KumarNo ratings yet
- 20 Questions - Orthopedic and Extremity InjuryDocument3 pages20 Questions - Orthopedic and Extremity InjurymichaelsophianNo ratings yet
- Lumbar SpineDocument1 pageLumbar Spineyosra adamNo ratings yet
- Medical Prefixes and SuffixesDocument12 pagesMedical Prefixes and SuffixesKrishnanunni KLNo ratings yet
- Case Report Rehabilitation Program in A Patient With Intertrochanteric Femoral FractureDocument26 pagesCase Report Rehabilitation Program in A Patient With Intertrochanteric Femoral FractureNatalia LoredanaNo ratings yet
- Glenohumeral Internal Rotation Deficit Rehab: Timmons Office: (713) 441-3560 Baytown Office: (832) 556-0880Document8 pagesGlenohumeral Internal Rotation Deficit Rehab: Timmons Office: (713) 441-3560 Baytown Office: (832) 556-0880mortadela silvaNo ratings yet
- Case Report Rehabilitation Program in A Patient With Bilateral Arthroplasty For Hip OsteoarthritisDocument26 pagesCase Report Rehabilitation Program in A Patient With Bilateral Arthroplasty For Hip OsteoarthritisNatalia LoredanaNo ratings yet
- Case Synopsis: Past HistoryDocument5 pagesCase Synopsis: Past Historyjayen_98No ratings yet
- 2010 March 24thDocument4 pages2010 March 24thTom WuNo ratings yet
- NCP For FractureDocument2 pagesNCP For FractureArnie Jude Carido100% (1)
- Fifa P - C M A (PCMA) : RE Ompetition Edical SsessmentDocument17 pagesFifa P - C M A (PCMA) : RE Ompetition Edical SsessmentMuhammad AdhaNo ratings yet
- (Download PDF) Shoulder Arthroplasty The Shoulder Club Guide Gazi Huri Online Ebook All Chapter PDFDocument42 pages(Download PDF) Shoulder Arthroplasty The Shoulder Club Guide Gazi Huri Online Ebook All Chapter PDFnancy.randolph444100% (12)
- Close Right Arm Fracture: Our Lady of Fatima University College of NursingDocument12 pagesClose Right Arm Fracture: Our Lady of Fatima University College of NursingBrylle Capili100% (1)
- Antenatal Case SheetDocument4 pagesAntenatal Case SheetRichard SnellNo ratings yet
- Lower Extremity Amputation #8Document7 pagesLower Extremity Amputation #8Mary StrangeNo ratings yet
- SC2 - TAZ - Adolescent Idiopathic ScoliosisDocument45 pagesSC2 - TAZ - Adolescent Idiopathic ScoliosisdamargilangNo ratings yet
- Spinal Stenosis - Johns Hopkins MedicineDocument3 pagesSpinal Stenosis - Johns Hopkins MedicinechhavishNo ratings yet
- Case Analysis - FractureDocument7 pagesCase Analysis - FractureMichelle Teodoro100% (1)
- Shoulder Arthroplasty: The Shoulder Club GuideFrom EverandShoulder Arthroplasty: The Shoulder Club GuideGazi HuriNo ratings yet
- Correct Your Pelvis and Heal your Back-Pain: The Self-Help Manual for Alleviating Back-Pain and other Musculo-Skeletal Aches and PainsFrom EverandCorrect Your Pelvis and Heal your Back-Pain: The Self-Help Manual for Alleviating Back-Pain and other Musculo-Skeletal Aches and PainsNo ratings yet
- 3 Ecce DerivativesDocument4 pages3 Ecce DerivativesGabriela MccawleyNo ratings yet
- Laparoscopic Repair of Large Type III Hiatal Hernia: Objective Followup Reveals High Recurrence RateDocument8 pagesLaparoscopic Repair of Large Type III Hiatal Hernia: Objective Followup Reveals High Recurrence RateAtulOsaveNo ratings yet
- FNCPDocument3 pagesFNCPDjan Kurvie ValencerinaNo ratings yet
- Lab Activity #1Document5 pagesLab Activity #1Meg Angela Cirunay-Decena0% (1)
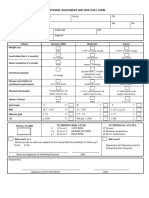
- 4 - Nutritional Assessment and Risk LevelDocument1 page4 - Nutritional Assessment and Risk LevelBok MatthewNo ratings yet
- Community Service ProjectDocument13 pagesCommunity Service ProjectvaibhavNo ratings yet
- DgdbuiDocument5 pagesDgdbuiAvinash Kumar SinghNo ratings yet
- Edl CHC 2016Document3 pagesEdl CHC 2016Prabir Kumar ChatterjeeNo ratings yet
- Entry Level Nurse Resume Sample - Windsor OriginalDocument2 pagesEntry Level Nurse Resume Sample - Windsor OriginalRatrika SariNo ratings yet
- Chapter 1-3Document41 pagesChapter 1-3Alerick Velasco100% (6)
- En Atex BrochureDocument12 pagesEn Atex BrochureAntony MylvaganamNo ratings yet
- Challenging Clinical Scenarios of The BreastDocument62 pagesChallenging Clinical Scenarios of The BreastMuhammad HassanNo ratings yet
- 5.11 Normal Ecg, Chamber Enlargements, Ischemia, Infarcts: TH THDocument6 pages5.11 Normal Ecg, Chamber Enlargements, Ischemia, Infarcts: TH THRomeo AragonNo ratings yet
- 403ACIjournalsDocument10 pages403ACIjournalsNguyen Van QuyenNo ratings yet
- Failure To ThriveDocument4 pagesFailure To ThriveShane PangilinanNo ratings yet
- Abdul Halim, Abu Sayeed Md. Abdullah, Fazlur Rahman, Animesh BiswasDocument11 pagesAbdul Halim, Abu Sayeed Md. Abdullah, Fazlur Rahman, Animesh BiswasNoraNo ratings yet
- Parents OrientationDocument2 pagesParents OrientationDonna Marie Paz CasipitNo ratings yet
- Serbia Cleanrooms Seminar 2Document31 pagesSerbia Cleanrooms Seminar 2Luis Gerardo Almanza LlanosNo ratings yet
- Ateneo de Zamboanga University: WaiverDocument1 pageAteneo de Zamboanga University: WaiverCATHERINE SIENNA ALTARNo ratings yet
- Risk Taking WorksheetDocument1 pageRisk Taking WorksheetTina EvansNo ratings yet
- Lesson Plan in CheerdanceDocument14 pagesLesson Plan in CheerdanceVeejayjay marquez100% (1)
- Facial Flow Final PDFDocument6 pagesFacial Flow Final PDFsamir caceresNo ratings yet
- Controversies in Periodontogy. Rama. NikhatDocument121 pagesControversies in Periodontogy. Rama. NikhatDpartment of Periodontology100% (1)
- Karpaga Vinayaga College of NursingDocument11 pagesKarpaga Vinayaga College of NursingPreeti ChouhanNo ratings yet
- Bright Kids - 06092016Document12 pagesBright Kids - 06092016Times MediaNo ratings yet
- Editor 'S Desk: As I Com Pile This Edition With An Inspiring WorkDocument7 pagesEditor 'S Desk: As I Com Pile This Edition With An Inspiring Workbotta bhavnaNo ratings yet
- Times 2003Document222 pagesTimes 2003tazman123No ratings yet
- Week 2 - Whats Eating Gilbert GrapeDocument2 pagesWeek 2 - Whats Eating Gilbert GrapeGabriella ConcepciónNo ratings yet
- Head InjuryDocument61 pagesHead InjuryRicky Cornelius TariganNo ratings yet