Download as pdf or txt
You might also like
- CNL-500 Topic 6: Comparison WorksheetDocument6 pagesCNL-500 Topic 6: Comparison WorksheetDeekay100% (23)
- Isabel Clarke, Hazel Nicholls - Third Wave CBT Integration For Individuals and Teams - Comprehend, Cope and Connect (2017, Routledge)Document185 pagesIsabel Clarke, Hazel Nicholls - Third Wave CBT Integration For Individuals and Teams - Comprehend, Cope and Connect (2017, Routledge)Anna Thallita AraujoNo ratings yet
- Pulp Exposure in Permanent Teeth CG-A012-04 UpdatedDocument7 pagesPulp Exposure in Permanent Teeth CG-A012-04 UpdatedmahmoudNo ratings yet
- Violent Behaviour Assessment ScaleDocument2 pagesViolent Behaviour Assessment Scalejessicali717No ratings yet
- Community Pharmacy MedicationDocument11 pagesCommunity Pharmacy MedicationVander JuniorNo ratings yet
- Hummael (2010)Document6 pagesHummael (2010)dewiNo ratings yet
- Kalisch - The Impact of Teamwork On Missed - Nursing CareDocument9 pagesKalisch - The Impact of Teamwork On Missed - Nursing CarePutri NabillaNo ratings yet
- See Also Page 1013: ESS S OREDocument3 pagesSee Also Page 1013: ESS S ORESundas EjazNo ratings yet
- Translator Apr2010 Vo4 Iss1Document4 pagesTranslator Apr2010 Vo4 Iss1Vina Angga RiniNo ratings yet
- Arch Intern Med Medication Errors Observed in 36 Health Care Facilities 2002Document7 pagesArch Intern Med Medication Errors Observed in 36 Health Care Facilities 2002alejandromfunes1749No ratings yet
- Shaffer2017-Tutku MacBook ProDocument6 pagesShaffer2017-Tutku MacBook ProMEKSELINA KALENDERNo ratings yet
- Artigo 2Document13 pagesArtigo 2Paulo TononNo ratings yet
- Artikel Ebsco 3Document7 pagesArtikel Ebsco 3bakena bajentaNo ratings yet
- Medication Related Problems During Transfer From Hospital To Home Care: Baseline Data From SwitzerlandDocument7 pagesMedication Related Problems During Transfer From Hospital To Home Care: Baseline Data From SwitzerlandJorge Arturo Porras BermúdezNo ratings yet
- Reporting Medical Errors To Improve Patient Safety: A Survey of Physicians in Teaching HospitalsDocument7 pagesReporting Medical Errors To Improve Patient Safety: A Survey of Physicians in Teaching HospitalsDanily Faith VillarNo ratings yet
- Hayward EvaluationGenericScreens 1993Document10 pagesHayward EvaluationGenericScreens 1993Dauna Apriansa Anggoro PutriNo ratings yet
- Medication Errors in An Intensive Care Unit: OriginalresearchDocument10 pagesMedication Errors in An Intensive Care Unit: OriginalresearchFauziah AizulNo ratings yet
- Jorgensen 2017Document6 pagesJorgensen 2017jessicapxeNo ratings yet
- Selected Topics: Prehospital CareDocument9 pagesSelected Topics: Prehospital CareYo MeNo ratings yet
- The Effect of Guided Care TeamsDocument7 pagesThe Effect of Guided Care TeamsHuzi SidNo ratings yet
- Conciliação 005Document13 pagesConciliação 005Izabella WebberNo ratings yet
- Obstetric Referrals at Saint Paul'S Hospital Millennium Medical College (SPHMMC) : Pre-Referral Care and AppropriatenessDocument7 pagesObstetric Referrals at Saint Paul'S Hospital Millennium Medical College (SPHMMC) : Pre-Referral Care and AppropriatenessTaklu Marama M. BaatiiNo ratings yet
- Thirumagal 2017Document6 pagesThirumagal 2017Armando cortezNo ratings yet
- Ceschi 2021 Oi 210724 1631040648.26526Document13 pagesCeschi 2021 Oi 210724 1631040648.26526pymb6gt7jbNo ratings yet
- Emergency Physician Awareness of Prehospital ProceDocument8 pagesEmergency Physician Awareness of Prehospital ProceNines RíosNo ratings yet
- Nurse Perceptions of Medication ErrorsDocument9 pagesNurse Perceptions of Medication ErrorsMoisés PonceNo ratings yet
- Impact of An Integrated Medication Reconciliation ModelDocument8 pagesImpact of An Integrated Medication Reconciliation Modelprissyben17No ratings yet
- Ambulatory Prescribing Errors Among Community Based Providers in Two StatesDocument6 pagesAmbulatory Prescribing Errors Among Community Based Providers in Two StatesIsaura RubioNo ratings yet
- Factors Associated With 30-Day Readmission For Patients Hospitalized For SeizuresDocument10 pagesFactors Associated With 30-Day Readmission For Patients Hospitalized For SeizuresAndhika DNo ratings yet
- Adverse Event or Near-Miss Analysis (Nursing) .EditedDocument10 pagesAdverse Event or Near-Miss Analysis (Nursing) .EditedMaina PeterNo ratings yet
- Clinical Practice Guideline Safe Medication Use.32Document39 pagesClinical Practice Guideline Safe Medication Use.32Edward ZiyachechaNo ratings yet
- Computerized ProgramDocument7 pagesComputerized ProgramfatiisaadatNo ratings yet
- Nursing Practice Today: Behrouz Pakcheshm, Imane Bagheri Zohreh KalaniDocument9 pagesNursing Practice Today: Behrouz Pakcheshm, Imane Bagheri Zohreh KalaniFernando PintoNo ratings yet
- Medication Errors:: Don't Let Them Happen To YouDocument6 pagesMedication Errors:: Don't Let Them Happen To YouPhuong Tran100% (1)
- POTENTIAL DRUG INTERACTIONS IN INTENSIVE CARE PATIENTS AT A Teaching HospitalDocument6 pagesPOTENTIAL DRUG INTERACTIONS IN INTENSIVE CARE PATIENTS AT A Teaching HospitalJuwita RamadhaniNo ratings yet
- Pharmacy: Evolution of Interdisciplinary Transition of Care Services in A Primary Care OrganizationDocument6 pagesPharmacy: Evolution of Interdisciplinary Transition of Care Services in A Primary Care OrganizationMr XNo ratings yet
- Komunikasi Efektif Smith2014Document9 pagesKomunikasi Efektif Smith2014agstriansNo ratings yet
- Fernandes Medication Reconciliation Practical Tips Strategies and Tools For PharmacistsDocument10 pagesFernandes Medication Reconciliation Practical Tips Strategies and Tools For PharmacistsEvianti Dwi AgustinNo ratings yet
- RSP 48 02 0314Document8 pagesRSP 48 02 0314euandianaeuanNo ratings yet
- Kejadian Eror Medikasi Di Ruang ICU JurnalDocument11 pagesKejadian Eror Medikasi Di Ruang ICU JurnalindriNo ratings yet
- Effect of Automated Drug Distribution Systems On Medication Error Rates in A Short-Stay Geriatric UnitDocument7 pagesEffect of Automated Drug Distribution Systems On Medication Error Rates in A Short-Stay Geriatric Unitdinia fitrianiNo ratings yet
- 2000, Antonow J. Medication Error Reporting PediatriaDocument7 pages2000, Antonow J. Medication Error Reporting PediatriaFilipa Salvador SalvadorNo ratings yet
- AnnalsATS 201605-398OCDocument8 pagesAnnalsATS 201605-398OCRodrigoSachiFreitasNo ratings yet
- Appropriateness of Hospital Use by Family Physicians: ResultsDocument7 pagesAppropriateness of Hospital Use by Family Physicians: ResultsSurya WijayaNo ratings yet
- The Medication Reconciliation DilemmaDocument73 pagesThe Medication Reconciliation Dilemmaknive13No ratings yet
- The Relationship Between Early Emergency Team Calls and Serious Adverse EventsDocument13 pagesThe Relationship Between Early Emergency Team Calls and Serious Adverse Eventsririznurlaila123No ratings yet
- Improving Primary Care in Rural Alabama With A Pharmacy InitiativeDocument7 pagesImproving Primary Care in Rural Alabama With A Pharmacy InitiativeBasilharbi HammadNo ratings yet
- Pediatric Anesthesiology Fellows' Perception of Quality of Attending Supervision and Medical ErrorsDocument5 pagesPediatric Anesthesiology Fellows' Perception of Quality of Attending Supervision and Medical ErrorsGio VandaNo ratings yet
- Articulo NeumoniaDocument7 pagesArticulo NeumoniaEd BarajasNo ratings yet
- Lower Urinary TractDocument8 pagesLower Urinary TractMyisha UfairaNo ratings yet
- Pharmacy 07 00128 v2 PDFDocument8 pagesPharmacy 07 00128 v2 PDFMr XNo ratings yet
- Roughead 2016Document10 pagesRoughead 2016Armando cortezNo ratings yet
- ,adherence, 2008Document8 pages,adherence, 2008Abdurhman SeidNo ratings yet
- Challenges at Care Transitions: Failure To Follow Medication Changes Made at Hospital DischargeDocument14 pagesChallenges at Care Transitions: Failure To Follow Medication Changes Made at Hospital DischargePranvera ApostoliNo ratings yet
- Randomized Trial of An Education and Support Intervention To Prevent Readmission of Patients With Heart FailureDocument7 pagesRandomized Trial of An Education and Support Intervention To Prevent Readmission of Patients With Heart FailureThyka MayasariNo ratings yet
- 加拿大食道癌Document8 pages加拿大食道癌Joseph ChenNo ratings yet
- Er ReadingsDocument6 pagesEr ReadingsReginald UyNo ratings yet
- Artigo 02 - Bond & RaehlDocument13 pagesArtigo 02 - Bond & RaehlDeanzek WinchesterNo ratings yet
- Pandini Et Al., 2016Document6 pagesPandini Et Al., 2016mackenzie.lacey28No ratings yet
- What We Need To Know For Patient SafetyDocument9 pagesWhat We Need To Know For Patient SafetyhusainiNo ratings yet
- Maria Adorno Week 5 RUADocument6 pagesMaria Adorno Week 5 RUAMaria AdornoNo ratings yet
- The Maximally Efficient and Optimally Effective Emergency Department: One Good Thing A DayFrom EverandThe Maximally Efficient and Optimally Effective Emergency Department: One Good Thing A DayNo ratings yet
- Nurses Contributions to Quality Health OutcomesFrom EverandNurses Contributions to Quality Health OutcomesMarianne BaernholdtNo ratings yet
- Steroid Tapering and Supportive Treatment Guidance V1.0 PDFDocument1 pageSteroid Tapering and Supportive Treatment Guidance V1.0 PDFRiza Yulia RezkiNo ratings yet
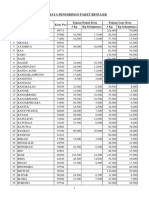
- Biaya Kirim Paket RegulerDocument9 pagesBiaya Kirim Paket RegulerRiza Yulia RezkiNo ratings yet
- Jurnal 2Document4 pagesJurnal 2Riza Yulia RezkiNo ratings yet
- Jurnal 1 PDFDocument8 pagesJurnal 1 PDFRiza Yulia RezkiNo ratings yet
- Massage Therapy Client Intake FormDocument4 pagesMassage Therapy Client Intake FormEverly Oballo100% (1)
- Module 4 MedicineDocument50 pagesModule 4 Medicinepjanu86No ratings yet
- Revised Extended DefinitionDocument7 pagesRevised Extended Definitionapi-458848708No ratings yet
- CancerConfidential PDFDocument158 pagesCancerConfidential PDFTiago CostaNo ratings yet
- Renal Function TestsDocument7 pagesRenal Function Testsiyuth dytiartiNo ratings yet
- Objection Handling With ConfidenceDocument3 pagesObjection Handling With ConfidenceAnup Soans100% (2)
- Good Practice Guidance 4. Expiry Dates For MedicationDocument5 pagesGood Practice Guidance 4. Expiry Dates For MedicationAgnieszka WaligóraNo ratings yet
- 23 TransplantationDocument15 pages23 TransplantationHaseeb IslamNo ratings yet
- Disease Control Priorities For Mental, Neurological and Substance Abuse Disorders 2015Document307 pagesDisease Control Priorities For Mental, Neurological and Substance Abuse Disorders 2015LunaFiaNo ratings yet
- ECHS Referral FormDocument17 pagesECHS Referral FormBrem AnandNo ratings yet
- Chronic Suppurative Otitis MediaDocument4 pagesChronic Suppurative Otitis MediarchristoverNo ratings yet
- Edema Pulmo Pada PreeklamsiDocument50 pagesEdema Pulmo Pada PreeklamsiZelly Mitia ZubirNo ratings yet
- Mood ChartDocument2 pagesMood ChartPsydocNo ratings yet
- Pi Is 0007091217439080Document8 pagesPi Is 0007091217439080Halim SudonoNo ratings yet
- Perspective: New England Journal MedicineDocument4 pagesPerspective: New England Journal MedicineTha Vila Le ColloNo ratings yet
- Kristin Gabrielsen - Treating Sensory Disability in Autism With QST Massage Decreases Severity of Autism: A Replication StudyDocument1 pageKristin Gabrielsen - Treating Sensory Disability in Autism With QST Massage Decreases Severity of Autism: A Replication StudyAUCDNo ratings yet
- What Is OsteoarthritisDocument12 pagesWhat Is OsteoarthritischicktankNo ratings yet
- Status Kalazion - Yoga 1161050136Document10 pagesStatus Kalazion - Yoga 1161050136Yoga WitularNo ratings yet
- Respiratory EmergencyDocument14 pagesRespiratory EmergencyThomas SentanuNo ratings yet
- Neurosurgery 4 Mental DisordersDocument82 pagesNeurosurgery 4 Mental DisordersTomChristianNo ratings yet
- Pace University End of Life Simulation State 2 Pain ManagementDocument4 pagesPace University End of Life Simulation State 2 Pain Managementapi-414017065No ratings yet
- Magnesium CitrateDocument3 pagesMagnesium CitrateMorticia AdamsNo ratings yet
- Care of New Traumatic SCI Patients in JamaicaDocument32 pagesCare of New Traumatic SCI Patients in JamaicaRory DixonNo ratings yet
- Dental Management of COPD Patient: SS Rahman1, M Faruque2, MHA Khan3, SA Hossain4Document3 pagesDental Management of COPD Patient: SS Rahman1, M Faruque2, MHA Khan3, SA Hossain4Shirmayne TangNo ratings yet
- Liverpool Ni Modi PineDocument5 pagesLiverpool Ni Modi Pinerachmat fajar noor kNo ratings yet
- Nursing Review Notes 2Document4 pagesNursing Review Notes 2api-3822508100% (5)