Download as pdf or txt
You might also like
- Alcon Acrysof Iol Product CatalogDocument15 pagesAlcon Acrysof Iol Product CatalogtibbicihazlarintamiriNo ratings yet
- APAO2013 Scientific Program ScheduleDocument59 pagesAPAO2013 Scientific Program ScheduleMul YaniNo ratings yet
- Clinical Study: Long-Term Effects of Cataract Surgery On Tear Film ParametersDocument5 pagesClinical Study: Long-Term Effects of Cataract Surgery On Tear Film ParametersJohn ElfranNo ratings yet
- Accuracy of Biometry in Pediatric Cataract Extraction With Primary Intraocular Lens ImplantationDocument8 pagesAccuracy of Biometry in Pediatric Cataract Extraction With Primary Intraocular Lens ImplantationRodrigo BarreraNo ratings yet
- Demographic and Clinical Profile of Patients Who Underwent Refractive Surgery ScreeningDocument8 pagesDemographic and Clinical Profile of Patients Who Underwent Refractive Surgery ScreeningPierre A. RodulfoNo ratings yet
- Clinical Characteristics and Surgical Outcomes in Patients With Intermittent ExotropiaDocument6 pagesClinical Characteristics and Surgical Outcomes in Patients With Intermittent ExotropiaIkmal ShahromNo ratings yet
- Jabbar V and 2015Document7 pagesJabbar V and 2015annisaNo ratings yet
- Patient Safety During Sedation by Anesthesia ProfeDocument8 pagesPatient Safety During Sedation by Anesthesia ProfeIsmar MorenoNo ratings yet
- Lundstrom Etal JCRS 2018 Risk Factors For Refractive Error After Cataract SurgeryDocument16 pagesLundstrom Etal JCRS 2018 Risk Factors For Refractive Error After Cataract Surgeryhenok birukNo ratings yet
- Relationship of Dissociated Vertical Deviation and The Timing of Initial Surgery For Congenital EsotropiaDocument4 pagesRelationship of Dissociated Vertical Deviation and The Timing of Initial Surgery For Congenital EsotropiaMacarena AlvarezNo ratings yet
- Epidemiology and Clinical Characteristics of Episcleritis and Scleritis in Olmsted County, MinnesotaDocument8 pagesEpidemiology and Clinical Characteristics of Episcleritis and Scleritis in Olmsted County, MinnesotaApriansyah Arfandy AzisNo ratings yet
- Corneal and Conjunctival Injury Seen in Urgent Care Centres in IsraelDocument7 pagesCorneal and Conjunctival Injury Seen in Urgent Care Centres in IsraelOchi D. GreenNo ratings yet
- George - Are There Sex-Based Disparities in Cataract SurgeryDocument8 pagesGeorge - Are There Sex-Based Disparities in Cataract SurgerygeorgeNo ratings yet
- MN Community Measurement Total Knee Replacement Impact and Recommendation Document June 2010Document5 pagesMN Community Measurement Total Knee Replacement Impact and Recommendation Document June 2010ronnyNo ratings yet
- Venous Malformations Sclerotherapy Outcomes, Patient Satisfaction and Predictors of Treatment SuccessDocument7 pagesVenous Malformations Sclerotherapy Outcomes, Patient Satisfaction and Predictors of Treatment Successradhianie djanNo ratings yet
- Clinical Study: Outcome and Prognostic Factors For Traumatic Endophthalmitis Over A 5-Year PeriodDocument8 pagesClinical Study: Outcome and Prognostic Factors For Traumatic Endophthalmitis Over A 5-Year PeriodannisaNo ratings yet
- Honea-Mls 339 Final Paper 1Document9 pagesHonea-Mls 339 Final Paper 1api-744681971No ratings yet
- Eye 2011154 ADocument7 pagesEye 2011154 AAmba PutraNo ratings yet
- Articulo 2021 - EfectosDocument5 pagesArticulo 2021 - Efectosmilena cedeñoNo ratings yet
- Accuracy of Referral and Phone-Triage Diagnoses in An Eye Emergency DepartmentDocument3 pagesAccuracy of Referral and Phone-Triage Diagnoses in An Eye Emergency DepartmentBima RizkiNo ratings yet
- Endophthalmitis Following Cataract Surgery in Sweden. The 1998 National Prospective SurveyDocument4 pagesEndophthalmitis Following Cataract Surgery in Sweden. The 1998 National Prospective SurveySurendar KesavanNo ratings yet
- Aes 04 9Document6 pagesAes 04 9Ignasius HansNo ratings yet
- Eye Findings in Patients With Juvenile Dermatomyositis: Key Indexing TermsDocument6 pagesEye Findings in Patients With Juvenile Dermatomyositis: Key Indexing TermsOana BiancaNo ratings yet
- AygunDocument5 pagesAygunotheasNo ratings yet
- Network IIHS International Infant Hydrocephalus Study IVH Intraventricular HemorrhageDocument9 pagesNetwork IIHS International Infant Hydrocephalus Study IVH Intraventricular HemorrhageCrisu AlexandraNo ratings yet
- PRO 1 - MethodologyDocument9 pagesPRO 1 - MethodologyImran KhatriNo ratings yet
- 227 Manuscript 538 1 10 20210129Document5 pages227 Manuscript 538 1 10 20210129Ayele BizunehNo ratings yet
- Pi Is 0161642012005052Document8 pagesPi Is 0161642012005052Pra BowoNo ratings yet
- The Extent of Knowledge and Participation of The Staff Nurses On The Visual Infusion Phlebitis Program of Saint Anthony College HospitalDocument89 pagesThe Extent of Knowledge and Participation of The Staff Nurses On The Visual Infusion Phlebitis Program of Saint Anthony College HospitalWinj BudayNo ratings yet
- tmpC73A TMPDocument8 pagestmpC73A TMPFrontiersNo ratings yet
- Uveitis 2Document9 pagesUveitis 2srihandayaniakbarNo ratings yet
- Testicular Torsion and Risk Factors For Orchiectomy: Jonathan M. Mansbach, MD Peter Forbes, MA Craig Peters, MDDocument5 pagesTesticular Torsion and Risk Factors For Orchiectomy: Jonathan M. Mansbach, MD Peter Forbes, MA Craig Peters, MDDiah Sukmawati HidayahNo ratings yet
- Natural History and Outcome of Optic Pathway Gliomas in ChildrenDocument7 pagesNatural History and Outcome of Optic Pathway Gliomas in ChildrenCamilo Benavides BurbanoNo ratings yet
- 1 S PSCDocument8 pages1 S PSCKen WonNo ratings yet
- CDC Repeat Syphilis Infection and HIV Coinfection Among Men Who Have SexDocument16 pagesCDC Repeat Syphilis Infection and HIV Coinfection Among Men Who Have SexkikiNo ratings yet
- Coba Baca 36634-130622-2-PBDocument5 pagesCoba Baca 36634-130622-2-PBannisaNo ratings yet
- The Human Bite Injury: A Clinical Audit and Discussion Regarding The Management of This Alcohol Fuelled PhenomenonDocument4 pagesThe Human Bite Injury: A Clinical Audit and Discussion Regarding The Management of This Alcohol Fuelled PhenomenonJiff EstuNo ratings yet
- An Examination of The Ocular Signs of Blunt Eye Injuries in A Prospective ResearchDocument4 pagesAn Examination of The Ocular Signs of Blunt Eye Injuries in A Prospective ResearchInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Characteristics of Uveitis Presenting For The First Time in The Elderly Analysis of 91 Patients in A Tertiary CenterDocument9 pagesCharacteristics of Uveitis Presenting For The First Time in The Elderly Analysis of 91 Patients in A Tertiary CenterFrancescFranquesaNo ratings yet
- PIIS0002939422004007Document11 pagesPIIS0002939422004007Anca Florina GaceaNo ratings yet
- Development of an Electronic Frailty Index for Hospitalized Older Adults in SwedenDocument9 pagesDevelopment of an Electronic Frailty Index for Hospitalized Older Adults in SwedencharmyshkuNo ratings yet
- Dysphotopsia After Temporal Versus Superior Laser Peripheral Iridotomy - A Prospective Randomized Paired Eye TrialDocument9 pagesDysphotopsia After Temporal Versus Superior Laser Peripheral Iridotomy - A Prospective Randomized Paired Eye TrialHanna_RNo ratings yet
- Effect of Implementation of A Surgical Safety Checklist On Perioperative and Postoperative Complications at An Academic Institution in North AmericaDocument14 pagesEffect of Implementation of A Surgical Safety Checklist On Perioperative and Postoperative Complications at An Academic Institution in North AmericaMuhammad BasharatullahNo ratings yet
- Continued Endothelial Cell Loss Ten Years After Lens ImplantationDocument10 pagesContinued Endothelial Cell Loss Ten Years After Lens ImplantationPriscila MartínezNo ratings yet
- Penetrating Keratoplasty in Active Acanthamoeba KeratitisDocument5 pagesPenetrating Keratoplasty in Active Acanthamoeba Keratitisdrvishalkulkarni2007No ratings yet
- Does This Patient Have An Infection of A Chronic Wound?: The Rational Clinical ExaminationDocument7 pagesDoes This Patient Have An Infection of A Chronic Wound?: The Rational Clinical Examinationapi-181367805No ratings yet
- Research Article 'S Disease: Severity of Ocular: Vision-Threatening Behcet Involvement PredictorsDocument7 pagesResearch Article 'S Disease: Severity of Ocular: Vision-Threatening Behcet Involvement PredictorsdeswitrigintaNo ratings yet
- Factors Associated With The Time To Complete Clinical Exome - 2022 - Genetics inDocument6 pagesFactors Associated With The Time To Complete Clinical Exome - 2022 - Genetics inronaldquezada038No ratings yet
- Medico-Legal Aspects of Altered Sensation Following Tic TX Givol Et Al 2011Document6 pagesMedico-Legal Aspects of Altered Sensation Following Tic TX Givol Et Al 2011Edward AbadiaNo ratings yet
- 564 Full PDFDocument7 pages564 Full PDFMi MihaelaNo ratings yet
- Azad 2019Document7 pagesAzad 2019Eka BagaskaraNo ratings yet
- Eye Banking and Corneal Transplantation in Tertiary Care Hospital Located in Rural AreaDocument6 pagesEye Banking and Corneal Transplantation in Tertiary Care Hospital Located in Rural AreaIOSR Journal of PharmacyNo ratings yet
- Incidence of PostcataractDocument8 pagesIncidence of PostcataractSurendar KesavanNo ratings yet
- The Prevalence of OpenDocument17 pagesThe Prevalence of OpenShaney_flNo ratings yet
- What Are The Patterns of Compliance Whith Early Warning TrackDocument9 pagesWhat Are The Patterns of Compliance Whith Early Warning TrackPAULA SORAIA CHENNo ratings yet
- Literature Review PterygiumDocument7 pagesLiterature Review Pterygiumafmzzaadfjygyf100% (1)
- Knowlegde and Willingness To Donate Eye Among Medical Doctors in Delta StateDocument7 pagesKnowlegde and Willingness To Donate Eye Among Medical Doctors in Delta StateInternational Organization of Scientific Research (IOSR)No ratings yet
- TranslateDocument5 pagesTranslatenoviadewaniNo ratings yet
- Test PaperDocument4 pagesTest PaperJOSE MANUEL EspirituNo ratings yet
- Biomedicines 11 03124Document11 pagesBiomedicines 11 03124Hello PtaiNo ratings yet
- Baseline Visual Field Findings in The Idiopathic Intracranial Hypertension Treatment Trial IIHTTDocument8 pagesBaseline Visual Field Findings in The Idiopathic Intracranial Hypertension Treatment Trial IIHTTFFarfanNo ratings yet
- Blepharitis: A Comprehensive Clinical GuideFrom EverandBlepharitis: A Comprehensive Clinical GuideAsim V. FarooqNo ratings yet
- Management of Intraocular Foreign BodiesDocument7 pagesManagement of Intraocular Foreign BodiesdebbyNo ratings yet
- Corneal SurgeryDocument159 pagesCorneal Surgerydebby100% (3)
- Management and Treatment of Herpes Simplex Keratitis: June 2016Document8 pagesManagement and Treatment of Herpes Simplex Keratitis: June 2016debbyNo ratings yet
- Diseases of The Cornea Prof. Zoltán Zsolt NagyDocument123 pagesDiseases of The Cornea Prof. Zoltán Zsolt NagydebbyNo ratings yet
- 1 2 2018 Lens Induced Glaucoma Bhuvan PDFDocument50 pages1 2 2018 Lens Induced Glaucoma Bhuvan PDFDara AprillyantiNo ratings yet
- Eyesi Surgical BrochureDocument16 pagesEyesi Surgical BrochureHaag-Streit UK (HS-UK)No ratings yet
- Cataract: Nature Reviews Disease Primers June 2015Document16 pagesCataract: Nature Reviews Disease Primers June 2015Adi PratamaNo ratings yet
- Discuss The Major Health Problems in IndiaDocument4 pagesDiscuss The Major Health Problems in Indianaresh BNo ratings yet
- Astigmatism After Cataract Surgery: Nylon Versus Mersilene: Five-Year DataDocument3 pagesAstigmatism After Cataract Surgery: Nylon Versus Mersilene: Five-Year Dataandrema123No ratings yet
- Exploring and Understanding The Benefits of Torsional PhacoemulsificationDocument13 pagesExploring and Understanding The Benefits of Torsional Phacoemulsificationthubui90No ratings yet
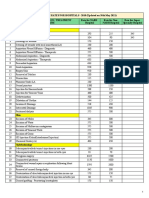
- CGHS Mumbai 2010 Rates Updated On 30th May 2021Document49 pagesCGHS Mumbai 2010 Rates Updated On 30th May 2021zemse11715No ratings yet
- Eye Essentials Cataract Assessment Classification and ManagementDocument245 pagesEye Essentials Cataract Assessment Classification and ManagementMaíra Dias100% (7)
- A Guide: To Choose Right IOL - Cataract SurgeryDocument25 pagesA Guide: To Choose Right IOL - Cataract SurgeryChristopherJamesNo ratings yet
- National Programme For Control of Blindness: Assistant Prof., Deptt. of Community Medicine GMCH ChandigarhDocument23 pagesNational Programme For Control of Blindness: Assistant Prof., Deptt. of Community Medicine GMCH ChandigarhSumon SarkarNo ratings yet
- Tecnis Eyhance SpecSheetDocument2 pagesTecnis Eyhance SpecSheetShripad BhawsarNo ratings yet
- AvanseePreset Review Article Miyake Et Al EuroTimes - Sept 2014Document12 pagesAvanseePreset Review Article Miyake Et Al EuroTimes - Sept 2014Hombre69No ratings yet
- Pearls in PPCDocument5 pagesPearls in PPCRajinder Kumar BassanNo ratings yet
- Blindness Control ProgrammeDocument6 pagesBlindness Control Programmearunjv1234No ratings yet
- CGHS Rates - LucknowDocument38 pagesCGHS Rates - LucknowBITS PILANI WILP MTQMNo ratings yet
- Bjo Malignant Glaucoma - FullDocument5 pagesBjo Malignant Glaucoma - FullABID ALI100% (1)
- Tasya - Lam2015Document16 pagesTasya - Lam2015Yuwan RamjadaNo ratings yet
- MUHS Dissertation 13-14Document75 pagesMUHS Dissertation 13-14Juned LabbaiNo ratings yet
- IOL HandoutDocument8 pagesIOL HandoutIhsan AnasNo ratings yet
- Combined Cataract and Glaucoma SurgeryDocument20 pagesCombined Cataract and Glaucoma SurgerymanognaaaaNo ratings yet
- Nylon LoopDocument4 pagesNylon LooporlandgpicadoNo ratings yet
- Avanti AngioVue Brochure 2018Document22 pagesAvanti AngioVue Brochure 2018Roberto Vega FloresNo ratings yet
- Cataract Surgery With Phaco & Femtophaco TechniqueDocument193 pagesCataract Surgery With Phaco & Femtophaco TechniqueRajesh GuptaNo ratings yet
- Guide PDFDocument84 pagesGuide PDFbiomeditechNo ratings yet
- Trust, Compassion and Loyalty Seeing ClearlyDocument5 pagesTrust, Compassion and Loyalty Seeing Clearlysvetlana_sdNo ratings yet
- Complicationts of Cataract Surgery (Other Anterior Segment Complications)Document30 pagesComplicationts of Cataract Surgery (Other Anterior Segment Complications)Hikban FiqhiNo ratings yet
- UntitledDocument20 pagesUntitledpratapekkaNo ratings yet
- Updated Ico Residency CurriculumDocument219 pagesUpdated Ico Residency CurriculumEdoga Chima EmmanuelNo ratings yet