
Articulo SOT
Articulo SOT
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A6 C5 Parts ListDocument37 pagesA6 C5 Parts ListOmar Ordorica88% (8)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Gay Kid and Fat Chick (03.14.13) - Bo BurnhamDocument114 pagesGay Kid and Fat Chick (03.14.13) - Bo BurnhamDaryl BastienNo ratings yet
- Kimble K2200C PartsDocument202 pagesKimble K2200C Partsviemey195250% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Title Associated With Instrumentation Feature Vocal KeyDocument15 pagesTitle Associated With Instrumentation Feature Vocal KeyKCNo ratings yet
- Clothing Catalog TemplateDocument14 pagesClothing Catalog TemplateJAVIER MAMANINo ratings yet
- Aku PusingDocument2 pagesAku Pusingdanishzahabi1No ratings yet
- Massey Ferguson 2705 TRACTOR Service Parts Catalogue Manual (Part Number 651415)Document16 pagesMassey Ferguson 2705 TRACTOR Service Parts Catalogue Manual (Part Number 651415)hujiao6607280No ratings yet
- Royalty Mod TutorialsDocument39 pagesRoyalty Mod Tutorialsnuriasante242No ratings yet
- Undaunted Using Stuka JoeDocument4 pagesUndaunted Using Stuka JoeechdascribdNo ratings yet
- Neuro OSCE - Student Guide PDFDocument9 pagesNeuro OSCE - Student Guide PDFDAVE RYAN DELA CRUZ100% (1)
- Misfire, Hangfire, and StoppageDocument3 pagesMisfire, Hangfire, and StoppageShaik Mudassar Nazar100% (1)
- Advantage Plays BlackjackDocument2 pagesAdvantage Plays BlackjackAngela BrownNo ratings yet
- HyperFlipz DFYDocument7 pagesHyperFlipz DFYAlex Van EckNo ratings yet
- Allison AT540Document1 pageAllison AT540francy ramirezNo ratings yet
- Air Conditioning Fundamentals: ©2000 Caterpillar IncDocument13 pagesAir Conditioning Fundamentals: ©2000 Caterpillar IncAnonymous NtS775PYyNo ratings yet
- 2015 Candelaria Intl Derby ResultsDocument25 pages2015 Candelaria Intl Derby ResultsByron PojolNo ratings yet
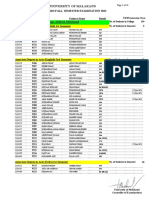
- ADA - ADS Fall Semester Examinations Results 2022Document41 pagesADA - ADS Fall Semester Examinations Results 2022Fida HussainNo ratings yet
- AvadhanaDocument21 pagesAvadhanavikasargodNo ratings yet
- Projectile AssignmentDocument8 pagesProjectile Assignmentmoon007000No ratings yet
- All Venn DiagramsDocument20 pagesAll Venn Diagramssyam17masterNo ratings yet
- Quiz 2Document4 pagesQuiz 2Ijaz Talib Classical MechanicsNo ratings yet
- 7227 - MasterstrokeAugustWeek 1 FINALDocument42 pages7227 - MasterstrokeAugustWeek 1 FINALVikalp YadavNo ratings yet
- Drum Brakes ManualDocument7 pagesDrum Brakes Manualrobjones33No ratings yet
- PHATDocument9 pagesPHATPontic47No ratings yet
- CBSE Class 12 Physical EducationDocument32 pagesCBSE Class 12 Physical EducationRamandeepSinghNo ratings yet
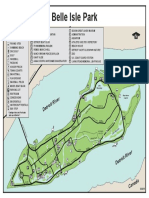
- DNR MapDocument1 pageDNR Mapmichael prasciusNo ratings yet
- Gca State Level Childrens Chess TournamentDocument2 pagesGca State Level Childrens Chess TournamentManikandan TayalanNo ratings yet
- L316 15MY AVM 110 130 INDUSTRIAL 6PP tcm295-87386Document6 pagesL316 15MY AVM 110 130 INDUSTRIAL 6PP tcm295-87386AliNo ratings yet
- 1) Tss-Still Column Reboiler, Rev.ADocument1 page1) Tss-Still Column Reboiler, Rev.AKiran KumarNo ratings yet
- Comenzi AmxmodxDocument4 pagesComenzi AmxmodxaltundevaNo ratings yet





































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A6 C5 Parts ListDocument37 pagesA6 C5 Parts ListOmar Ordorica88% (8)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Gay Kid and Fat Chick (03.14.13) - Bo BurnhamDocument114 pagesGay Kid and Fat Chick (03.14.13) - Bo BurnhamDaryl BastienNo ratings yet
- Kimble K2200C PartsDocument202 pagesKimble K2200C Partsviemey195250% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Title Associated With Instrumentation Feature Vocal KeyDocument15 pagesTitle Associated With Instrumentation Feature Vocal KeyKCNo ratings yet
- Clothing Catalog TemplateDocument14 pagesClothing Catalog TemplateJAVIER MAMANINo ratings yet
- Aku PusingDocument2 pagesAku Pusingdanishzahabi1No ratings yet
- Massey Ferguson 2705 TRACTOR Service Parts Catalogue Manual (Part Number 651415)Document16 pagesMassey Ferguson 2705 TRACTOR Service Parts Catalogue Manual (Part Number 651415)hujiao6607280No ratings yet
- Royalty Mod TutorialsDocument39 pagesRoyalty Mod Tutorialsnuriasante242No ratings yet
- Undaunted Using Stuka JoeDocument4 pagesUndaunted Using Stuka JoeechdascribdNo ratings yet
- Neuro OSCE - Student Guide PDFDocument9 pagesNeuro OSCE - Student Guide PDFDAVE RYAN DELA CRUZ100% (1)
- Misfire, Hangfire, and StoppageDocument3 pagesMisfire, Hangfire, and StoppageShaik Mudassar Nazar100% (1)
- Advantage Plays BlackjackDocument2 pagesAdvantage Plays BlackjackAngela BrownNo ratings yet
- HyperFlipz DFYDocument7 pagesHyperFlipz DFYAlex Van EckNo ratings yet
- Allison AT540Document1 pageAllison AT540francy ramirezNo ratings yet
- Air Conditioning Fundamentals: ©2000 Caterpillar IncDocument13 pagesAir Conditioning Fundamentals: ©2000 Caterpillar IncAnonymous NtS775PYyNo ratings yet
- 2015 Candelaria Intl Derby ResultsDocument25 pages2015 Candelaria Intl Derby ResultsByron PojolNo ratings yet
- ADA - ADS Fall Semester Examinations Results 2022Document41 pagesADA - ADS Fall Semester Examinations Results 2022Fida HussainNo ratings yet
- AvadhanaDocument21 pagesAvadhanavikasargodNo ratings yet
- Projectile AssignmentDocument8 pagesProjectile Assignmentmoon007000No ratings yet
- All Venn DiagramsDocument20 pagesAll Venn Diagramssyam17masterNo ratings yet
- Quiz 2Document4 pagesQuiz 2Ijaz Talib Classical MechanicsNo ratings yet
- 7227 - MasterstrokeAugustWeek 1 FINALDocument42 pages7227 - MasterstrokeAugustWeek 1 FINALVikalp YadavNo ratings yet
- Drum Brakes ManualDocument7 pagesDrum Brakes Manualrobjones33No ratings yet
- PHATDocument9 pagesPHATPontic47No ratings yet
- CBSE Class 12 Physical EducationDocument32 pagesCBSE Class 12 Physical EducationRamandeepSinghNo ratings yet
- DNR MapDocument1 pageDNR Mapmichael prasciusNo ratings yet
- Gca State Level Childrens Chess TournamentDocument2 pagesGca State Level Childrens Chess TournamentManikandan TayalanNo ratings yet
- L316 15MY AVM 110 130 INDUSTRIAL 6PP tcm295-87386Document6 pagesL316 15MY AVM 110 130 INDUSTRIAL 6PP tcm295-87386AliNo ratings yet
- 1) Tss-Still Column Reboiler, Rev.ADocument1 page1) Tss-Still Column Reboiler, Rev.AKiran KumarNo ratings yet
- Comenzi AmxmodxDocument4 pagesComenzi AmxmodxaltundevaNo ratings yet