
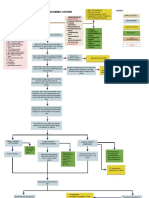
Acute Back Pain and Cauda Equina: Key Points
Acute Back Pain and Cauda Equina: Key Points
You might also like
- Acute Ischemic Stroke Concept MapDocument6 pagesAcute Ischemic Stroke Concept MapMoonyeen Jann Casera Balic100% (2)
- Low Back Pain 2018Document18 pagesLow Back Pain 2018Salazar Ángel100% (1)
- 2.5 NotesDocument7 pages2.5 NotesKenneth MelchorNo ratings yet
- The Treatment of Neck and Upper Back Pain With AcuDocument6 pagesThe Treatment of Neck and Upper Back Pain With AcuMohmmad Hossein NazariNo ratings yet
- Evidence Based Physiotherapy Management of A Cervical Radiculopathy PatientDocument9 pagesEvidence Based Physiotherapy Management of A Cervical Radiculopathy PatientDr Abdallah BahaaNo ratings yet
- Interventions in Chronic Pain ManagementDocument4 pagesInterventions in Chronic Pain ManagementwladjaNo ratings yet
- Cleveland Clinic Journal of Medicine 2007 Klineberg 905 13Document9 pagesCleveland Clinic Journal of Medicine 2007 Klineberg 905 13Sohaib AliNo ratings yet
- Assessment and Management of Acute Low Back Pain - American Family PhysicianDocument9 pagesAssessment and Management of Acute Low Back Pain - American Family PhysiciancaralivroNo ratings yet
- Discogenic LBP Revised September 2017Document13 pagesDiscogenic LBP Revised September 2017Clinton Franda Markus SitanggangNo ratings yet
- Herniated Lumbar Intervertebral Disk: Epidemiology and Natural HistoryDocument6 pagesHerniated Lumbar Intervertebral Disk: Epidemiology and Natural HistoryGeysel SuarezNo ratings yet
- Advances in The Diagnosis and Management of Neck PainDocument19 pagesAdvances in The Diagnosis and Management of Neck PainJose Fernando DiezNo ratings yet
- Low Back Pain Guidelines-Reduced2Document26 pagesLow Back Pain Guidelines-Reduced2ranggadr100% (1)
- Nurs 65 Medical Surgical Nursing: Cavite State UniversityDocument14 pagesNurs 65 Medical Surgical Nursing: Cavite State UniversityDennis Nyambane MomanyiNo ratings yet
- Nejmcp 2032396Document10 pagesNejmcp 2032396juan carlosNo ratings yet
- LBP 2Document12 pagesLBP 2Attika DiniNo ratings yet
- The Enciclopedia of The Back and Spine Systems and Disorders 2007 UCLADocument369 pagesThe Enciclopedia of The Back and Spine Systems and Disorders 2007 UCLAOana CristeaNo ratings yet
- Inflammatory Biomarkers of Low Back PainDocument17 pagesInflammatory Biomarkers of Low Back Painshivaprasad kolurNo ratings yet
- Algoritmo de Tratamiento para Dolor Secundario A Sindrome de Bertolotti 2024Document10 pagesAlgoritmo de Tratamiento para Dolor Secundario A Sindrome de Bertolotti 2024Oscar Cayetano Herrera RodríguezNo ratings yet
- Management L Low Back PainDocument7 pagesManagement L Low Back PainelsyamelindaNo ratings yet
- Koes2006 PDFDocument5 pagesKoes2006 PDFDewi FathmahNo ratings yet
- Padjadjaran University Medical SchoolDocument14 pagesPadjadjaran University Medical SchoolSelvi Puspa SariNo ratings yet
- Difficult Pain ProblemsDocument9 pagesDifficult Pain ProblemsRina WahyuniNo ratings yet
- Knee Oa NcbiDocument7 pagesKnee Oa NcbiFitria Dewi LestariNo ratings yet
- Lespasio Et Al 2017 Knee Osteoarthritis A PrimerDocument7 pagesLespasio Et Al 2017 Knee Osteoarthritis A PrimerMuhammad MuktiNo ratings yet
- Physiotherapy Management of Neck Pain: Arianne P VerhagenDocument7 pagesPhysiotherapy Management of Neck Pain: Arianne P VerhagenHari25885No ratings yet
- A 24-Year-Old Man With Suspected Sacroiliitis PDFDocument2 pagesA 24-Year-Old Man With Suspected Sacroiliitis PDFnertila dalaniNo ratings yet
- Advances in The Diagnosis & Management of Neck Pain - Article.Document19 pagesAdvances in The Diagnosis & Management of Neck Pain - Article.salmankhan09215No ratings yet
- 2018 - The Lancet 1 - Hartvigsen LBP PDFDocument12 pages2018 - The Lancet 1 - Hartvigsen LBP PDFLeslie Yuz AracenaNo ratings yet
- Nonspecific Low Back Pain: Clinical PracticeDocument9 pagesNonspecific Low Back Pain: Clinical PracticeandhikahadiNo ratings yet
- None 2Document9 pagesNone 2Alfina RahmiNo ratings yet
- Low Back PainDocument24 pagesLow Back PainAbraham SaldañaNo ratings yet
- Neck PDFDocument20 pagesNeck PDFManisha KarnaniNo ratings yet
- WhiplashInjury CEACCPDocument5 pagesWhiplashInjury CEACCPCarlosNo ratings yet
- Manual - of - Orthopaedics - (PG - 13 230)Document218 pagesManual - of - Orthopaedics - (PG - 13 230)2wk8cr7rmdNo ratings yet
- What Low Back Pain Is and Why We Need To Pay Attention: The Lancet March 2018Document13 pagesWhat Low Back Pain Is and Why We Need To Pay Attention: The Lancet March 2018Michael JunNo ratings yet
- Abnormal Spine CurvaturesDocument7 pagesAbnormal Spine CurvaturesMartin SageNo ratings yet
- Lumbar Radiculopathy Medback Castillo Mendez EDITEDDocument12 pagesLumbar Radiculopathy Medback Castillo Mendez EDITEDSteve ColbertNo ratings yet
- Back Pain ReliefDocument6 pagesBack Pain ReliefYuvraj SinghNo ratings yet
- Managing Low Back Pain in Primary Care: Chris G Maher, Director Chris Lin, Research FellowDocument5 pagesManaging Low Back Pain in Primary Care: Chris G Maher, Director Chris Lin, Research FellowPaulina ChangoNo ratings yet
- Jurnal Frozen PDFDocument27 pagesJurnal Frozen PDFFahmi MiNo ratings yet
- Hands On: Management of Shoulder Disorders in Primary CareDocument8 pagesHands On: Management of Shoulder Disorders in Primary CareCambriaChicoNo ratings yet
- Emergencia de Los Cuidados Paliativos en Un Hospital en UsaDocument4 pagesEmergencia de Los Cuidados Paliativos en Un Hospital en UsaIvan NuñezNo ratings yet
- 2011 Article 9218Document8 pages2011 Article 9218RenaldiPrimaSaputraNo ratings yet
- 2011 Article 9218 PDFDocument8 pages2011 Article 9218 PDFAgnesya GunawanNo ratings yet
- PSB 419Document7 pagesPSB 419Erick PrasetyaNo ratings yet
- Back Pain and Scoliosis in Children When To Image, What To ConsiderDocument12 pagesBack Pain and Scoliosis in Children When To Image, What To ConsiderGiancarlo PalaciosNo ratings yet
- The Effectiveness of Physiotherapeutic Interventions in Treatment of Frozen Shoulder Adhesive Capsulitis A Systematic ReviewDocument28 pagesThe Effectiveness of Physiotherapeutic Interventions in Treatment of Frozen Shoulder Adhesive Capsulitis A Systematic ReviewseetokindNo ratings yet
- Winzenberg, T. (2015) - Musculoskeletal Chest Wall Pain.Document5 pagesWinzenberg, T. (2015) - Musculoskeletal Chest Wall Pain.Tom StevensNo ratings yet
- Bland 1984Document28 pagesBland 1984Hellmann Adrian Escobar CNo ratings yet
- Cervical Spondylosis and Neck PainDocument5 pagesCervical Spondylosis and Neck PainIsaac AlemanNo ratings yet
- Avaliação Quadril PDFDocument10 pagesAvaliação Quadril PDFMarcus Dos SantosNo ratings yet
- 10.1515 - Jom 2021 0231Document8 pages10.1515 - Jom 2021 0231consueloamado.medNo ratings yet
- Jurnal 8 - 10.1191@1460408606ta357oaDocument18 pagesJurnal 8 - 10.1191@1460408606ta357oaAyu Novita KartikaningtyasNo ratings yet
- Chronic Mechanical LBPDocument7 pagesChronic Mechanical LBPMar'aa NurNo ratings yet
- Risk Factors Forchronic Low Back Pain 2161 0711.1000271Document4 pagesRisk Factors Forchronic Low Back Pain 2161 0711.100027155664411No ratings yet
- Chronic Back Pain 2006 Continuing Education in Anaesthesia Critical Care PDocument4 pagesChronic Back Pain 2006 Continuing Education in Anaesthesia Critical Care Pronaldquezada038No ratings yet
- Donald L. Renfrew, MD: Spine PainDocument16 pagesDonald L. Renfrew, MD: Spine PainalmiraerickaiNo ratings yet
- 266 Full PDFDocument7 pages266 Full PDFannisaNo ratings yet
- Cervical Radiculopathy and Cervical Myelopathy:: Clinical IntelligenceDocument3 pagesCervical Radiculopathy and Cervical Myelopathy:: Clinical IntelligenceCylla RevataNo ratings yet
- A Guide to Back Pain: Symptoms; Causes; Treatment; PreventionFrom EverandA Guide to Back Pain: Symptoms; Causes; Treatment; PreventionNo ratings yet
- Back Pain: Back Pain Treatment: Back Pain Relief: How To Heal Back ProblemsFrom EverandBack Pain: Back Pain Treatment: Back Pain Relief: How To Heal Back ProblemsNo ratings yet
- Pengantar RadiologiDocument40 pagesPengantar Radiologishrt gtNo ratings yet
- Acute Kidney Injury: Mohammad RudiansyahDocument80 pagesAcute Kidney Injury: Mohammad Rudiansyahshrt gtNo ratings yet
- Addiction To: DiazepamDocument21 pagesAddiction To: Diazepamshrt gtNo ratings yet
- An Overview of Indian Research in Anxiety Disorders: J. K. Trivedi, Pawan Kumar GuptaDocument9 pagesAn Overview of Indian Research in Anxiety Disorders: J. K. Trivedi, Pawan Kumar Guptashrt gtNo ratings yet
- Cauda Equina SyndromeDocument2 pagesCauda Equina Syndromeshrt gtNo ratings yet
- PEMERIKSAAN RADIOLOGI PADA GASTRITIS DAN ULKUS-edited2017Document51 pagesPEMERIKSAAN RADIOLOGI PADA GASTRITIS DAN ULKUS-edited2017shrt gtNo ratings yet
- Cauda Equina Syndrome: Innovait October 2011Document6 pagesCauda Equina Syndrome: Innovait October 2011shrt gtNo ratings yet
- Delayed Speech or Language DevelopmentDocument2 pagesDelayed Speech or Language Developmentshrt gtNo ratings yet
- Delay SpeechDocument8 pagesDelay Speechshrt gtNo ratings yet
- Cellulitis FactsDocument3 pagesCellulitis FactsCyril D. SuazoNo ratings yet
- Urine-Catherther-Insertion-And-Removal DocsDocument6 pagesUrine-Catherther-Insertion-And-Removal DocssrslytrdNo ratings yet
- FNCPDocument4 pagesFNCPChristian DaevinNo ratings yet
- Introduction To Abnormal Psychology Boundless PsychologyDocument17 pagesIntroduction To Abnormal Psychology Boundless PsychologySana NasirNo ratings yet
- ObjectivesDocument3 pagesObjectivesSicat Mark BantiyanNo ratings yet
- Metastasis 2Document28 pagesMetastasis 2RaNa MaYaaNo ratings yet
- Birmingham SquareDocument3 pagesBirmingham SquarefoxypandaNo ratings yet
- Taxim OFDocument13 pagesTaxim OFsarfaraz arzoo shaikhNo ratings yet
- Scorpion Envenomation Treatment & Management Prehospital Care, Emergency Department Care, Medical CareDocument12 pagesScorpion Envenomation Treatment & Management Prehospital Care, Emergency Department Care, Medical Carejoaoalmeida_1955No ratings yet
- Cardiopulmonary ResuscitationDocument10 pagesCardiopulmonary ResuscitationLilay MakulayNo ratings yet
- Canine Hypothyroidism, An OverviewDocument6 pagesCanine Hypothyroidism, An OverviewISABELSSBNo ratings yet
- SOMATOM Definition AS Open 20 64 RadOncol PDFDocument20 pagesSOMATOM Definition AS Open 20 64 RadOncol PDFJorge LopezNo ratings yet
- Cancer GeneticsDocument301 pagesCancer GeneticsNguyễn Tiến HồngNo ratings yet
- Test Bank For Mechanical Ventilation 7th Edition J M CairoDocument13 pagesTest Bank For Mechanical Ventilation 7th Edition J M CairocalliopesilasaagyNo ratings yet
- Nebivolol in HtaDocument16 pagesNebivolol in HtaCodruta Emanuela Maria VirsescuNo ratings yet
- uk-spc-nexium-sachet-10mg-DRESS-update-GI 21 0012aDocument17 pagesuk-spc-nexium-sachet-10mg-DRESS-update-GI 21 0012aDeisy ClerkeNo ratings yet
- Pendekatan Anak Saat Melakukan Perawatan GigiDocument17 pagesPendekatan Anak Saat Melakukan Perawatan Gigihelen mrbnNo ratings yet
- Clinical Practice Guideline For An Infection Controlexposure Control Program in The Oral Healthcare SettingDocument1 pageClinical Practice Guideline For An Infection Controlexposure Control Program in The Oral Healthcare Settingapi-399847495No ratings yet
- The Significance of Immunization in The Prevention of Childhood Killer DiseasesDocument69 pagesThe Significance of Immunization in The Prevention of Childhood Killer DiseasesUsman Ahmad Tijjani100% (1)
- Davao Doctors College Nursing Program Nursing Care PlanDocument3 pagesDavao Doctors College Nursing Program Nursing Care PlanPRINCESS KOBAYASHINo ratings yet
- BLUE & FALLS Protocol LichensteinDocument12 pagesBLUE & FALLS Protocol LichensteinCarlos MoncayoNo ratings yet
- ADHD and The BrainDocument1 pageADHD and The Brain111No ratings yet
- BA-BE Study Design and ProtocolDocument6 pagesBA-BE Study Design and ProtocolvarishNo ratings yet
- Advisory On The Opening of The Registration For The 2024 Cycle of The Ritm National External Quality Assessment Scheme FinalDocument2 pagesAdvisory On The Opening of The Registration For The 2024 Cycle of The Ritm National External Quality Assessment Scheme Finalgdh.lab2022No ratings yet
- Brochure DepressionDocument2 pagesBrochure Depressionel milanesasNo ratings yet
- Medical For Athletes 2..BOYS RODICADocument2 pagesMedical For Athletes 2..BOYS RODICADiana Rose Acupeado100% (1)
- Quick Sleep Tips For Truck DriversDocument2 pagesQuick Sleep Tips For Truck DriversBaye HickinsNo ratings yet
- CBSE NCERT Solutions For Class 12 Science Chapter 4: Back of Chapter QuestionsDocument5 pagesCBSE NCERT Solutions For Class 12 Science Chapter 4: Back of Chapter QuestionsSatvik MishraNo ratings yet
- Bulletin June2011Document6 pagesBulletin June2011Rema Panickar SugunanNo ratings yet
































































































Download as pdf or txt
You might also like
- Acute Ischemic Stroke Concept MapDocument6 pagesAcute Ischemic Stroke Concept MapMoonyeen Jann Casera Balic100% (2)
- Low Back Pain 2018Document18 pagesLow Back Pain 2018Salazar Ángel100% (1)
- 2.5 NotesDocument7 pages2.5 NotesKenneth MelchorNo ratings yet
- The Treatment of Neck and Upper Back Pain With AcuDocument6 pagesThe Treatment of Neck and Upper Back Pain With AcuMohmmad Hossein NazariNo ratings yet
- Evidence Based Physiotherapy Management of A Cervical Radiculopathy PatientDocument9 pagesEvidence Based Physiotherapy Management of A Cervical Radiculopathy PatientDr Abdallah BahaaNo ratings yet
- Interventions in Chronic Pain ManagementDocument4 pagesInterventions in Chronic Pain ManagementwladjaNo ratings yet
- Cleveland Clinic Journal of Medicine 2007 Klineberg 905 13Document9 pagesCleveland Clinic Journal of Medicine 2007 Klineberg 905 13Sohaib AliNo ratings yet
- Assessment and Management of Acute Low Back Pain - American Family PhysicianDocument9 pagesAssessment and Management of Acute Low Back Pain - American Family PhysiciancaralivroNo ratings yet
- Discogenic LBP Revised September 2017Document13 pagesDiscogenic LBP Revised September 2017Clinton Franda Markus SitanggangNo ratings yet
- Herniated Lumbar Intervertebral Disk: Epidemiology and Natural HistoryDocument6 pagesHerniated Lumbar Intervertebral Disk: Epidemiology and Natural HistoryGeysel SuarezNo ratings yet
- Advances in The Diagnosis and Management of Neck PainDocument19 pagesAdvances in The Diagnosis and Management of Neck PainJose Fernando DiezNo ratings yet
- Low Back Pain Guidelines-Reduced2Document26 pagesLow Back Pain Guidelines-Reduced2ranggadr100% (1)
- Nurs 65 Medical Surgical Nursing: Cavite State UniversityDocument14 pagesNurs 65 Medical Surgical Nursing: Cavite State UniversityDennis Nyambane MomanyiNo ratings yet
- Nejmcp 2032396Document10 pagesNejmcp 2032396juan carlosNo ratings yet
- LBP 2Document12 pagesLBP 2Attika DiniNo ratings yet
- The Enciclopedia of The Back and Spine Systems and Disorders 2007 UCLADocument369 pagesThe Enciclopedia of The Back and Spine Systems and Disorders 2007 UCLAOana CristeaNo ratings yet
- Inflammatory Biomarkers of Low Back PainDocument17 pagesInflammatory Biomarkers of Low Back Painshivaprasad kolurNo ratings yet
- Algoritmo de Tratamiento para Dolor Secundario A Sindrome de Bertolotti 2024Document10 pagesAlgoritmo de Tratamiento para Dolor Secundario A Sindrome de Bertolotti 2024Oscar Cayetano Herrera RodríguezNo ratings yet
- Management L Low Back PainDocument7 pagesManagement L Low Back PainelsyamelindaNo ratings yet
- Koes2006 PDFDocument5 pagesKoes2006 PDFDewi FathmahNo ratings yet
- Padjadjaran University Medical SchoolDocument14 pagesPadjadjaran University Medical SchoolSelvi Puspa SariNo ratings yet
- Difficult Pain ProblemsDocument9 pagesDifficult Pain ProblemsRina WahyuniNo ratings yet
- Knee Oa NcbiDocument7 pagesKnee Oa NcbiFitria Dewi LestariNo ratings yet
- Lespasio Et Al 2017 Knee Osteoarthritis A PrimerDocument7 pagesLespasio Et Al 2017 Knee Osteoarthritis A PrimerMuhammad MuktiNo ratings yet
- Physiotherapy Management of Neck Pain: Arianne P VerhagenDocument7 pagesPhysiotherapy Management of Neck Pain: Arianne P VerhagenHari25885No ratings yet
- A 24-Year-Old Man With Suspected Sacroiliitis PDFDocument2 pagesA 24-Year-Old Man With Suspected Sacroiliitis PDFnertila dalaniNo ratings yet
- Advances in The Diagnosis & Management of Neck Pain - Article.Document19 pagesAdvances in The Diagnosis & Management of Neck Pain - Article.salmankhan09215No ratings yet
- 2018 - The Lancet 1 - Hartvigsen LBP PDFDocument12 pages2018 - The Lancet 1 - Hartvigsen LBP PDFLeslie Yuz AracenaNo ratings yet
- Nonspecific Low Back Pain: Clinical PracticeDocument9 pagesNonspecific Low Back Pain: Clinical PracticeandhikahadiNo ratings yet
- None 2Document9 pagesNone 2Alfina RahmiNo ratings yet
- Low Back PainDocument24 pagesLow Back PainAbraham SaldañaNo ratings yet
- Neck PDFDocument20 pagesNeck PDFManisha KarnaniNo ratings yet
- WhiplashInjury CEACCPDocument5 pagesWhiplashInjury CEACCPCarlosNo ratings yet
- Manual - of - Orthopaedics - (PG - 13 230)Document218 pagesManual - of - Orthopaedics - (PG - 13 230)2wk8cr7rmdNo ratings yet
- What Low Back Pain Is and Why We Need To Pay Attention: The Lancet March 2018Document13 pagesWhat Low Back Pain Is and Why We Need To Pay Attention: The Lancet March 2018Michael JunNo ratings yet
- Abnormal Spine CurvaturesDocument7 pagesAbnormal Spine CurvaturesMartin SageNo ratings yet
- Lumbar Radiculopathy Medback Castillo Mendez EDITEDDocument12 pagesLumbar Radiculopathy Medback Castillo Mendez EDITEDSteve ColbertNo ratings yet
- Back Pain ReliefDocument6 pagesBack Pain ReliefYuvraj SinghNo ratings yet
- Managing Low Back Pain in Primary Care: Chris G Maher, Director Chris Lin, Research FellowDocument5 pagesManaging Low Back Pain in Primary Care: Chris G Maher, Director Chris Lin, Research FellowPaulina ChangoNo ratings yet
- Jurnal Frozen PDFDocument27 pagesJurnal Frozen PDFFahmi MiNo ratings yet
- Hands On: Management of Shoulder Disorders in Primary CareDocument8 pagesHands On: Management of Shoulder Disorders in Primary CareCambriaChicoNo ratings yet
- Emergencia de Los Cuidados Paliativos en Un Hospital en UsaDocument4 pagesEmergencia de Los Cuidados Paliativos en Un Hospital en UsaIvan NuñezNo ratings yet
- 2011 Article 9218Document8 pages2011 Article 9218RenaldiPrimaSaputraNo ratings yet
- 2011 Article 9218 PDFDocument8 pages2011 Article 9218 PDFAgnesya GunawanNo ratings yet
- PSB 419Document7 pagesPSB 419Erick PrasetyaNo ratings yet
- Back Pain and Scoliosis in Children When To Image, What To ConsiderDocument12 pagesBack Pain and Scoliosis in Children When To Image, What To ConsiderGiancarlo PalaciosNo ratings yet
- The Effectiveness of Physiotherapeutic Interventions in Treatment of Frozen Shoulder Adhesive Capsulitis A Systematic ReviewDocument28 pagesThe Effectiveness of Physiotherapeutic Interventions in Treatment of Frozen Shoulder Adhesive Capsulitis A Systematic ReviewseetokindNo ratings yet
- Winzenberg, T. (2015) - Musculoskeletal Chest Wall Pain.Document5 pagesWinzenberg, T. (2015) - Musculoskeletal Chest Wall Pain.Tom StevensNo ratings yet
- Bland 1984Document28 pagesBland 1984Hellmann Adrian Escobar CNo ratings yet
- Cervical Spondylosis and Neck PainDocument5 pagesCervical Spondylosis and Neck PainIsaac AlemanNo ratings yet
- Avaliação Quadril PDFDocument10 pagesAvaliação Quadril PDFMarcus Dos SantosNo ratings yet
- 10.1515 - Jom 2021 0231Document8 pages10.1515 - Jom 2021 0231consueloamado.medNo ratings yet
- Jurnal 8 - 10.1191@1460408606ta357oaDocument18 pagesJurnal 8 - 10.1191@1460408606ta357oaAyu Novita KartikaningtyasNo ratings yet
- Chronic Mechanical LBPDocument7 pagesChronic Mechanical LBPMar'aa NurNo ratings yet
- Risk Factors Forchronic Low Back Pain 2161 0711.1000271Document4 pagesRisk Factors Forchronic Low Back Pain 2161 0711.100027155664411No ratings yet
- Chronic Back Pain 2006 Continuing Education in Anaesthesia Critical Care PDocument4 pagesChronic Back Pain 2006 Continuing Education in Anaesthesia Critical Care Pronaldquezada038No ratings yet
- Donald L. Renfrew, MD: Spine PainDocument16 pagesDonald L. Renfrew, MD: Spine PainalmiraerickaiNo ratings yet
- 266 Full PDFDocument7 pages266 Full PDFannisaNo ratings yet
- Cervical Radiculopathy and Cervical Myelopathy:: Clinical IntelligenceDocument3 pagesCervical Radiculopathy and Cervical Myelopathy:: Clinical IntelligenceCylla RevataNo ratings yet
- A Guide to Back Pain: Symptoms; Causes; Treatment; PreventionFrom EverandA Guide to Back Pain: Symptoms; Causes; Treatment; PreventionNo ratings yet
- Back Pain: Back Pain Treatment: Back Pain Relief: How To Heal Back ProblemsFrom EverandBack Pain: Back Pain Treatment: Back Pain Relief: How To Heal Back ProblemsNo ratings yet
- Pengantar RadiologiDocument40 pagesPengantar Radiologishrt gtNo ratings yet
- Acute Kidney Injury: Mohammad RudiansyahDocument80 pagesAcute Kidney Injury: Mohammad Rudiansyahshrt gtNo ratings yet
- Addiction To: DiazepamDocument21 pagesAddiction To: Diazepamshrt gtNo ratings yet
- An Overview of Indian Research in Anxiety Disorders: J. K. Trivedi, Pawan Kumar GuptaDocument9 pagesAn Overview of Indian Research in Anxiety Disorders: J. K. Trivedi, Pawan Kumar Guptashrt gtNo ratings yet
- Cauda Equina SyndromeDocument2 pagesCauda Equina Syndromeshrt gtNo ratings yet
- PEMERIKSAAN RADIOLOGI PADA GASTRITIS DAN ULKUS-edited2017Document51 pagesPEMERIKSAAN RADIOLOGI PADA GASTRITIS DAN ULKUS-edited2017shrt gtNo ratings yet
- Cauda Equina Syndrome: Innovait October 2011Document6 pagesCauda Equina Syndrome: Innovait October 2011shrt gtNo ratings yet
- Delayed Speech or Language DevelopmentDocument2 pagesDelayed Speech or Language Developmentshrt gtNo ratings yet
- Delay SpeechDocument8 pagesDelay Speechshrt gtNo ratings yet
- Cellulitis FactsDocument3 pagesCellulitis FactsCyril D. SuazoNo ratings yet
- Urine-Catherther-Insertion-And-Removal DocsDocument6 pagesUrine-Catherther-Insertion-And-Removal DocssrslytrdNo ratings yet
- FNCPDocument4 pagesFNCPChristian DaevinNo ratings yet
- Introduction To Abnormal Psychology Boundless PsychologyDocument17 pagesIntroduction To Abnormal Psychology Boundless PsychologySana NasirNo ratings yet
- ObjectivesDocument3 pagesObjectivesSicat Mark BantiyanNo ratings yet
- Metastasis 2Document28 pagesMetastasis 2RaNa MaYaaNo ratings yet
- Birmingham SquareDocument3 pagesBirmingham SquarefoxypandaNo ratings yet
- Taxim OFDocument13 pagesTaxim OFsarfaraz arzoo shaikhNo ratings yet
- Scorpion Envenomation Treatment & Management Prehospital Care, Emergency Department Care, Medical CareDocument12 pagesScorpion Envenomation Treatment & Management Prehospital Care, Emergency Department Care, Medical Carejoaoalmeida_1955No ratings yet
- Cardiopulmonary ResuscitationDocument10 pagesCardiopulmonary ResuscitationLilay MakulayNo ratings yet
- Canine Hypothyroidism, An OverviewDocument6 pagesCanine Hypothyroidism, An OverviewISABELSSBNo ratings yet
- SOMATOM Definition AS Open 20 64 RadOncol PDFDocument20 pagesSOMATOM Definition AS Open 20 64 RadOncol PDFJorge LopezNo ratings yet
- Cancer GeneticsDocument301 pagesCancer GeneticsNguyễn Tiến HồngNo ratings yet
- Test Bank For Mechanical Ventilation 7th Edition J M CairoDocument13 pagesTest Bank For Mechanical Ventilation 7th Edition J M CairocalliopesilasaagyNo ratings yet
- Nebivolol in HtaDocument16 pagesNebivolol in HtaCodruta Emanuela Maria VirsescuNo ratings yet
- uk-spc-nexium-sachet-10mg-DRESS-update-GI 21 0012aDocument17 pagesuk-spc-nexium-sachet-10mg-DRESS-update-GI 21 0012aDeisy ClerkeNo ratings yet
- Pendekatan Anak Saat Melakukan Perawatan GigiDocument17 pagesPendekatan Anak Saat Melakukan Perawatan Gigihelen mrbnNo ratings yet
- Clinical Practice Guideline For An Infection Controlexposure Control Program in The Oral Healthcare SettingDocument1 pageClinical Practice Guideline For An Infection Controlexposure Control Program in The Oral Healthcare Settingapi-399847495No ratings yet
- The Significance of Immunization in The Prevention of Childhood Killer DiseasesDocument69 pagesThe Significance of Immunization in The Prevention of Childhood Killer DiseasesUsman Ahmad Tijjani100% (1)
- Davao Doctors College Nursing Program Nursing Care PlanDocument3 pagesDavao Doctors College Nursing Program Nursing Care PlanPRINCESS KOBAYASHINo ratings yet
- BLUE & FALLS Protocol LichensteinDocument12 pagesBLUE & FALLS Protocol LichensteinCarlos MoncayoNo ratings yet
- ADHD and The BrainDocument1 pageADHD and The Brain111No ratings yet
- BA-BE Study Design and ProtocolDocument6 pagesBA-BE Study Design and ProtocolvarishNo ratings yet
- Advisory On The Opening of The Registration For The 2024 Cycle of The Ritm National External Quality Assessment Scheme FinalDocument2 pagesAdvisory On The Opening of The Registration For The 2024 Cycle of The Ritm National External Quality Assessment Scheme Finalgdh.lab2022No ratings yet
- Brochure DepressionDocument2 pagesBrochure Depressionel milanesasNo ratings yet
- Medical For Athletes 2..BOYS RODICADocument2 pagesMedical For Athletes 2..BOYS RODICADiana Rose Acupeado100% (1)
- Quick Sleep Tips For Truck DriversDocument2 pagesQuick Sleep Tips For Truck DriversBaye HickinsNo ratings yet
- CBSE NCERT Solutions For Class 12 Science Chapter 4: Back of Chapter QuestionsDocument5 pagesCBSE NCERT Solutions For Class 12 Science Chapter 4: Back of Chapter QuestionsSatvik MishraNo ratings yet
- Bulletin June2011Document6 pagesBulletin June2011Rema Panickar SugunanNo ratings yet