Download as pdf or txt
You might also like
- Adaptive School - StrategiesDocument301 pagesAdaptive School - StrategiesAngel GiranoNo ratings yet
- Itunes Gifted Card Format-1Document1 pageItunes Gifted Card Format-1Mr Naijatim89% (282)
- BPR at Nike: Submitted By:-Krishan Pal B.E (Chem) Int MBA, 5 Year CM15216Document8 pagesBPR at Nike: Submitted By:-Krishan Pal B.E (Chem) Int MBA, 5 Year CM15216krishan pal100% (1)
- How Can The Law Be Used As An Instrument For Creating Social Change - IpleadersDocument13 pagesHow Can The Law Be Used As An Instrument For Creating Social Change - IpleadersLeelakrishna VemuruNo ratings yet
- The Perception of Anatomy Teaching Among UK Medical StudentsDocument4 pagesThe Perception of Anatomy Teaching Among UK Medical StudentsPaul AndreasNo ratings yet
- Bedside Teaching of Medical StudentsDocument2 pagesBedside Teaching of Medical StudentsRafi Ullah HaleemNo ratings yet
- Herzig Et At, 2012.Document6 pagesHerzig Et At, 2012.MarcelaPuentesNo ratings yet
- Death by AbleismDocument3 pagesDeath by AbleismtolliNo ratings yet
- 3 Jury S Martin Harris B 2020 Best Practices in Modified BariumDocument16 pages3 Jury S Martin Harris B 2020 Best Practices in Modified Bariumfranciscojavier.hernandez.eNo ratings yet
- The Importance of Anatomy in Health Professions.8Document3 pagesThe Importance of Anatomy in Health Professions.8Dr Dhiren Kumar PandaNo ratings yet
- Family Physicians' Experiences of Physical Examination: Martina Ann Kelly, Lisa Kathryn Freeman, Tim DornanDocument7 pagesFamily Physicians' Experiences of Physical Examination: Martina Ann Kelly, Lisa Kathryn Freeman, Tim DornanMahmoud AbouelsoudNo ratings yet
- Perceptions of Cadaveric Dissection in Anatomy Teaching: Original ArticleDocument4 pagesPerceptions of Cadaveric Dissection in Anatomy Teaching: Original ArticleDawit H. WoldeyesNo ratings yet
- Short Term and Long Term EffectsDocument9 pagesShort Term and Long Term EffectsmariapaulapmNo ratings yet
- The Rheumatology Physical Examination: Making Clinical Anatomy RelevantDocument7 pagesThe Rheumatology Physical Examination: Making Clinical Anatomy RelevantJoão GasparNo ratings yet
- Expert Evidence Criminal: Presenting ProceedingsDocument2 pagesExpert Evidence Criminal: Presenting ProceedingsLana NeparidzeNo ratings yet
- Health Professional For A New CenturyDocument36 pagesHealth Professional For A New CenturyjoaoNo ratings yet
- Jed120070 923 924Document2 pagesJed120070 923 924LyinglionNo ratings yet
- Pathogenesis and Treatment of Varicoceles: Controversy Still Surrounds Surgical TreatmentDocument2 pagesPathogenesis and Treatment of Varicoceles: Controversy Still Surrounds Surgical TreatmentFenny LiNo ratings yet
- PDF 13Document1 pagePDF 13Amina GoharyNo ratings yet
- Raise Standards For Preclinical Cancer ResearchDocument3 pagesRaise Standards For Preclinical Cancer ResearchMiguel CastroNo ratings yet
- Finding-the-Right-Balance-in-Lung-Nodule-EvaluatioDocument2 pagesFinding-the-Right-Balance-in-Lung-Nodule-Evaluatiosergio salazarNo ratings yet
- Congenital Muscular Torticollis: Bridging The Gap Between Research and Clinical PracticeDocument10 pagesCongenital Muscular Torticollis: Bridging The Gap Between Research and Clinical PracticeMuiz SaddozaiNo ratings yet
- Mbs Measurement Tool For Swallow Impairment-Mbsimp: Establishing A StandardDocument15 pagesMbs Measurement Tool For Swallow Impairment-Mbsimp: Establishing A StandardTaty MorenaNo ratings yet
- ScriptDocument13 pagesScript張水蛙No ratings yet
- Identifying Predictors of Ventral Hernia Recurrence Systematic Review and Meta-AnalysisDocument9 pagesIdentifying Predictors of Ventral Hernia Recurrence Systematic Review and Meta-Analysiss2mz66b26gNo ratings yet
- The FNIH Sarcopenia Project: Rationale, Study Description, Conference Recommendations, and Final EstimatesDocument12 pagesThe FNIH Sarcopenia Project: Rationale, Study Description, Conference Recommendations, and Final EstimatesCsenge JeszenszkyNo ratings yet
- Nejmp 1215594Document4 pagesNejmp 1215594Cj AlmazanNo ratings yet
- Biofilms and Chronic Infections: CommentariesDocument3 pagesBiofilms and Chronic Infections: CommentariesnissaNo ratings yet
- Causal Inference and Effects of Interventions From Observational Studies in Medical Journals JAMA 202Document9 pagesCausal Inference and Effects of Interventions From Observational Studies in Medical Journals JAMA 202Medicina InternaNo ratings yet
- The Importance of The Autopsy in Medicine: Perspectives of Pathology ColleaguesDocument9 pagesThe Importance of The Autopsy in Medicine: Perspectives of Pathology Colleaguesป๋ม ชอบลั่นล๊าNo ratings yet
- The Doctor's Oldest Tool: PerspectiveDocument3 pagesThe Doctor's Oldest Tool: PerspectivePierre PradelNo ratings yet
- (Panic) Laboratory (Parameter) : PolicyDocument1 page(Panic) Laboratory (Parameter) : Policymy accountNo ratings yet
- Genetic Dietetics - Nutrigenomics and The Future of Dietetics PracticeDocument2 pagesGenetic Dietetics - Nutrigenomics and The Future of Dietetics PracticeIffa Karina PermatasariNo ratings yet
- ASE Latest POCUS Peds GuidelineDocument13 pagesASE Latest POCUS Peds GuidelinekingbavaNo ratings yet
- Interest in Research Among Medical Students: Challenges For The Undergraduate EducationDocument7 pagesInterest in Research Among Medical Students: Challenges For The Undergraduate EducationsalmansecNo ratings yet
- KAM Eng 2Document6 pagesKAM Eng 2Dóri PappNo ratings yet
- Cdem 18june WebDocument32 pagesCdem 18june WebRicardo Jonathan Ayala GarciaNo ratings yet
- Chest Physiotherapy in Mechanically Ventilated Children: A ReviewDocument8 pagesChest Physiotherapy in Mechanically Ventilated Children: A Reviewganesh goreNo ratings yet
- Autópsia No EnsinoDocument2 pagesAutópsia No EnsinoguyzkdzrbdcogvwsumNo ratings yet
- Isscr Coreconceptsinstemcellbiology November2020Document49 pagesIsscr Coreconceptsinstemcellbiology November2020MKGUNo ratings yet
- Mandatory Resident Work Hour LimitationsDocument2 pagesMandatory Resident Work Hour LimitationsSteven GodelmanNo ratings yet
- Contemporary Global Perspectives of Medical Students On Research During Undergraduate Medical Education A Systematic Literature ReviewDocument14 pagesContemporary Global Perspectives of Medical Students On Research During Undergraduate Medical Education A Systematic Literature Reviewhabihabi0609No ratings yet
- This Content Downloaded From 14.139.228.235 On Fri, 12 Feb 2021 08:39:50 UTCDocument3 pagesThis Content Downloaded From 14.139.228.235 On Fri, 12 Feb 2021 08:39:50 UTCsparsh lalNo ratings yet
- Master Thesis Drug DeliveryDocument4 pagesMaster Thesis Drug Deliveryaflnbwmjhdinys100% (2)
- Trends in Publications About Cerebral PalsyDocument11 pagesTrends in Publications About Cerebral Palsycvdk8dc8sbNo ratings yet
- Nej MP 1510394Document3 pagesNej MP 1510394anggiNo ratings yet
- 1 s2.0 S016517811930602X MainDocument6 pages1 s2.0 S016517811930602X MainIim Roatul HamidahNo ratings yet
- Grech Grech 2020 Stroke Knowledge Developing A Framework For Data Integration in A Sequential Exploratory Mixed MethodDocument14 pagesGrech Grech 2020 Stroke Knowledge Developing A Framework For Data Integration in A Sequential Exploratory Mixed Methodwani zolNo ratings yet
- Getting The Most From Your History and PhysicalDocument9 pagesGetting The Most From Your History and PhysicalSamian QuaziNo ratings yet
- Ross2007 Abs AjogDocument2 pagesRoss2007 Abs AjogAbdillah FauziNo ratings yet
- The Clinical Reasoning Mapping Exercise (CResME) )Document5 pagesThe Clinical Reasoning Mapping Exercise (CResME) )Frederico PóvoaNo ratings yet
- Fenotipos Sepsis 1 PDFDocument2 pagesFenotipos Sepsis 1 PDFGerardo LermaNo ratings yet
- Develop Med Child Neuro - 2023 - Mayston - The Bobath Clinical Reasoning Framework A Systems Science Approach To TheDocument9 pagesDevelop Med Child Neuro - 2023 - Mayston - The Bobath Clinical Reasoning Framework A Systems Science Approach To ThenevenkaterapeutaNo ratings yet
- Family-Centred ServiceDocument20 pagesFamily-Centred ServiceCynthia RodriguesNo ratings yet
- A Guide To Competencies, Educational Goals, and Learning Objectives For Teaching Medical Histology in An Undergraduate Medical Education SettingDocument12 pagesA Guide To Competencies, Educational Goals, and Learning Objectives For Teaching Medical Histology in An Undergraduate Medical Education SettingahmedNo ratings yet
- Reinvigorating The Clinical Examination For The 21st CenturDocument6 pagesReinvigorating The Clinical Examination For The 21st CenturAnnette GaspardNo ratings yet
- Chang-With A Little Help From Machine Learning, Precision Radiology Can Be Feasible - 2018-RadiologyDocument2 pagesChang-With A Little Help From Machine Learning, Precision Radiology Can Be Feasible - 2018-RadiologyAsik AliNo ratings yet
- NIH Public AccessDocument14 pagesNIH Public AccessJamesNo ratings yet
- 3.giacomami Users Quides To The MedicalDocument6 pages3.giacomami Users Quides To The MedicalMayra De LeonNo ratings yet
- Nutrigenomics and Nutrigenetics: The Emerging Faces of NutritionDocument16 pagesNutrigenomics and Nutrigenetics: The Emerging Faces of Nutritionmulat aytoNo ratings yet
- 462 1 FullDocument1 page462 1 FullEVELYN EZEKWENo ratings yet
- I2333 0406 21 4 LeeDocument7 pagesI2333 0406 21 4 LeePablo Segales BautistaNo ratings yet
- Guidelines SBO (Small Bowel Obstruction)Document14 pagesGuidelines SBO (Small Bowel Obstruction)Ghege GuntaranNo ratings yet
- Practical Cytopathology: Frequently Asked QuestionsFrom EverandPractical Cytopathology: Frequently Asked QuestionsHuihong XuNo ratings yet
- Transfusion Reaction PDFDocument1 pageTransfusion Reaction PDFKah Man GohNo ratings yet
- SpleenAnatomy Functions Rupture HypersplenismDocument77 pagesSpleenAnatomy Functions Rupture HypersplenismKah Man GohNo ratings yet
- Diabetic Retinopathy Case 09Document2 pagesDiabetic Retinopathy Case 09Kah Man GohNo ratings yet
- Parenteral Drug Administration: Learning OutcomesDocument31 pagesParenteral Drug Administration: Learning OutcomesKah Man GohNo ratings yet
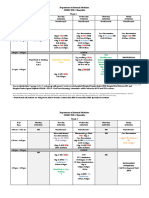
- Semester 6 Timetable 25 April 2016 To 10 June 2016 (GRP C) Revised 12 May 2016Document7 pagesSemester 6 Timetable 25 April 2016 To 10 June 2016 (GRP C) Revised 12 May 2016Kah Man GohNo ratings yet
- Opensheets Black JokeDocument34 pagesOpensheets Black JokebobNo ratings yet
- Project Report (Aniket18GSOB1010055, Sakshi18GSOB1010164, Rupali18GSOB1010192)Document25 pagesProject Report (Aniket18GSOB1010055, Sakshi18GSOB1010164, Rupali18GSOB1010192)vidhya vijayanNo ratings yet
- South Indian RecipesDocument7 pagesSouth Indian RecipesJagannath AcharyaNo ratings yet
- Richard-2019-9-29 - (PO 1048) PDFDocument1 pageRichard-2019-9-29 - (PO 1048) PDFLeslie Ali TapodocNo ratings yet
- BinggrisDocument11 pagesBinggrisDina Putri RachmandariNo ratings yet
- Thank-You For Downloading The SW Tool IQ-OQ-PQ Template!Document14 pagesThank-You For Downloading The SW Tool IQ-OQ-PQ Template!MichelleNo ratings yet
- Section Viii Div 1 Div 2 Div ComparisonDocument2 pagesSection Viii Div 1 Div 2 Div Comparisonapparaokr100% (5)
- Ahsan's CVDocument2 pagesAhsan's CVAhsan DilshadNo ratings yet
- Republic of The Philippines Department of Education Ugong Pasig National High SchoolDocument12 pagesRepublic of The Philippines Department of Education Ugong Pasig National High SchoolJOEL MONTERDENo ratings yet
- Genestealer Cult House Rules Form DAKKA DAKKADocument5 pagesGenestealer Cult House Rules Form DAKKA DAKKADaniel Locke100% (1)
- SLA GuideDocument205 pagesSLA GuidePeng Chiew Low100% (1)
- Earth Charter and The Global ImpactDocument27 pagesEarth Charter and The Global ImpactDaisyNo ratings yet
- Menstruation Disorders NotesDocument27 pagesMenstruation Disorders NotesemmaNo ratings yet
- Tiểu luận TemplateDocument7 pagesTiểu luận TemplateThảo NguyênNo ratings yet
- Elhussein 2007Document7 pagesElhussein 2007Elena DraganNo ratings yet
- Field & Herbarium MethodsDocument53 pagesField & Herbarium MethodsAshima JoshiNo ratings yet
- Face2face Pre-Intermediate Lesson 1CDocument11 pagesFace2face Pre-Intermediate Lesson 1CJean LoaizaNo ratings yet
- Livspace Interior Expo, HulkulDocument35 pagesLivspace Interior Expo, HulkulNitish KumarNo ratings yet
- 15life Cycle Costing PrintableDocument8 pages15life Cycle Costing Printablep99.subasNo ratings yet
- Ingles V e VIDocument314 pagesIngles V e VIAntonio MacaiaNo ratings yet
- How An Average Nigerian Can Cast Powerful Spells For Love, Money, Protection and Spiritual Power.Document22 pagesHow An Average Nigerian Can Cast Powerful Spells For Love, Money, Protection and Spiritual Power.Keysopedia WiredNo ratings yet
- Manual de Instruções Marantz SR-7500 DFU - 00 - CoverDocument56 pagesManual de Instruções Marantz SR-7500 DFU - 00 - CoverAntonio VidalNo ratings yet
- ASEAN ATM Master Planning Activity 4.2: AgendaDocument6 pagesASEAN ATM Master Planning Activity 4.2: AgendaXA Pakse Pakz ApprNo ratings yet
- Kumar Sabnani Org CultureDocument2 pagesKumar Sabnani Org CultureAayushi SinghNo ratings yet
- Volvo B5TL: When All You Need Is Everything in A Double Deck BusDocument13 pagesVolvo B5TL: When All You Need Is Everything in A Double Deck BusКонстантин КосаревNo ratings yet