
Emergency Nursing Care Record
Emergency Nursing Care Record
You might also like
- Skin Assessment Form PDFDocument1 pageSkin Assessment Form PDFRHBeautyCareTambolakaNo ratings yet
- Diagnostic Criteria Examination Form PDFDocument2 pagesDiagnostic Criteria Examination Form PDFNor Nadia Zakaria50% (2)
- Patient Encounter FormDocument2 pagesPatient Encounter FormSpectator Medic0% (1)
- 5-Hole 1/4 1 3/8 C-To-C: Anesthesia RecordDocument10 pages5-Hole 1/4 1 3/8 C-To-C: Anesthesia RecordMohammed100% (2)
- SSC Coo RRPP..CC Oom M: Ssa Am MPP LleeDocument2 pagesSSC Coo RRPP..CC Oom M: Ssa Am MPP LleeEkaSaktiWahyuningtyasNo ratings yet
- Organizational WorksheetDocument4 pagesOrganizational WorksheetJennifer AprilNo ratings yet
- Bedside Shift ReportDocument3 pagesBedside Shift ReportRumkee chyNo ratings yet
- TraumaDocument4 pagesTraumaDra. Carol Angélica Artigas GómezNo ratings yet
- TradeEvaluationWorksheet CalendarSpread - 2010 02 20Document1 pageTradeEvaluationWorksheet CalendarSpread - 2010 02 20InvestmentguybNo ratings yet
- Surgical Safety Checklist 1Document1 pageSurgical Safety Checklist 1rhod_bspt3251No ratings yet
- Who Surgery ChecklistDocument2 pagesWho Surgery ChecklistcalyxelNo ratings yet
- A Smart Plan For A Healthier Life: Presenting Manipalcigna Prohealth Insurance With Added FeaturesDocument2 pagesA Smart Plan For A Healthier Life: Presenting Manipalcigna Prohealth Insurance With Added FeaturesMana PlanetNo ratings yet
- Night BeforeDocument3 pagesNight BeforeChris MoffettNo ratings yet
- Non-Neonatal Tetanus: (ICD 10 Code: A35)Document2 pagesNon-Neonatal Tetanus: (ICD 10 Code: A35)CHICKY100% (1)
- Internal Medicine HISTORYDocument4 pagesInternal Medicine HISTORYNorjetalexis CabreraNo ratings yet
- Fitness TestDocument2 pagesFitness TestWordzone DpsNo ratings yet
- 2018-04-09 Pediatric Emergency Nursing Assessment Record FormDocument2 pages2018-04-09 Pediatric Emergency Nursing Assessment Record FormHengkyNo ratings yet
- T HRD 025 Leave Form NEWDocument1 pageT HRD 025 Leave Form NEWMarshall james G. RamirezNo ratings yet
- Ketikkan Emergency HostDocument2 pagesKetikkan Emergency HostBella ApNo ratings yet
- Internal Medicine HISTORYDocument4 pagesInternal Medicine HISTORYClaire FNo ratings yet
- Physical Examination - Equine 2pg VersionDocument2 pagesPhysical Examination - Equine 2pg VersionvetthamilNo ratings yet
- Contact Tracing FormDocument2 pagesContact Tracing FormDyrom TorioNo ratings yet
- 2020 MedicalCertificateCombativeDocument1 page2020 MedicalCertificateCombativejefferson pabloNo ratings yet
- Isbar FormDocument1 pageIsbar FormChandrasreeNo ratings yet
- Ficha Bunga, Inquebrantavel-Coração-de-Ferro PDFDocument4 pagesFicha Bunga, Inquebrantavel-Coração-de-Ferro PDFNinho do CondorNo ratings yet
- Medical For Athletes 1Document2 pagesMedical For Athletes 1Patrick RodriguezNo ratings yet
- Physicalexam Score SheetDocument2 pagesPhysicalexam Score SheetMarieCrisNo ratings yet
- Medical For Athletes 1Document1 pageMedical For Athletes 1marlou john lacdaoNo ratings yet
- Teriandror, Filho de Teriadrin - OuADocument2 pagesTeriandror, Filho de Teriadrin - OuACarlos SantanaNo ratings yet
- CRT 7Document8 pagesCRT 7api-643868511No ratings yet
- Confidential Patient Information: C L C CDocument6 pagesConfidential Patient Information: C L C CPedroNo ratings yet
- Speech Therapy Evaluation Guideline For Orofacial Motor Skills 2016Document11 pagesSpeech Therapy Evaluation Guideline For Orofacial Motor Skills 2016ScribdTranslationsNo ratings yet
- Nursing Report 1Document1 pageNursing Report 1Saved ANo ratings yet
- 2020 MedicalCertificate (Combative)Document1 page2020 MedicalCertificate (Combative)Dennmark IgutNo ratings yet
- Chap 01Document36 pagesChap 01neonsrmiNo ratings yet
- LenghwiseDocument2 pagesLenghwiseAnna Margarett Mutia CaballarNo ratings yet
- IBE, Susanna Martha B. 2014-57561 Ward 1Document4 pagesIBE, Susanna Martha B. 2014-57561 Ward 1WazzupNo ratings yet
- Medication HistoryDocument2 pagesMedication HistoryShona EtheringtonNo ratings yet
- ExaltedvsWoD 2-Page InteractiveDocument2 pagesExaltedvsWoD 2-Page InteractiveJosh smithNo ratings yet
- IMP - OuADocument2 pagesIMP - OuACarlos SantanaNo ratings yet
- Iii. Physical Assessment and Review of SystemDocument7 pagesIii. Physical Assessment and Review of SystemBiya MacunteNo ratings yet
- Katharina SchwarzDocument2 pagesKatharina SchwarzAnonymous qGdZVLNo ratings yet
- Medical For Athletes ASGDocument1 pageMedical For Athletes ASGJanette BolanteNo ratings yet
- Home Health Solutions Group Home Companion Services: Nursing Assessment Form - RecertificationDocument5 pagesHome Health Solutions Group Home Companion Services: Nursing Assessment Form - RecertificationCitra Puspita SariNo ratings yet
- Patient Assessment Form: Assess Scene Secondary SurveyDocument2 pagesPatient Assessment Form: Assess Scene Secondary Surveydeepeezee_beenNo ratings yet
- Orthodontics DiagnosisDocument26 pagesOrthodontics DiagnosisMu'taz ArmanNo ratings yet
- Acute Abdomen WorkbookDocument11 pagesAcute Abdomen WorkbookFarid AkbarNo ratings yet
- Unscheduled Visit - SynAct-CS002Document11 pagesUnscheduled Visit - SynAct-CS002adriana gutanuNo ratings yet
- Daily Expense FormDocument1 pageDaily Expense Formwintwah.myantestNo ratings yet
- List - Manuevers SwordsageDocument3 pagesList - Manuevers SwordsageAaron SumnersNo ratings yet
- Hasil Pemeriksaan Kesehatan: I. General Data / Data PribadiDocument3 pagesHasil Pemeriksaan Kesehatan: I. General Data / Data PribadiAoeliaZulkarneinNo ratings yet
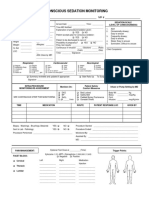
- 34 An Consious Sedation MonitoringDocument2 pages34 An Consious Sedation Monitoringabu alauon abed almohsenNo ratings yet
- Nursing Report Sheet - Nursing Report SheetDocument1 pageNursing Report Sheet - Nursing Report SheetSaved ANo ratings yet
- Traits - : Anão Das Montanhas Solitárias RicoDocument2 pagesTraits - : Anão Das Montanhas Solitárias RicoCarlos SantanaNo ratings yet
- Damage Resistance: Condition Condition Condition Condition Condition Condition Condition Condition Condition ConditionDocument1 pageDamage Resistance: Condition Condition Condition Condition Condition Condition Condition Condition Condition Conditionvaly playNo ratings yet
- Circulating Nurse ChecklistDocument2 pagesCirculating Nurse ChecklistOne Click Online ShopNo ratings yet
- Birth History/Parent Concerns Physical Examination (Unclothed)Document3 pagesBirth History/Parent Concerns Physical Examination (Unclothed)brian@coombsmd.comNo ratings yet
- Assigment Problem 2Document5 pagesAssigment Problem 2William Y. OspinaNo ratings yet
- The MelancholicDocument5 pagesThe MelancholicJohn Albert LogoNo ratings yet
- CDCP - 02.28.11 - Titration Excel PracticeDocument2 pagesCDCP - 02.28.11 - Titration Excel PracticeSeleneblueNo ratings yet
- Latihan Soal Cls 8 ADocument3 pagesLatihan Soal Cls 8 AJamal UdinNo ratings yet
- Quantitative Historical Linguistics A Corpus Framework (Oxford Studies in Diachronic and Historical Linguistics)Document247 pagesQuantitative Historical Linguistics A Corpus Framework (Oxford Studies in Diachronic and Historical Linguistics)ChristianNo ratings yet
- (J. A Short) Drilling A Source Book On Oil and Ga PDFDocument588 pages(J. A Short) Drilling A Source Book On Oil and Ga PDFZana Qadir100% (1)
- Taboo Cards - RemovedDocument7 pagesTaboo Cards - RemovedArthur FariasNo ratings yet
- MR NobodyDocument1 pageMR NobodyCatalina PricopeNo ratings yet
- Epidemiologi, Pathogenesis, Diagnosis DM, BPJS 2015Document35 pagesEpidemiologi, Pathogenesis, Diagnosis DM, BPJS 2015Samuel Albert Andrian SiagianNo ratings yet
- Food Biotechnology Sports NutritionDocument14 pagesFood Biotechnology Sports NutritionAngelo PalmeroNo ratings yet
- Fairchild V.glenhaven Funeral Services LTDDocument9 pagesFairchild V.glenhaven Funeral Services LTDSwastik SinghNo ratings yet
- Wishonttari Vedic PredictionDocument7 pagesWishonttari Vedic PredictionSelvaraj RangasamyNo ratings yet
- Principles 1Document13 pagesPrinciples 1RicaNo ratings yet
- Recommendation Letter Thesis Supervisor SampleDocument6 pagesRecommendation Letter Thesis Supervisor Sampleafknjdsta100% (2)
- Statistics Chapter 10-12Document11 pagesStatistics Chapter 10-12Alna Gamulo LosaNo ratings yet
- LUTHERAN Gregorian Psalter and Canticles Matins Vespers 1897Document488 pagesLUTHERAN Gregorian Psalter and Canticles Matins Vespers 1897Peter Brandt-SorheimNo ratings yet
- Resume Physics Faculty Latur PDFDocument2 pagesResume Physics Faculty Latur PDFDishaNo ratings yet
- "Deep" Learning For Missing Value Imputation in Tables With Non-Numerical DataDocument9 pages"Deep" Learning For Missing Value Imputation in Tables With Non-Numerical DataRamon LopesNo ratings yet
- Solution Manual For Calculus 1st Edition by Briggs and CochranDocument34 pagesSolution Manual For Calculus 1st Edition by Briggs and Cochranstree.brooklet1wue7u100% (48)
- Blom and Another V Brown and Others - 2011 - 3 All SA 223 - SCADocument7 pagesBlom and Another V Brown and Others - 2011 - 3 All SA 223 - SCAtoritNo ratings yet
- Auto-Reclose On Distribution NetworksDocument57 pagesAuto-Reclose On Distribution NetworksNeelakandan MasilamaniNo ratings yet
- Like Father Like SonDocument8 pagesLike Father Like Sonnisemononamae7990No ratings yet
- Amniotic Membrane in Oral and Maxillofacial SurgeryDocument13 pagesAmniotic Membrane in Oral and Maxillofacial SurgerySooraj SNo ratings yet
- Struktur Organisasi: Kabupaten GorontaloDocument3 pagesStruktur Organisasi: Kabupaten GorontaloMohamad TaufanNo ratings yet
- The Obsidian Dagger Being The Further Extraordinary Adventures of Horatio Lyle Number 2 in Series by Catherine Webb (Webb, Catherine)Document289 pagesThe Obsidian Dagger Being The Further Extraordinary Adventures of Horatio Lyle Number 2 in Series by Catherine Webb (Webb, Catherine)Hitha MathewNo ratings yet
- Lymphoproliferative DiseasesDocument8 pagesLymphoproliferative DiseasesRegla Mailyn Perez PerezNo ratings yet
- ZNKR Seitei Iaido PDFDocument46 pagesZNKR Seitei Iaido PDFaldemararaujo100% (2)
- DR - Hala ExpansionTypesinArabic FinalDocument40 pagesDR - Hala ExpansionTypesinArabic FinalWaleed OthmanNo ratings yet
- Adriyanmahmoudi 168hourassignmentDocument3 pagesAdriyanmahmoudi 168hourassignmentapi-528485357No ratings yet
- A Quiet Day: July 25thDocument20 pagesA Quiet Day: July 25thЛюбовь МароваNo ratings yet





















































































Download as pdf or txt
You might also like
- Skin Assessment Form PDFDocument1 pageSkin Assessment Form PDFRHBeautyCareTambolakaNo ratings yet
- Diagnostic Criteria Examination Form PDFDocument2 pagesDiagnostic Criteria Examination Form PDFNor Nadia Zakaria50% (2)
- Patient Encounter FormDocument2 pagesPatient Encounter FormSpectator Medic0% (1)
- 5-Hole 1/4 1 3/8 C-To-C: Anesthesia RecordDocument10 pages5-Hole 1/4 1 3/8 C-To-C: Anesthesia RecordMohammed100% (2)
- SSC Coo RRPP..CC Oom M: Ssa Am MPP LleeDocument2 pagesSSC Coo RRPP..CC Oom M: Ssa Am MPP LleeEkaSaktiWahyuningtyasNo ratings yet
- Organizational WorksheetDocument4 pagesOrganizational WorksheetJennifer AprilNo ratings yet
- Bedside Shift ReportDocument3 pagesBedside Shift ReportRumkee chyNo ratings yet
- TraumaDocument4 pagesTraumaDra. Carol Angélica Artigas GómezNo ratings yet
- TradeEvaluationWorksheet CalendarSpread - 2010 02 20Document1 pageTradeEvaluationWorksheet CalendarSpread - 2010 02 20InvestmentguybNo ratings yet
- Surgical Safety Checklist 1Document1 pageSurgical Safety Checklist 1rhod_bspt3251No ratings yet
- Who Surgery ChecklistDocument2 pagesWho Surgery ChecklistcalyxelNo ratings yet
- A Smart Plan For A Healthier Life: Presenting Manipalcigna Prohealth Insurance With Added FeaturesDocument2 pagesA Smart Plan For A Healthier Life: Presenting Manipalcigna Prohealth Insurance With Added FeaturesMana PlanetNo ratings yet
- Night BeforeDocument3 pagesNight BeforeChris MoffettNo ratings yet
- Non-Neonatal Tetanus: (ICD 10 Code: A35)Document2 pagesNon-Neonatal Tetanus: (ICD 10 Code: A35)CHICKY100% (1)
- Internal Medicine HISTORYDocument4 pagesInternal Medicine HISTORYNorjetalexis CabreraNo ratings yet
- Fitness TestDocument2 pagesFitness TestWordzone DpsNo ratings yet
- 2018-04-09 Pediatric Emergency Nursing Assessment Record FormDocument2 pages2018-04-09 Pediatric Emergency Nursing Assessment Record FormHengkyNo ratings yet
- T HRD 025 Leave Form NEWDocument1 pageT HRD 025 Leave Form NEWMarshall james G. RamirezNo ratings yet
- Ketikkan Emergency HostDocument2 pagesKetikkan Emergency HostBella ApNo ratings yet
- Internal Medicine HISTORYDocument4 pagesInternal Medicine HISTORYClaire FNo ratings yet
- Physical Examination - Equine 2pg VersionDocument2 pagesPhysical Examination - Equine 2pg VersionvetthamilNo ratings yet
- Contact Tracing FormDocument2 pagesContact Tracing FormDyrom TorioNo ratings yet
- 2020 MedicalCertificateCombativeDocument1 page2020 MedicalCertificateCombativejefferson pabloNo ratings yet
- Isbar FormDocument1 pageIsbar FormChandrasreeNo ratings yet
- Ficha Bunga, Inquebrantavel-Coração-de-Ferro PDFDocument4 pagesFicha Bunga, Inquebrantavel-Coração-de-Ferro PDFNinho do CondorNo ratings yet
- Medical For Athletes 1Document2 pagesMedical For Athletes 1Patrick RodriguezNo ratings yet
- Physicalexam Score SheetDocument2 pagesPhysicalexam Score SheetMarieCrisNo ratings yet
- Medical For Athletes 1Document1 pageMedical For Athletes 1marlou john lacdaoNo ratings yet
- Teriandror, Filho de Teriadrin - OuADocument2 pagesTeriandror, Filho de Teriadrin - OuACarlos SantanaNo ratings yet
- CRT 7Document8 pagesCRT 7api-643868511No ratings yet
- Confidential Patient Information: C L C CDocument6 pagesConfidential Patient Information: C L C CPedroNo ratings yet
- Speech Therapy Evaluation Guideline For Orofacial Motor Skills 2016Document11 pagesSpeech Therapy Evaluation Guideline For Orofacial Motor Skills 2016ScribdTranslationsNo ratings yet
- Nursing Report 1Document1 pageNursing Report 1Saved ANo ratings yet
- 2020 MedicalCertificate (Combative)Document1 page2020 MedicalCertificate (Combative)Dennmark IgutNo ratings yet
- Chap 01Document36 pagesChap 01neonsrmiNo ratings yet
- LenghwiseDocument2 pagesLenghwiseAnna Margarett Mutia CaballarNo ratings yet
- IBE, Susanna Martha B. 2014-57561 Ward 1Document4 pagesIBE, Susanna Martha B. 2014-57561 Ward 1WazzupNo ratings yet
- Medication HistoryDocument2 pagesMedication HistoryShona EtheringtonNo ratings yet
- ExaltedvsWoD 2-Page InteractiveDocument2 pagesExaltedvsWoD 2-Page InteractiveJosh smithNo ratings yet
- IMP - OuADocument2 pagesIMP - OuACarlos SantanaNo ratings yet
- Iii. Physical Assessment and Review of SystemDocument7 pagesIii. Physical Assessment and Review of SystemBiya MacunteNo ratings yet
- Katharina SchwarzDocument2 pagesKatharina SchwarzAnonymous qGdZVLNo ratings yet
- Medical For Athletes ASGDocument1 pageMedical For Athletes ASGJanette BolanteNo ratings yet
- Home Health Solutions Group Home Companion Services: Nursing Assessment Form - RecertificationDocument5 pagesHome Health Solutions Group Home Companion Services: Nursing Assessment Form - RecertificationCitra Puspita SariNo ratings yet
- Patient Assessment Form: Assess Scene Secondary SurveyDocument2 pagesPatient Assessment Form: Assess Scene Secondary Surveydeepeezee_beenNo ratings yet
- Orthodontics DiagnosisDocument26 pagesOrthodontics DiagnosisMu'taz ArmanNo ratings yet
- Acute Abdomen WorkbookDocument11 pagesAcute Abdomen WorkbookFarid AkbarNo ratings yet
- Unscheduled Visit - SynAct-CS002Document11 pagesUnscheduled Visit - SynAct-CS002adriana gutanuNo ratings yet
- Daily Expense FormDocument1 pageDaily Expense Formwintwah.myantestNo ratings yet
- List - Manuevers SwordsageDocument3 pagesList - Manuevers SwordsageAaron SumnersNo ratings yet
- Hasil Pemeriksaan Kesehatan: I. General Data / Data PribadiDocument3 pagesHasil Pemeriksaan Kesehatan: I. General Data / Data PribadiAoeliaZulkarneinNo ratings yet
- 34 An Consious Sedation MonitoringDocument2 pages34 An Consious Sedation Monitoringabu alauon abed almohsenNo ratings yet
- Nursing Report Sheet - Nursing Report SheetDocument1 pageNursing Report Sheet - Nursing Report SheetSaved ANo ratings yet
- Traits - : Anão Das Montanhas Solitárias RicoDocument2 pagesTraits - : Anão Das Montanhas Solitárias RicoCarlos SantanaNo ratings yet
- Damage Resistance: Condition Condition Condition Condition Condition Condition Condition Condition Condition ConditionDocument1 pageDamage Resistance: Condition Condition Condition Condition Condition Condition Condition Condition Condition Conditionvaly playNo ratings yet
- Circulating Nurse ChecklistDocument2 pagesCirculating Nurse ChecklistOne Click Online ShopNo ratings yet
- Birth History/Parent Concerns Physical Examination (Unclothed)Document3 pagesBirth History/Parent Concerns Physical Examination (Unclothed)brian@coombsmd.comNo ratings yet
- Assigment Problem 2Document5 pagesAssigment Problem 2William Y. OspinaNo ratings yet
- The MelancholicDocument5 pagesThe MelancholicJohn Albert LogoNo ratings yet
- CDCP - 02.28.11 - Titration Excel PracticeDocument2 pagesCDCP - 02.28.11 - Titration Excel PracticeSeleneblueNo ratings yet
- Latihan Soal Cls 8 ADocument3 pagesLatihan Soal Cls 8 AJamal UdinNo ratings yet
- Quantitative Historical Linguistics A Corpus Framework (Oxford Studies in Diachronic and Historical Linguistics)Document247 pagesQuantitative Historical Linguistics A Corpus Framework (Oxford Studies in Diachronic and Historical Linguistics)ChristianNo ratings yet
- (J. A Short) Drilling A Source Book On Oil and Ga PDFDocument588 pages(J. A Short) Drilling A Source Book On Oil and Ga PDFZana Qadir100% (1)
- Taboo Cards - RemovedDocument7 pagesTaboo Cards - RemovedArthur FariasNo ratings yet
- MR NobodyDocument1 pageMR NobodyCatalina PricopeNo ratings yet
- Epidemiologi, Pathogenesis, Diagnosis DM, BPJS 2015Document35 pagesEpidemiologi, Pathogenesis, Diagnosis DM, BPJS 2015Samuel Albert Andrian SiagianNo ratings yet
- Food Biotechnology Sports NutritionDocument14 pagesFood Biotechnology Sports NutritionAngelo PalmeroNo ratings yet
- Fairchild V.glenhaven Funeral Services LTDDocument9 pagesFairchild V.glenhaven Funeral Services LTDSwastik SinghNo ratings yet
- Wishonttari Vedic PredictionDocument7 pagesWishonttari Vedic PredictionSelvaraj RangasamyNo ratings yet
- Principles 1Document13 pagesPrinciples 1RicaNo ratings yet
- Recommendation Letter Thesis Supervisor SampleDocument6 pagesRecommendation Letter Thesis Supervisor Sampleafknjdsta100% (2)
- Statistics Chapter 10-12Document11 pagesStatistics Chapter 10-12Alna Gamulo LosaNo ratings yet
- LUTHERAN Gregorian Psalter and Canticles Matins Vespers 1897Document488 pagesLUTHERAN Gregorian Psalter and Canticles Matins Vespers 1897Peter Brandt-SorheimNo ratings yet
- Resume Physics Faculty Latur PDFDocument2 pagesResume Physics Faculty Latur PDFDishaNo ratings yet
- "Deep" Learning For Missing Value Imputation in Tables With Non-Numerical DataDocument9 pages"Deep" Learning For Missing Value Imputation in Tables With Non-Numerical DataRamon LopesNo ratings yet
- Solution Manual For Calculus 1st Edition by Briggs and CochranDocument34 pagesSolution Manual For Calculus 1st Edition by Briggs and Cochranstree.brooklet1wue7u100% (48)
- Blom and Another V Brown and Others - 2011 - 3 All SA 223 - SCADocument7 pagesBlom and Another V Brown and Others - 2011 - 3 All SA 223 - SCAtoritNo ratings yet
- Auto-Reclose On Distribution NetworksDocument57 pagesAuto-Reclose On Distribution NetworksNeelakandan MasilamaniNo ratings yet
- Like Father Like SonDocument8 pagesLike Father Like Sonnisemononamae7990No ratings yet
- Amniotic Membrane in Oral and Maxillofacial SurgeryDocument13 pagesAmniotic Membrane in Oral and Maxillofacial SurgerySooraj SNo ratings yet
- Struktur Organisasi: Kabupaten GorontaloDocument3 pagesStruktur Organisasi: Kabupaten GorontaloMohamad TaufanNo ratings yet
- The Obsidian Dagger Being The Further Extraordinary Adventures of Horatio Lyle Number 2 in Series by Catherine Webb (Webb, Catherine)Document289 pagesThe Obsidian Dagger Being The Further Extraordinary Adventures of Horatio Lyle Number 2 in Series by Catherine Webb (Webb, Catherine)Hitha MathewNo ratings yet
- Lymphoproliferative DiseasesDocument8 pagesLymphoproliferative DiseasesRegla Mailyn Perez PerezNo ratings yet
- ZNKR Seitei Iaido PDFDocument46 pagesZNKR Seitei Iaido PDFaldemararaujo100% (2)
- DR - Hala ExpansionTypesinArabic FinalDocument40 pagesDR - Hala ExpansionTypesinArabic FinalWaleed OthmanNo ratings yet
- Adriyanmahmoudi 168hourassignmentDocument3 pagesAdriyanmahmoudi 168hourassignmentapi-528485357No ratings yet
- A Quiet Day: July 25thDocument20 pagesA Quiet Day: July 25thЛюбовь МароваNo ratings yet