Download as pdf or txt
You might also like
- Fast Facts for Patients and Supporters: Cholangiocarcinoma: A cancer of the bile duct and liver Information + Taking Control = Best OutcomeFrom EverandFast Facts for Patients and Supporters: Cholangiocarcinoma: A cancer of the bile duct and liver Information + Taking Control = Best OutcomeNo ratings yet
- Addiction: The Process of AddictionDocument5 pagesAddiction: The Process of AddictionRaudel GlezNo ratings yet
- Disorders of PancreasDocument17 pagesDisorders of PancreasjonasNo ratings yet
- NMSC Gross HematuriaDocument41 pagesNMSC Gross HematuriaStoned PickleNo ratings yet
- UTUCDocument39 pagesUTUCShalini shreeNo ratings yet
- Eva Bolton Haematuria Presentation WebDocument52 pagesEva Bolton Haematuria Presentation WebereczkieNo ratings yet
- Hepatocellular Carcinoma and Other Hepatic MassesDocument59 pagesHepatocellular Carcinoma and Other Hepatic MassesIsaac MwangiNo ratings yet
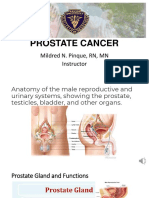
- Prostate Cancer 111606Document31 pagesProstate Cancer 111606abd12medyNo ratings yet
- Hematuria: Ikobho A. DDocument28 pagesHematuria: Ikobho A. DPrincewill SeiyefaNo ratings yet
- HematuriaDocument15 pagesHematurianisaw_2No ratings yet
- TP Thyroid Nodules 1Document59 pagesTP Thyroid Nodules 1Meaw Thitirat SupasilNo ratings yet
- Cystic Diseases of The Kidney. Renal NeoplasmsDocument31 pagesCystic Diseases of The Kidney. Renal NeoplasmsFate ChanNo ratings yet
- Case Based Teaching - Urology: Haematuria & Renal TransplantDocument21 pagesCase Based Teaching - Urology: Haematuria & Renal Transplantamoody95No ratings yet
- The Paris System For Reporting Urinary CytopathologyDocument32 pagesThe Paris System For Reporting Urinary CytopathologyReymes BusterNo ratings yet
- Brad J Hornberger Cystoscopy Indications and Preparation. UAPA CME Conference 2012 (30 Min)Document36 pagesBrad J Hornberger Cystoscopy Indications and Preparation. UAPA CME Conference 2012 (30 Min)Cristian OrozcoNo ratings yet
- Testicular TumorsDocument35 pagesTesticular TumorsHafizur RashidNo ratings yet
- MS, Frcs (England), Frcs (Edinburgh), Frcs (Glasgow)Document52 pagesMS, Frcs (England), Frcs (Edinburgh), Frcs (Glasgow)Anis HospitalNo ratings yet
- Approach To Patient With Renal DiseaseDocument74 pagesApproach To Patient With Renal DiseaseSaja SaqerNo ratings yet
- Urology Sample Osce Exam e PDFDocument8 pagesUrology Sample Osce Exam e PDFLana LocoNo ratings yet
- Back To Basics - Urology - Dr. James Watterson 2009 - CompressedDocument171 pagesBack To Basics - Urology - Dr. James Watterson 2009 - CompressedDr Anais AsimNo ratings yet
- Evaluation and Management of HematuriaDocument26 pagesEvaluation and Management of Hematuriaoki777jxNo ratings yet
- Renal Cell Carcinoma: DR - Amit Gupta Associate Professor Dept. of SurgeryDocument20 pagesRenal Cell Carcinoma: DR - Amit Gupta Associate Professor Dept. of SurgeryvitelinductNo ratings yet
- Cervical CancerDocument36 pagesCervical CancerPro fatherNo ratings yet
- Hepatocellular CarcinomaDocument62 pagesHepatocellular CarcinomaWilliams Emmanuel AdeyeyeNo ratings yet
- Abnormal Cervical SmearDocument63 pagesAbnormal Cervical SmearAkhmal SidekNo ratings yet
- Urological TumoursDocument68 pagesUrological TumoursDr Anais AsimNo ratings yet
- HematuriaDocument31 pagesHematuriaSiti Zainab Bani PurwanaNo ratings yet
- Benign Prostatic HyperplasiaDocument36 pagesBenign Prostatic Hyperplasiamomodou s jallowNo ratings yet
- Imaging of Acute PancreatitisDocument53 pagesImaging of Acute PancreatitisLazar VučetićNo ratings yet
- Common Bile Duct Stones StrictureDocument48 pagesCommon Bile Duct Stones StrictureSyarif MalawatNo ratings yet
- Faiza Hashim Soomro PG-Gen SurgeryDocument47 pagesFaiza Hashim Soomro PG-Gen SurgeryFaiza Hashim SoomroNo ratings yet
- Gall Bladder CarcinomaDocument29 pagesGall Bladder CarcinomaUsman FarooqNo ratings yet
- Urothelial Tumors of The Upper Urinary Tract FixDocument25 pagesUrothelial Tumors of The Upper Urinary Tract FixAgung IndraNo ratings yet
- Liver BiopsyDocument4 pagesLiver BiopsyLouis Fortunato100% (1)
- Guidelines For UrologyDocument91 pagesGuidelines For UrologyAruna HarikrishnanNo ratings yet
- Colon CancerDocument41 pagesColon Cancervaishali TayadeNo ratings yet
- Renal Cell CarcinomaDocument9 pagesRenal Cell CarcinomaFabb NelsonNo ratings yet
- Tumors of The Kidney and Urinary BladerDocument76 pagesTumors of The Kidney and Urinary BladerTaufik Gumilar WahyudinNo ratings yet
- Faculty of Medicine NR - Ii Department of Surgery NR - Ii: Diseases of The Biliary TractDocument40 pagesFaculty of Medicine NR - Ii Department of Surgery NR - Ii: Diseases of The Biliary TractGalina LozovanuNo ratings yet
- Urogenital Cancers: - Renal Cell Ca - Bladder Ca - Renal Pelvis & Ureter - BPH & Prostate CaDocument17 pagesUrogenital Cancers: - Renal Cell Ca - Bladder Ca - Renal Pelvis & Ureter - BPH & Prostate CaAli Husain Abdul KadirNo ratings yet
- Surg 2 JaundicedDocument94 pagesSurg 2 Jaundicedapi-3728522No ratings yet
- Ca CervixDocument48 pagesCa CervixRanjita BainsNo ratings yet
- Radiologi Edit-1Document50 pagesRadiologi Edit-1Resi OfzanNo ratings yet
- Prof. Ziv Ben-Ari Liver Institute Rabin Medical CenterDocument62 pagesProf. Ziv Ben-Ari Liver Institute Rabin Medical CenterLigia Ariana BancuNo ratings yet
- Case StudiesDocument6 pagesCase StudiesPatricia CruzNo ratings yet
- RadiologiDocument54 pagesRadiologiresi silviaNo ratings yet
- Carcinomagallbladder PDFDocument61 pagesCarcinomagallbladder PDFZaki DhiifNo ratings yet
- HEPATOMADocument30 pagesHEPATOMASemestaNo ratings yet
- Topic 10Document10 pagesTopic 1089qqzp4yhkNo ratings yet
- Approach To The Patient With Hematuria: Paul D. Simmons, MD St. Mary's Family Medicine Residency Grand JunctionDocument41 pagesApproach To The Patient With Hematuria: Paul D. Simmons, MD St. Mary's Family Medicine Residency Grand JunctionMichael Spica RampangileiNo ratings yet
- Pancreaticcancer 150917114601 Lva1 App6891Document30 pagesPancreaticcancer 150917114601 Lva1 App6891enam professorNo ratings yet
- 9 Urinary and Male GenitalDocument31 pages9 Urinary and Male GenitalFlavia CatalinaNo ratings yet
- Seminar On Tumor of Genito-Urinary SystemDocument33 pagesSeminar On Tumor of Genito-Urinary SystemLakshay AroraNo ratings yet
- Squamous Cell CarcinomaDocument53 pagesSquamous Cell CarcinomaWacky BlankNo ratings yet
- HematuriaDocument4 pagesHematuriaArian SuryaNo ratings yet
- Abdominaltraumaanoverview-171025062135 4Document75 pagesAbdominaltraumaanoverview-171025062135 4Ion AndreeaNo ratings yet
- Liver TraumaDocument7 pagesLiver TraumanouradreamNo ratings yet
- 11 Prostate CancerDocument52 pages11 Prostate Cancerclaire yowsNo ratings yet
- Thrombophilia: Duha Alharbi, MD InternDocument30 pagesThrombophilia: Duha Alharbi, MD InternabrarNo ratings yet
- Hello PandaDocument1 pageHello PandajenegneNo ratings yet
- Hshshhshsben SNDocument3 pagesHshshhshsben SNjenegneNo ratings yet
- GFGFGFDocument5 pagesGFGFGFjenegneNo ratings yet
- Measurements in Femoro-Acetabular Impingement: How To Doit?Document33 pagesMeasurements in Femoro-Acetabular Impingement: How To Doit?jenegneNo ratings yet
- Nutrients: Use of An Extract of Annona Muricata Linn To Prevent High-Fat Diet Induced Metabolic Disorders in C57BLDocument22 pagesNutrients: Use of An Extract of Annona Muricata Linn To Prevent High-Fat Diet Induced Metabolic Disorders in C57BLjenegneNo ratings yet
- Measurements in Femoro-Acetabular Impingement: How To Doit?Document33 pagesMeasurements in Femoro-Acetabular Impingement: How To Doit?jenegneNo ratings yet
- Banadoz ® Cefpodoxime: CompositionDocument5 pagesBanadoz ® Cefpodoxime: CompositionjenegneNo ratings yet
- Journal of Clinical and Basic Cardiology: WWW - Kup.at/jcbcDocument6 pagesJournal of Clinical and Basic Cardiology: WWW - Kup.at/jcbcjenegneNo ratings yet
- 9164 62159 1 PBDocument12 pages9164 62159 1 PBjenegneNo ratings yet
- Overview of Viral MyositisDocument3 pagesOverview of Viral MyositisemirkurtalicNo ratings yet
- None C9efb7c9Document6 pagesNone C9efb7c9liana iwiwNo ratings yet
- Homeopathy Research Evidence Base 7-12-2017 PDFDocument214 pagesHomeopathy Research Evidence Base 7-12-2017 PDFGanesh ganguly GMNo ratings yet
- Nurse Practitioner Nurse in Philadelphia PA Resume Deborah StallworthDocument2 pagesNurse Practitioner Nurse in Philadelphia PA Resume Deborah StallworthDeborah StallworthNo ratings yet
- Abdominal Aortic AneurysmDocument44 pagesAbdominal Aortic AneurysmAkhilMuraleedharan100% (2)
- Applicable For Third & Fourth Year Subject Homoeopathic Materia MedicaDocument16 pagesApplicable For Third & Fourth Year Subject Homoeopathic Materia MedicaRahul MaliNo ratings yet
- Prophasedx Laboratory Phone: (855) 982-1100Document2 pagesProphasedx Laboratory Phone: (855) 982-1100ommanon15 aNo ratings yet
- High Risk NewbornDocument68 pagesHigh Risk NewbornjeshemaNo ratings yet
- Granulomatous InflammationDocument96 pagesGranulomatous InflammationIvonne Trujillo TorbiscoNo ratings yet
- Editorial Intro DR Jessica Rose-The Lies Vaccinologists Tell Themselves - VAERS Receives Due ScrutinyDocument3 pagesEditorial Intro DR Jessica Rose-The Lies Vaccinologists Tell Themselves - VAERS Receives Due ScrutinySY LodhiNo ratings yet
- Cardiovascular Examination FinalDocument28 pagesCardiovascular Examination FinalAllen Caine Taabbil100% (1)
- ICD-10 PodiatryDocument25 pagesICD-10 PodiatryAnonymous kdBDppigENo ratings yet
- Study Data Reviewer's Guide: LDCP, Inc. Study LDCP-0242-005Document15 pagesStudy Data Reviewer's Guide: LDCP, Inc. Study LDCP-0242-005anon_181306460No ratings yet
- Chapter 109. Nursing ServicesDocument10 pagesChapter 109. Nursing ServicesTarun SoniNo ratings yet
- The Effects of Active Break and Postural Shift Interventions On Recovery FromDocument8 pagesThe Effects of Active Break and Postural Shift Interventions On Recovery FromNiko TrogerNo ratings yet
- Please Stand by ..: © Business & Legal Reports, Inc. 1110Document37 pagesPlease Stand by ..: © Business & Legal Reports, Inc. 1110Johanamhy PanergoNo ratings yet
- Bear Cub 750 - Quick User GuideDocument2 pagesBear Cub 750 - Quick User GuideSn DayanidhiNo ratings yet
- Allergy - 2022 - Kallieri - RELIght A Two Year REal LIfe Study of Mepolizumab in Patients With Severe Eosinophilic AsTHmaDocument5 pagesAllergy - 2022 - Kallieri - RELIght A Two Year REal LIfe Study of Mepolizumab in Patients With Severe Eosinophilic AsTHmaRamon RondoNo ratings yet
- Ped CardioDocument18 pagesPed CardioIdioness100% (1)
- Assessment of The AbdomenDocument6 pagesAssessment of The Abdomenmalyn1218No ratings yet
- Bed Site Teaching: Ridwan Permana (712014027) Preceptor: Dr. Rizal Daulay, SP - OT.,MARSDocument21 pagesBed Site Teaching: Ridwan Permana (712014027) Preceptor: Dr. Rizal Daulay, SP - OT.,MARSRidwan PermanaNo ratings yet
- Cefoxitin Drug StudyDocument3 pagesCefoxitin Drug StudyBea Dela Cena100% (2)
- Health Informatics Exam AnswersDocument8 pagesHealth Informatics Exam Answersnajib TibizukaNo ratings yet
- Module 1 - IS-PEFRDocument7 pagesModule 1 - IS-PEFRRenea Joy ArruejoNo ratings yet
- IPX066 (Rytary) : A New Medication For Parkinson's Disease, Robert A. Hauser MDDocument8 pagesIPX066 (Rytary) : A New Medication For Parkinson's Disease, Robert A. Hauser MDRobert A. Hauser, MDNo ratings yet
- System 5000 Electrosurgical Unit (ESU)Document4 pagesSystem 5000 Electrosurgical Unit (ESU)George VlNo ratings yet
- Management of Chronic Hepatitis B in AdultsDocument76 pagesManagement of Chronic Hepatitis B in AdultsLan AllemNo ratings yet
- Buscopan - Medicine To Treat Stomach Cramps and IBS - NHSDocument9 pagesBuscopan - Medicine To Treat Stomach Cramps and IBS - NHSAdityaWijayaNo ratings yet