Download as pdf or txt
You might also like
- A Guide To The Examination of Horses (The Blue Book) - 0Document56 pagesA Guide To The Examination of Horses (The Blue Book) - 0sangeetsamrat100% (1)
- Managing Congenitally Missing Lateral Incisors. Part III: Single-Tooth ImplantsDocument9 pagesManaging Congenitally Missing Lateral Incisors. Part III: Single-Tooth ImplantsSalma RafiqNo ratings yet
- 7-Differences Between Primary and Permanent TeethDocument4 pages7-Differences Between Primary and Permanent TeethAhmed AbdNo ratings yet
- Orth Update 2021 14 8-12Document5 pagesOrth Update 2021 14 8-12sunk86100% (1)
- ActivatorDocument7 pagesActivatorMeenu D GrtNo ratings yet
- Orthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFrom EverandOrthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFederico BrugnamiNo ratings yet
- Oral Habits and Its Relationship To Malocclusion A Review.20141212083000Document4 pagesOral Habits and Its Relationship To Malocclusion A Review.20141212083000Stacia AnastashaNo ratings yet
- Terapia MiofuncionalDocument10 pagesTerapia MiofuncionalvivianaNo ratings yet
- A Modified Bluegrass Appliance For Interception of Tongue Thrust Habit - A Clinical InnovatiDocument3 pagesA Modified Bluegrass Appliance For Interception of Tongue Thrust Habit - A Clinical InnovatiAdvanced Research PublicationsNo ratings yet
- Journal of Musculoskeletal Disorders and Treatment JMDT 2 022Document6 pagesJournal of Musculoskeletal Disorders and Treatment JMDT 2 022mulya sfNo ratings yet
- Development of Occlusion: Gum Pads StageDocument5 pagesDevelopment of Occlusion: Gum Pads StageSaid SaidNo ratings yet
- Evaluation of Tongue Force Using Piezoelectric Sensor in Tongue Thrusting PatientsDocument4 pagesEvaluation of Tongue Force Using Piezoelectric Sensor in Tongue Thrusting PatientsIJAR JOURNALNo ratings yet
- Gumy SmileDocument8 pagesGumy Smiledr. gusfarizNo ratings yet
- PREPROSTHETIC SURGERY - RamonDocument49 pagesPREPROSTHETIC SURGERY - Ramonjamaica faith ramonNo ratings yet
- OcclusionDocument26 pagesOcclusionAbdelrahman Galal100% (2)
- Understanding The Basis of Space Closure in Orthodontics For A More Efficient Orthodontic TreatmentDocument12 pagesUnderstanding The Basis of Space Closure in Orthodontics For A More Efficient Orthodontic TreatmentGerardo QuinteroNo ratings yet
- Extrinsic and Intrinsic Factors in The Etiology of MalocclusionDocument7 pagesExtrinsic and Intrinsic Factors in The Etiology of MalocclusionNavroop KaurNo ratings yet
- Appliance Catalogue: Orthodontic S Without Brac EsDocument8 pagesAppliance Catalogue: Orthodontic S Without Brac EsIzat IzatNo ratings yet
- Altered Active and Passive Eruption A Modified ClassificationDocument7 pagesAltered Active and Passive Eruption A Modified ClassificationMara CondorNo ratings yet
- Congenitally Missing Lateral IncisorDocument17 pagesCongenitally Missing Lateral IncisorAvneet MalikNo ratings yet
- Invasive Cervical Résorption: An Analysis of Potential Predisposing FactorsDocument14 pagesInvasive Cervical Résorption: An Analysis of Potential Predisposing FactorsNitin LalwaniNo ratings yet
- Complete Denture Prosthodontics in Children With Ectodermal DysplasiaDocument29 pagesComplete Denture Prosthodontics in Children With Ectodermal DysplasiaAmit BhargavNo ratings yet
- 11 - Facts and Myths Regarding The Maxillary Midline Frenum and Its Treatment A Systematic Review of The LiteratureDocument11 pages11 - Facts and Myths Regarding The Maxillary Midline Frenum and Its Treatment A Systematic Review of The Literaturekochikaghochi100% (1)
- Molares InclinadosDocument13 pagesMolares Inclinadosmaria jose peña rojas100% (1)
- Space Regainers in Pediatric DentistryDocument6 pagesSpace Regainers in Pediatric DentistryDiba Eka DiputriNo ratings yet
- Functional Occlusion and The Mounting of The CastsDocument88 pagesFunctional Occlusion and The Mounting of The CastsAina SalsaNo ratings yet
- Early Childhood CariesDocument26 pagesEarly Childhood Cariesapi-485081343No ratings yet
- Crowding 180601115625 PDFDocument109 pagesCrowding 180601115625 PDFVishal SharmaNo ratings yet
- Goals of Orthodontic TreatmentDocument14 pagesGoals of Orthodontic TreatmentemanNo ratings yet
- Occlusal AnalysisDocument14 pagesOcclusal AnalysisDavid DongNo ratings yet
- A Review of Root Resorption in Orthodontics PDFDocument5 pagesA Review of Root Resorption in Orthodontics PDFRahulLife'sNo ratings yet
- Lec.9 Ortho. MovementDocument10 pagesLec.9 Ortho. MovementSaid SaidNo ratings yet
- Management of Impacted Maxillary Canines Using Mandibular AnchorageDocument4 pagesManagement of Impacted Maxillary Canines Using Mandibular Anchoragedrsankhya100% (1)
- Management of Developing DentitionDocument51 pagesManagement of Developing Dentitionahmed alshaariNo ratings yet
- Importance of 1st Permanent MolarDocument28 pagesImportance of 1st Permanent MolarAdyasha SahuNo ratings yet
- Development of Dentition and Occlusion: Sujina.SDocument214 pagesDevelopment of Dentition and Occlusion: Sujina.SsathyaNo ratings yet
- Orthodontics 1. Clinical ExaminationDocument8 pagesOrthodontics 1. Clinical Examinationmonica896No ratings yet
- Epithelial-Mesenchymal Signalling Regulating Tooth MorphogenesisDocument2 pagesEpithelial-Mesenchymal Signalling Regulating Tooth MorphogenesisalifNo ratings yet
- Congenitally Missing Maxillary Lateral IncisorsDocument56 pagesCongenitally Missing Maxillary Lateral Incisorsdrsankhya100% (1)
- Development of Occlusion (Seminar 1)Document47 pagesDevelopment of Occlusion (Seminar 1)Isha GargNo ratings yet
- Management of Open BiteDocument25 pagesManagement of Open BiteMoola Bharath ReddyNo ratings yet
- Zachrisson Et Al 2011, Canine Substitution PDFDocument6 pagesZachrisson Et Al 2011, Canine Substitution PDFDiana BobNo ratings yet
- Introduction To Dental Anatomy: Learning Objec TivesDocument12 pagesIntroduction To Dental Anatomy: Learning Objec Tivesbalkiz mahamedNo ratings yet
- 3.factors and Techniques Influencing Peri-Implant Papillae - PDFDocument12 pages3.factors and Techniques Influencing Peri-Implant Papillae - PDFMargarita María Blanco LópezNo ratings yet
- Gummy Smile and Optimization of Dentofacial Esthetics: Muhamad Abu-Hussein Nezar Watted Azzaldeen AbdulganiDocument5 pagesGummy Smile and Optimization of Dentofacial Esthetics: Muhamad Abu-Hussein Nezar Watted Azzaldeen AbdulganiIOSRjournalNo ratings yet
- Kinzer Kokich-Managing Congenitally Missing Lateral Incisors Part I Canine Substitution PDFDocument5 pagesKinzer Kokich-Managing Congenitally Missing Lateral Incisors Part I Canine Substitution PDFAdrian Silva SantosNo ratings yet
- Manual of Dental Practice 2014 Estonia: Council of European DentistsDocument10 pagesManual of Dental Practice 2014 Estonia: Council of European DentistsMohd GhausNo ratings yet
- Mandibular Incisor Extraction TherapyDocument10 pagesMandibular Incisor Extraction TherapyLeonardo LamimNo ratings yet
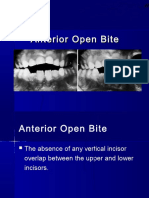
- Anterior Open BiteDocument34 pagesAnterior Open BiteAbdullah100% (1)
- Burstone PDFDocument23 pagesBurstone PDFJulio Ugás ZapataNo ratings yet
- Thumb SuckingDocument3 pagesThumb SuckingBasant karn50% (2)
- BroadbentDocument57 pagesBroadbentortodoncia 2018100% (1)
- Cephalometric SentDocument17 pagesCephalometric SentMuhammad NiyalishNo ratings yet
- Extraoral Orthopaedic AppliancesDocument59 pagesExtraoral Orthopaedic AppliancesAmatullahsadiyaNo ratings yet
- Transverse Dimension Andlong-Term Stability Robert L Vanarsdall JRDocument10 pagesTransverse Dimension Andlong-Term Stability Robert L Vanarsdall JRMa Lyn GabayeronNo ratings yet
- Impacted Maxillary Canines-A Review. - American Journal of Orthodontics and Dentofacial Orthopedics, 101-159, 1992 PDFDocument13 pagesImpacted Maxillary Canines-A Review. - American Journal of Orthodontics and Dentofacial Orthopedics, 101-159, 1992 PDFPia ContrerasNo ratings yet
- Bhanu Impaction Seminar FinalDocument138 pagesBhanu Impaction Seminar FinalBhanu PraseedhaNo ratings yet
- Smile Analysis: A Review Part IIDocument4 pagesSmile Analysis: A Review Part IIGustavoAndresGarciaNo ratings yet
- Journal Club1 / Orthodontic Courses by Indian Dental AcademyDocument19 pagesJournal Club1 / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Esthetic Considerations in Interdental Papilla PDFDocument11 pagesEsthetic Considerations in Interdental Papilla PDFXavier AltamiranoNo ratings yet
- Orthodontic Biomechanics: Treatment Of Complex Cases Using Clear AlignerFrom EverandOrthodontic Biomechanics: Treatment Of Complex Cases Using Clear AlignerNo ratings yet
- Borderline Cases in Orthodontics-A ReviewDocument6 pagesBorderline Cases in Orthodontics-A ReviewShatabdi A ChakravartyNo ratings yet
- Airway Focused Orthodontics: Invited SubmissionDocument6 pagesAirway Focused Orthodontics: Invited SubmissionShatabdi A ChakravartyNo ratings yet
- A Miniplate System For Improved Stability of Skeletal AnchorageDocument8 pagesA Miniplate System For Improved Stability of Skeletal AnchorageShatabdi A ChakravartyNo ratings yet
- Technique Clinic: Precise, Simultaneous Bracket and Miniscrew PlacementDocument2 pagesTechnique Clinic: Precise, Simultaneous Bracket and Miniscrew PlacementShatabdi A ChakravartyNo ratings yet
- A Patient-Classification System For Invisalign Cases: Doug Crosby, DDS, Ms Jessica LeeDocument5 pagesA Patient-Classification System For Invisalign Cases: Doug Crosby, DDS, Ms Jessica LeeShatabdi A ChakravartyNo ratings yet
- Krishnan 2006Document10 pagesKrishnan 2006Shatabdi A ChakravartyNo ratings yet
- Highly Crystalline MP-1 Hydroxylapatite Coating Part II: in Vivo Performance On Endosseous Root Implants in DogsDocument11 pagesHighly Crystalline MP-1 Hydroxylapatite Coating Part II: in Vivo Performance On Endosseous Root Implants in DogsShatabdi A ChakravartyNo ratings yet
- Unilateral ExtractionDocument10 pagesUnilateral ExtractionShatabdi A ChakravartyNo ratings yet
- Roth Vs MBTDocument2 pagesRoth Vs MBTShatabdi A ChakravartyNo ratings yet
- Brouwer 1973Document21 pagesBrouwer 1973Shatabdi A ChakravartyNo ratings yet
- MCQs On AutoimmunityDocument8 pagesMCQs On AutoimmunityShatabdi A Chakravarty100% (1)
- Genentech Internship Journal E-PortfolioDocument5 pagesGenentech Internship Journal E-Portfolioapi-317145308No ratings yet
- Joint DislocationDocument7 pagesJoint DislocationTeka KamNo ratings yet
- The New England Journal of Medicine Case Records of The Massachusetts General Hospital " Continuing To Learn From The Patient "Document44 pagesThe New England Journal of Medicine Case Records of The Massachusetts General Hospital " Continuing To Learn From The Patient "Triple ANo ratings yet
- Global Ivermectin Adoption For COVIDDocument18 pagesGlobal Ivermectin Adoption For COVIDFilipos Constantin100% (1)
- Dermatofitosis 2011 1Document35 pagesDermatofitosis 2011 1Carmen Cajina Doña MamiNo ratings yet
- Cerebral Salt Wasting SyndromeDocument6 pagesCerebral Salt Wasting SyndromeBrian BaileyNo ratings yet
- 656 659 PDFDocument4 pages656 659 PDFEloísa VásquezNo ratings yet
- Do Not Resuscitate (DNR) ResearchDocument7 pagesDo Not Resuscitate (DNR) ResearchOmar SalehNo ratings yet
- Antigens ClassDocument61 pagesAntigens ClassKoushali BanerjeeNo ratings yet
- Diatron (Samsung LABGEO) 2020 Abacus 5 Abacus 380Document5 pagesDiatron (Samsung LABGEO) 2020 Abacus 5 Abacus 380Mozfar IdreesNo ratings yet
- 31 de AgostoDocument23 pages31 de AgostoDavid CoelloNo ratings yet
- New PDF For PharmacologyDocument236 pagesNew PDF For PharmacologyDIPENDRA KUMAR KUSHAWAHA100% (1)
- Indian Ethnobotany: A Study On Past, Present and Future ProspectDocument11 pagesIndian Ethnobotany: A Study On Past, Present and Future ProspectTanika SinghNo ratings yet
- The Michael Jackson Autopsy Insights Provided by A Forensic Anesthesiologist 2157 7145.1000138 PDFDocument8 pagesThe Michael Jackson Autopsy Insights Provided by A Forensic Anesthesiologist 2157 7145.1000138 PDFJimmy R. JosephNo ratings yet
- Who S Who? Write The Names Under The Pictures.: Asignatura Objetivo de AprendizajeDocument5 pagesWho S Who? Write The Names Under The Pictures.: Asignatura Objetivo de AprendizajeMarisol VB100% (1)
- Surgical Cs Case Study - BangDocument25 pagesSurgical Cs Case Study - BangClyde R.OrtegaNo ratings yet
- 29 - Unusual - Extraoral SinusDocument29 pages29 - Unusual - Extraoral SinussonalyadavchinuNo ratings yet
- Types of Paraneoplastic Syndromes: 1 (Small Cell Carcinoma of LungDocument21 pagesTypes of Paraneoplastic Syndromes: 1 (Small Cell Carcinoma of LungSawsan Z. JwaiedNo ratings yet
- Cultural Competence Importance in HealthcareDocument20 pagesCultural Competence Importance in Healthcaresaharconsulting100% (6)
- Phytochemical Ingredients and Pharmacological Potential ofDocument17 pagesPhytochemical Ingredients and Pharmacological Potential ofzainab jehangirNo ratings yet
- Abdominal Stab WoundDocument5 pagesAbdominal Stab WoundHemingmingNo ratings yet
- Bear's Loose Tooth Lesson PlanDocument6 pagesBear's Loose Tooth Lesson PlanHeather Myers AntunezNo ratings yet
- Jensen - Outlining Anes Oral BoardsDocument9 pagesJensen - Outlining Anes Oral BoardsAriana AnugerahNo ratings yet
- ACETricepsStudy PDFDocument3 pagesACETricepsStudy PDFAlina PopescuNo ratings yet
- Chapter 15 Innate ImmunityDocument38 pagesChapter 15 Innate Immunityapi-270625839No ratings yet
- Trauma Saraf SpinalDocument41 pagesTrauma Saraf SpinalFatahillah NazarNo ratings yet
- Platelet Counting Fordirect Indirect MethodDocument30 pagesPlatelet Counting Fordirect Indirect MethodShana Flame Haze100% (2)
- Soal Cpns - BHSINGDocument25 pagesSoal Cpns - BHSINGSeesams AliNo ratings yet