Download as pdf or txt
You might also like
- Benign Breast Lesion 151120222Document81 pagesBenign Breast Lesion 151120222pannawat trerattanavongNo ratings yet
- The Pathology of Breast 14Document76 pagesThe Pathology of Breast 14Abu ZidaneNo ratings yet
- PATHOPHYSIOLOGY of NeurocysticercosisDocument6 pagesPATHOPHYSIOLOGY of Neurocysticercosisteddydeclines14100% (3)
- Pathology B - Breasts (Dy-Quiangco, 2016)Document10 pagesPathology B - Breasts (Dy-Quiangco, 2016)sahaniNo ratings yet
- BreastDocument8 pagesBreastNada MuchNo ratings yet
- Breast Pathology 1Document20 pagesBreast Pathology 1Awais IrshadNo ratings yet
- Pathology 5.05a CervixDocument6 pagesPathology 5.05a CervixDranreb Berylle MasangkayNo ratings yet
- Patho5-2 - Breast (Dr. Yanez)Document10 pagesPatho5-2 - Breast (Dr. Yanez)Miguel Cuevas DolotNo ratings yet
- Introduction To Breast DiseasesDocument10 pagesIntroduction To Breast DiseasessintayehuNo ratings yet
- ND THDocument14 pagesND THClint MorrisonNo ratings yet
- Pre-Invasive Lesions of The Cervix 2020Document58 pagesPre-Invasive Lesions of The Cervix 2020Jeno Luis J. ACUBNo ratings yet
- Focus Data Action Response SDocument5 pagesFocus Data Action Response SMeynard AndresNo ratings yet
- Benign Lesion Mimicking Malignant Breast LesionDocument82 pagesBenign Lesion Mimicking Malignant Breast Lesionachmad rizkiNo ratings yet
- Benign Disorders and Diseases of The BreastDocument45 pagesBenign Disorders and Diseases of The BreastzubairNo ratings yet
- Breast Sonography: Presented by DR Livinus - Chibuzo AbonyiDocument28 pagesBreast Sonography: Presented by DR Livinus - Chibuzo AbonyiKEN KIZITONo ratings yet
- Cervical ErosionDocument19 pagesCervical ErosionYogesh ValaNo ratings yet
- Chaiyarat Parames 2200084. 08.03.2023Document7 pagesChaiyarat Parames 2200084. 08.03.2023parames03041512No ratings yet
- 8,9-Breast CancerDocument24 pages8,9-Breast CancerAlmassri EslamNo ratings yet
- Affinity of Homoeopathic Drugs in Cases of FibroadenomaDocument5 pagesAffinity of Homoeopathic Drugs in Cases of FibroadenomaMohini GhãÑghàsNo ratings yet
- Learning Unit 7 - Benign Reactive Changes Part 2Document39 pagesLearning Unit 7 - Benign Reactive Changes Part 2Marelize ErasmusNo ratings yet
- Breast NewDocument72 pagesBreast NewDyn AdrianiNo ratings yet
- Breast Pathology 2018 PDFDocument12 pagesBreast Pathology 2018 PDFzaidNo ratings yet
- Lab Act Breast Mei 2022Document38 pagesLab Act Breast Mei 2022Cynthia AristaNo ratings yet
- Breast Surgery 1Document17 pagesBreast Surgery 1mariamNo ratings yet
- Cysts of The Oral CavityDocument11 pagesCysts of The Oral CavityGhada YaakoubNo ratings yet
- Day 1Document21 pagesDay 1Ahmed DorghamNo ratings yet
- Benign Tumor of The CervixDocument47 pagesBenign Tumor of The CervixjerrydanfordfxNo ratings yet
- Cervical Changes18 4Document75 pagesCervical Changes18 4Shaimaa DawaNo ratings yet
- Benign Gynecological LesionsDocument9 pagesBenign Gynecological LesionsLanceNo ratings yet
- Cervical Cancer - Pathology & CytologyDocument12 pagesCervical Cancer - Pathology & CytologyRekha GadgilNo ratings yet
- Benign & Malignant Breast Lesions Presented By: Omar Al. Ma'aita Mais Al - Shboul 6 Year, Surgery Course, J.U.S.TDocument87 pagesBenign & Malignant Breast Lesions Presented By: Omar Al. Ma'aita Mais Al - Shboul 6 Year, Surgery Course, J.U.S.TRussia Al Shboul100% (1)
- Patho OthaplmoDocument3 pagesPatho OthaplmoSushanta BhattaraiNo ratings yet
- Eqb - Breast: Le DischargeDocument22 pagesEqb - Breast: Le DischargeSagarRathodNo ratings yet
- Diseases of Female Reproductive SystemDocument13 pagesDiseases of Female Reproductive SystemSalon LamichhaneNo ratings yet
- Benign Disorders and Breast DXDocument19 pagesBenign Disorders and Breast DXkurniafniatiNo ratings yet
- Nabothian CystsDocument24 pagesNabothian CystsVirna SeptianaNo ratings yet
- Ovarian Cyst Topic ListDocument29 pagesOvarian Cyst Topic ListMichelle Defandi ChanNo ratings yet
- P2 Breast Pathology (Patho Surg) PDFDocument120 pagesP2 Breast Pathology (Patho Surg) PDFThakoon TtsNo ratings yet
- Management of Cystic Conditions+++Document14 pagesManagement of Cystic Conditions+++Fernando Peralta PalmezanoNo ratings yet
- Cytology 2Document30 pagesCytology 2okonkwojohnchuks1No ratings yet
- Benign Ovarian MassDocument39 pagesBenign Ovarian MassVidhi Chaudhary100% (1)
- Esophagus TumorsDocument5 pagesEsophagus TumorsblablalbablablablaNo ratings yet
- Clin TG Abnormalities of The Placenta & CordDocument13 pagesClin TG Abnormalities of The Placenta & CordTami Selvi100% (2)
- UNIT 15 Epith TumorsDocument25 pagesUNIT 15 Epith TumorsInes AlarfajNo ratings yet
- Ilovepdf MergedDocument119 pagesIlovepdf Mergedkushal100% (1)
- Salivary Gland Tumors2Document12 pagesSalivary Gland Tumors2Jose Siritt100% (1)
- Chapter 23 BreastDocument7 pagesChapter 23 BreastIsfahan MasulotNo ratings yet
- PBL CASE 2 Module 13 Reproductive SystemDocument25 pagesPBL CASE 2 Module 13 Reproductive SystemkaraenNo ratings yet
- Benign Conditions of The BreastDocument9 pagesBenign Conditions of The BreastSalim Mwiti NabeaNo ratings yet
- Benign Breast Disorders: Diani KartiniDocument27 pagesBenign Breast Disorders: Diani KartiniAngga ArioNo ratings yet
- Patho by DR - Elnemr (RPR)Document10 pagesPatho by DR - Elnemr (RPR)mrhazemahmed00No ratings yet
- 3.diseases of The BreastDocument87 pages3.diseases of The Breastأسود / BlackNo ratings yet
- Breast Pathology ReviewDocument45 pagesBreast Pathology ReviewNunu MirNo ratings yet
- Breast Patho LectDocument121 pagesBreast Patho LectRose AnnNo ratings yet
- Abnormal ImplantationDocument3 pagesAbnormal ImplantationMuhammet Fatih CantepeNo ratings yet
- at NeoplasmDocument50 pagesat NeoplasmNazmus SakibNo ratings yet
- Post Partum HemorrhageDocument9 pagesPost Partum HemorrhageghsNo ratings yet
- Cysts of The Jaw and Soft Tissues: A-Odontogenic Keratocyst. B - Dentigerous CystDocument15 pagesCysts of The Jaw and Soft Tissues: A-Odontogenic Keratocyst. B - Dentigerous CystruchikaNo ratings yet
- EndometriosisDocument10 pagesEndometriosisSivaram Shanmugha VilasNo ratings yet
- Tolerance: Chapter 20 - Regulation of Adaptive ImmunityDocument4 pagesTolerance: Chapter 20 - Regulation of Adaptive ImmunityZoe Alea MartinezNo ratings yet
- Lymphatic System and Immunity: Student Learning OutcomesDocument8 pagesLymphatic System and Immunity: Student Learning Outcomeslily1liang-1No ratings yet
- Vet Radiology Ultrasound - 2022 - SeilerDocument14 pagesVet Radiology Ultrasound - 2022 - SeilerWilver CanizalesNo ratings yet
- Cardiac Anatomy and Phvsiologv A Review - Aorn800Document16 pagesCardiac Anatomy and Phvsiologv A Review - Aorn800Citra Ayu ApriliaNo ratings yet
- Case Report Klatskin TumorDocument5 pagesCase Report Klatskin TumorwadejackNo ratings yet
- Surgery by GiselleDocument15 pagesSurgery by GiselleTris100% (1)
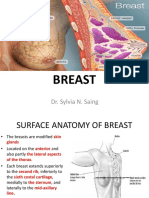
- Breast: Dr. Sylvia N. SaingDocument26 pagesBreast: Dr. Sylvia N. SaingRichard 151289100% (1)
- Endocrinology ProlactinomaDocument3 pagesEndocrinology ProlactinomasharrisanyaeNo ratings yet
- Necropsy Guide For Dogs Cats and Small Mammals - 2016 - McDonough - Front MatterDocument17 pagesNecropsy Guide For Dogs Cats and Small Mammals - 2016 - McDonough - Front Matternabal22No ratings yet
- Study Guide 1 Assessment of Digestive and Gastrointestinal Function and Treatment ModalitiesDocument10 pagesStudy Guide 1 Assessment of Digestive and Gastrointestinal Function and Treatment ModalitiesKc Cabanilla LizardoNo ratings yet
- Human Pelvis, MaleDocument24 pagesHuman Pelvis, MaleScience HouseNo ratings yet
- Topic - Characters and Affinities of DipnoiDocument11 pagesTopic - Characters and Affinities of Dipnoihj100% (1)
- محاضرات أنسجة 2017Document20 pagesمحاضرات أنسجة 2017Salam H Alhelali100% (2)
- Broncho-Pulmonary SegmentsDocument29 pagesBroncho-Pulmonary SegmentsArbin PanjaNo ratings yet
- Nervous SystemDocument3 pagesNervous SystemMary Rose Ponte FernandezNo ratings yet
- File Urecol DIANADocument14 pagesFile Urecol DIANAdiana lestariNo ratings yet
- MODULE 5 2ND QUARTERT Science 6 EDITDocument8 pagesMODULE 5 2ND QUARTERT Science 6 EDITEmie PonceNo ratings yet
- Ataxic Neurodegenerative Satiety Deficiency Syndrome: According To Dr. Steven C. SchlozmanDocument4 pagesAtaxic Neurodegenerative Satiety Deficiency Syndrome: According To Dr. Steven C. SchlozmanGabriel Martin100% (1)
- Histology of The Adrenal GlandsDocument1 pageHistology of The Adrenal GlandsSabrina NodariNo ratings yet
- Urinary System AssessmentDocument43 pagesUrinary System AssessmentGiri Siva100% (2)
- Study Material Class XDocument14 pagesStudy Material Class XsaleemNo ratings yet
- 3 4 PERTEMUAN 3 - 4 Far RangkiDocument35 pages3 4 PERTEMUAN 3 - 4 Far RangkiNoerhayatea SibaraniNo ratings yet
- Cerebral Salt Wasting Syndrome - StatPearls - NCBI BookshelfDocument4 pagesCerebral Salt Wasting Syndrome - StatPearls - NCBI BookshelfOnggo WiliyantoNo ratings yet
- T and B CellsDocument13 pagesT and B CellsFaisal Jamshed100% (1)
- Extracted Pages From 8. AcumedicoDocument1 pageExtracted Pages From 8. AcumedicodishkuNo ratings yet
- Ecg MonitoringDocument26 pagesEcg Monitoringclaire yowsNo ratings yet
- Professional Ethics and Responsibilities: Mitral ValveDocument9 pagesProfessional Ethics and Responsibilities: Mitral ValveMary LouNo ratings yet
- Grade3 Sense OrgansDocument28 pagesGrade3 Sense OrgansjindeylNo ratings yet
- Infant FeedingDocument26 pagesInfant Feedingabdelrahmanmoselhy122No ratings yet
- Lymphoid OrgansDocument4 pagesLymphoid OrgansJadys Merill DiezNo ratings yet