
Jurnal
Jurnal
You might also like
- Biopharmaceutics Answer Key-BLUE PACOPDocument48 pagesBiopharmaceutics Answer Key-BLUE PACOPChengD100% (5)
- Ectopic PregnancyDocument26 pagesEctopic PregnancyCHryz TinNo ratings yet
- Possible Cardiac Chest Pain Clinical Pathway: FacilityDocument2 pagesPossible Cardiac Chest Pain Clinical Pathway: Facilityshofiyuddin100% (1)
- Epidural HematomaDocument33 pagesEpidural HematomaRupak GhimireNo ratings yet
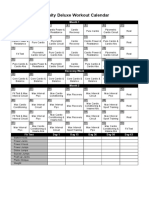
- Insanity Workout Deluxe Calendar SimpleDocument1 pageInsanity Workout Deluxe Calendar SimpleAnonymous sTnEkqy4No ratings yet
- Pelvic Floor Muscle TrainingDocument15 pagesPelvic Floor Muscle TrainingAne SoutoNo ratings yet
- Narrative Review of Pelvic Floor Muscle Training For Childbearing Women-Why, When, What, and HowDocument12 pagesNarrative Review of Pelvic Floor Muscle Training For Childbearing Women-Why, When, What, and HowLéa Cinthia Silva do NascimentoNo ratings yet
- Presentation 3Document34 pagesPresentation 3Chidube UkachukwuNo ratings yet
- Paula Exercise Method of Post-Fistula Repair IncontinenceDocument9 pagesPaula Exercise Method of Post-Fistula Repair IncontinenceLawal Isa UsmanNo ratings yet
- Abstract CHOICES OF NATIVE TISSUE REPAIRDocument2 pagesAbstract CHOICES OF NATIVE TISSUE REPAIRanton suponoNo ratings yet
- Hemorroid Shin2015Document9 pagesHemorroid Shin2015agusNo ratings yet
- BJON 2015 24 11 PelvicFloorUrology2Document5 pagesBJON 2015 24 11 PelvicFloorUrology2alonsosduranNo ratings yet
- RPMS in UIDocument13 pagesRPMS in UImageshNo ratings yet
- Update On Physiotherapy in Postpartum Urinary Incontinence. A Systematic ReviewDocument11 pagesUpdate On Physiotherapy in Postpartum Urinary Incontinence. A Systematic Reviewjake.leneNo ratings yet
- Stress Urinary Incontinence in Relation To Pelvic Floor Muscle StrengthDocument10 pagesStress Urinary Incontinence in Relation To Pelvic Floor Muscle StrengthNoraNo ratings yet
- Diastasis Recti in Pregnancy and Postpartum Period PDFDocument9 pagesDiastasis Recti in Pregnancy and Postpartum Period PDFIchim AmellyaNo ratings yet
- LP Post Partum SpontanDocument16 pagesLP Post Partum SpontanPutri PuspitaNo ratings yet
- Trastornos Del Suelo PélvicoDocument35 pagesTrastornos Del Suelo Pélvicodr.antoniogaonaNo ratings yet
- Effect of Kinesio Tape On Low Back Pain During Normal LaborDocument28 pagesEffect of Kinesio Tape On Low Back Pain During Normal Laborj_______________j100% (3)
- Prolonged Labor Incidences: Passage-Passenger Factors Analyzed (Descriptive Study in RSUD Dr. Koesma Tuban)Document5 pagesProlonged Labor Incidences: Passage-Passenger Factors Analyzed (Descriptive Study in RSUD Dr. Koesma Tuban)siska tiaraNo ratings yet
- Caesarean DeliveryDocument207 pagesCaesarean Deliverynsaid007No ratings yet
- Dismenorea and EndometriosisDocument4 pagesDismenorea and EndometriosispolygoneNo ratings yet
- Jbeim 21 394Document15 pagesJbeim 21 394Chloe BujuoirNo ratings yet
- 1 s2.0 S0002937823021166 MainDocument18 pages1 s2.0 S0002937823021166 MainAmin AminiNo ratings yet
- Clinical Study of Rupture Uterus - Assessment of Maternal and Fetal OutcomeDocument7 pagesClinical Study of Rupture Uterus - Assessment of Maternal and Fetal OutcomeIOSRjournalNo ratings yet
- 2016 Article 162 PDFDocument8 pages2016 Article 162 PDFefanNo ratings yet
- Retained Placenta After Vaginal Birth and Length of The Third Stage of Labor - UpToDateDocument19 pagesRetained Placenta After Vaginal Birth and Length of The Third Stage of Labor - UpToDateHartanto Lie100% (1)
- LASMARIAS IndivAct5Document25 pagesLASMARIAS IndivAct5AngelicaJaneA.SuanNo ratings yet
- UntitledDocument22 pagesUntitledAnurag DwivediNo ratings yet
- Abnormal Uterine Bleeding in Perimenopausal WomenDocument15 pagesAbnormal Uterine Bleeding in Perimenopausal WomenOrchid LandNo ratings yet
- Postoperative Peritoneal Adhesions in Adults and Their Prevention - UpToDateDocument17 pagesPostoperative Peritoneal Adhesions in Adults and Their Prevention - UpToDateDesak PramestiNo ratings yet
- Massage PerineumDocument13 pagesMassage PerineumGladys AilingNo ratings yet
- Therapeutic Potential of Mechanical Protection of Pelvic Floor During PregnancyDocument4 pagesTherapeutic Potential of Mechanical Protection of Pelvic Floor During PregnancyALfuNo ratings yet
- 1 s2.0 S183695532100014X MainDocument8 pages1 s2.0 S183695532100014X MainMetin HakkanNo ratings yet
- Uterine Prolapse: Clinical ReviewDocument5 pagesUterine Prolapse: Clinical ReviewPuannita SariNo ratings yet
- Poor Spontaneous and Oxytocin-Stimulated Contractility in Human Myometrium From Postdates PregnanciesDocument11 pagesPoor Spontaneous and Oxytocin-Stimulated Contractility in Human Myometrium From Postdates PregnanciesLauren RenNo ratings yet
- Pelvic Floor DysfunctionDocument4 pagesPelvic Floor Dysfunctionmyy.iphone1No ratings yet
- Uterine Prolapse: Presented By-Pooja Soni MSC Final Year Student Department of Obstetrics & GynecologyDocument39 pagesUterine Prolapse: Presented By-Pooja Soni MSC Final Year Student Department of Obstetrics & Gynecologyannu panchalNo ratings yet
- Ultrasonido en Infertilidad CapituloDocument20 pagesUltrasonido en Infertilidad CapituloVFJulianNo ratings yet
- Constipation in PregnancyDocument10 pagesConstipation in PregnancyMichimichi 78No ratings yet
- Abnormal Labor/Dystocia: Dystocia (Antonym Eutocia Greek: Tokos "Childbirth") Is An Abnormal orDocument12 pagesAbnormal Labor/Dystocia: Dystocia (Antonym Eutocia Greek: Tokos "Childbirth") Is An Abnormal ordinapurpleloversNo ratings yet
- NsaikilaDocument14 pagesNsaikilaayafor eric pekwalekeNo ratings yet
- Physiological Pathways and Molecular Mechanisms Regulating Uterine ContractilityDocument20 pagesPhysiological Pathways and Molecular Mechanisms Regulating Uterine ContractilityAchmad Ageng SeloNo ratings yet
- Exercise and Urinary Incontinence in WomeDocument5 pagesExercise and Urinary Incontinence in WomeKaren Itzel BlancarteNo ratings yet
- Acog Prolapso de Organos Pelvicos PDFDocument17 pagesAcog Prolapso de Organos Pelvicos PDFAnghelino Jesus Meza CentenoNo ratings yet
- Prevalence, Risk Factor, Pathophisiology of Sui: Dr. Budi Iman Santoso, Spog (K)Document11 pagesPrevalence, Risk Factor, Pathophisiology of Sui: Dr. Budi Iman Santoso, Spog (K)Komang TriwiramaNo ratings yet
- Diagnosis of Preterm Labor and Overview of Preterm BirthDocument15 pagesDiagnosis of Preterm Labor and Overview of Preterm BirthKenny IncsNo ratings yet
- Manual Therapy: Hsiu-Chuan Hung, Sheng-Mou Hsiao, Shu-Yun Chih, Ho-Hsiung Lin, Jau-Yih TsauoDocument7 pagesManual Therapy: Hsiu-Chuan Hung, Sheng-Mou Hsiao, Shu-Yun Chih, Ho-Hsiung Lin, Jau-Yih TsauoSara AguiarNo ratings yet
- La Longitud Vaginal: Análisis MultivarianteDocument42 pagesLa Longitud Vaginal: Análisis Multivariantedr.antoniogaonaNo ratings yet
- Menopause Part 1Document28 pagesMenopause Part 1Sanchita PandeyNo ratings yet
- ACOG 2019 Interim Update On POPDocument17 pagesACOG 2019 Interim Update On POPHaimanotNo ratings yet
- Jurnal Rupture Perineum 2Document9 pagesJurnal Rupture Perineum 2Muh AqwilNo ratings yet
- 10.1007@s00192 020 04302 8Document11 pages10.1007@s00192 020 04302 8Catur WulandariNo ratings yet
- Ectopic Pregnancy - StatPearls - NCBI BookshelfDocument6 pagesEctopic Pregnancy - StatPearls - NCBI BookshelfLaura valentina ramos mezaNo ratings yet
- Uterus KontaksiDocument13 pagesUterus KontaksiSuci SinagaNo ratings yet
- 2015 TJOG. Should We Add Unilateral Sacrospinous Ligament Fixation To Vaginal Hysterectomy in Management of Stage 3 and Stage 4 Pelvic Organ ProlapseDocument7 pages2015 TJOG. Should We Add Unilateral Sacrospinous Ligament Fixation To Vaginal Hysterectomy in Management of Stage 3 and Stage 4 Pelvic Organ ProlapseJoseTeodomiroQuispeRicciNo ratings yet
- The Myometrium: From Excitation To Contractions and Labour: Susan Wray and Clodagh PrendergastDocument31 pagesThe Myometrium: From Excitation To Contractions and Labour: Susan Wray and Clodagh PrendergastMBMNo ratings yet
- 10 Urogynecologic Problems in Pregnancy and Puerpurium TOG 2022Document9 pages10 Urogynecologic Problems in Pregnancy and Puerpurium TOG 2022Anna JuniedNo ratings yet
- Postpartum Stress Urinary Incontinance - Lessons From Animal ModelsDocument22 pagesPostpartum Stress Urinary Incontinance - Lessons From Animal ModelsinayahsyNo ratings yet
- Cervical and Vaginal Agenesis - A Rare Case ReportDocument5 pagesCervical and Vaginal Agenesis - A Rare Case ReportEditor_IAIMNo ratings yet
- Vaginal Vault ProlapseDocument9 pagesVaginal Vault ProlapseOanaNo ratings yet
- Print 1 FixDocument10 pagesPrint 1 Fixafriskha bulawanNo ratings yet
- Clinical Management of Bowel Endometriosis: From Diagnosis to TreatmentFrom EverandClinical Management of Bowel Endometriosis: From Diagnosis to TreatmentSimone FerreroNo ratings yet
- Psychiatric Nursing - Psycho PharmacologyDocument50 pagesPsychiatric Nursing - Psycho PharmacologyKaren MichelleNo ratings yet
- Disaster Mental Health Services: A Guidebook For Clinicians and AdministratorsDocument185 pagesDisaster Mental Health Services: A Guidebook For Clinicians and Administratorsnisabyan fansNo ratings yet
- Nursing NCP For Client With SchizophreniaDocument3 pagesNursing NCP For Client With Schizophreniaericjake_limNo ratings yet
- Emotion Release ChiroDocument12 pagesEmotion Release ChiroEurico GonçalvesNo ratings yet
- Or A SealDocument7 pagesOr A SealNo BoundariesNo ratings yet
- CV - NMCDocument2 pagesCV - NMCMav0% (1)
- Simplification of Referral System Under CGHS (Jan 2018)Document3 pagesSimplification of Referral System Under CGHS (Jan 2018)KALPUSHNo ratings yet
- By Mayo Clinic Staff: DiarrheaDocument6 pagesBy Mayo Clinic Staff: DiarrheaJamelyn GongoraNo ratings yet
- NCP BSN 3rd Yr Psychiatric WardDocument9 pagesNCP BSN 3rd Yr Psychiatric WardMary Margarett BoadoNo ratings yet
- Pharmacy Service Agreement PDFDocument164 pagesPharmacy Service Agreement PDFAnna YepNo ratings yet
- Nature's Pathways July 2014 Issue - Southeast WI EditionDocument60 pagesNature's Pathways July 2014 Issue - Southeast WI EditionNature's Pathways100% (1)
- Ortho Notes For New HODocument13 pagesOrtho Notes For New HORaja EllysyaNo ratings yet
- Pleural Effusion: PathophysiologyDocument6 pagesPleural Effusion: PathophysiologyNyamburaNo ratings yet
- Thermal BurnsDocument50 pagesThermal BurnsPooya WindyNo ratings yet
- Caton Et Al-2018-Journal of Clinical PeriodontologyDocument8 pagesCaton Et Al-2018-Journal of Clinical PeriodontologyWirajulay Pratiwi SanusiNo ratings yet
- CPG Recommendations For Patient Safety and Minimal Monitoring Standards During Anaesthesia and Recovery PDFDocument21 pagesCPG Recommendations For Patient Safety and Minimal Monitoring Standards During Anaesthesia and Recovery PDFDzarrinNo ratings yet
- Feridas Difícil CicatrizaçãoDocument22 pagesFeridas Difícil CicatrizaçãoBia BerzotiNo ratings yet
- Activities of Daily LivingDocument29 pagesActivities of Daily LivingAsraa MaryamNo ratings yet
- Role of UdvertanaDocument2 pagesRole of UdvertanaShamika Parab-KadamNo ratings yet
- Intravenous Vitamin CDocument3 pagesIntravenous Vitamin CnormaNo ratings yet
- Case WorkDocument2 pagesCase WorkDr.Laxmi PutranNo ratings yet
- Strategic PlanDocument84 pagesStrategic PlanAurutchat VichaiditNo ratings yet
- NCP Case PresDocument5 pagesNCP Case Pressyd19No ratings yet
- Journal of Anxiety Disorders: Penggunaan Realitas Virtual Dalam Penelitian Dan Penatalaksanaan AkrofobiaDocument13 pagesJournal of Anxiety Disorders: Penggunaan Realitas Virtual Dalam Penelitian Dan Penatalaksanaan AkrofobiaHerni Mariati RanganNo ratings yet
- Nephrology DR ZeinabDocument101 pagesNephrology DR ZeinabZeinab Muhammad100% (1)























































































Download as pdf or txt
You might also like
- Biopharmaceutics Answer Key-BLUE PACOPDocument48 pagesBiopharmaceutics Answer Key-BLUE PACOPChengD100% (5)
- Ectopic PregnancyDocument26 pagesEctopic PregnancyCHryz TinNo ratings yet
- Possible Cardiac Chest Pain Clinical Pathway: FacilityDocument2 pagesPossible Cardiac Chest Pain Clinical Pathway: Facilityshofiyuddin100% (1)
- Epidural HematomaDocument33 pagesEpidural HematomaRupak GhimireNo ratings yet
- Insanity Workout Deluxe Calendar SimpleDocument1 pageInsanity Workout Deluxe Calendar SimpleAnonymous sTnEkqy4No ratings yet
- Pelvic Floor Muscle TrainingDocument15 pagesPelvic Floor Muscle TrainingAne SoutoNo ratings yet
- Narrative Review of Pelvic Floor Muscle Training For Childbearing Women-Why, When, What, and HowDocument12 pagesNarrative Review of Pelvic Floor Muscle Training For Childbearing Women-Why, When, What, and HowLéa Cinthia Silva do NascimentoNo ratings yet
- Presentation 3Document34 pagesPresentation 3Chidube UkachukwuNo ratings yet
- Paula Exercise Method of Post-Fistula Repair IncontinenceDocument9 pagesPaula Exercise Method of Post-Fistula Repair IncontinenceLawal Isa UsmanNo ratings yet
- Abstract CHOICES OF NATIVE TISSUE REPAIRDocument2 pagesAbstract CHOICES OF NATIVE TISSUE REPAIRanton suponoNo ratings yet
- Hemorroid Shin2015Document9 pagesHemorroid Shin2015agusNo ratings yet
- BJON 2015 24 11 PelvicFloorUrology2Document5 pagesBJON 2015 24 11 PelvicFloorUrology2alonsosduranNo ratings yet
- RPMS in UIDocument13 pagesRPMS in UImageshNo ratings yet
- Update On Physiotherapy in Postpartum Urinary Incontinence. A Systematic ReviewDocument11 pagesUpdate On Physiotherapy in Postpartum Urinary Incontinence. A Systematic Reviewjake.leneNo ratings yet
- Stress Urinary Incontinence in Relation To Pelvic Floor Muscle StrengthDocument10 pagesStress Urinary Incontinence in Relation To Pelvic Floor Muscle StrengthNoraNo ratings yet
- Diastasis Recti in Pregnancy and Postpartum Period PDFDocument9 pagesDiastasis Recti in Pregnancy and Postpartum Period PDFIchim AmellyaNo ratings yet
- LP Post Partum SpontanDocument16 pagesLP Post Partum SpontanPutri PuspitaNo ratings yet
- Trastornos Del Suelo PélvicoDocument35 pagesTrastornos Del Suelo Pélvicodr.antoniogaonaNo ratings yet
- Effect of Kinesio Tape On Low Back Pain During Normal LaborDocument28 pagesEffect of Kinesio Tape On Low Back Pain During Normal Laborj_______________j100% (3)
- Prolonged Labor Incidences: Passage-Passenger Factors Analyzed (Descriptive Study in RSUD Dr. Koesma Tuban)Document5 pagesProlonged Labor Incidences: Passage-Passenger Factors Analyzed (Descriptive Study in RSUD Dr. Koesma Tuban)siska tiaraNo ratings yet
- Caesarean DeliveryDocument207 pagesCaesarean Deliverynsaid007No ratings yet
- Dismenorea and EndometriosisDocument4 pagesDismenorea and EndometriosispolygoneNo ratings yet
- Jbeim 21 394Document15 pagesJbeim 21 394Chloe BujuoirNo ratings yet
- 1 s2.0 S0002937823021166 MainDocument18 pages1 s2.0 S0002937823021166 MainAmin AminiNo ratings yet
- Clinical Study of Rupture Uterus - Assessment of Maternal and Fetal OutcomeDocument7 pagesClinical Study of Rupture Uterus - Assessment of Maternal and Fetal OutcomeIOSRjournalNo ratings yet
- 2016 Article 162 PDFDocument8 pages2016 Article 162 PDFefanNo ratings yet
- Retained Placenta After Vaginal Birth and Length of The Third Stage of Labor - UpToDateDocument19 pagesRetained Placenta After Vaginal Birth and Length of The Third Stage of Labor - UpToDateHartanto Lie100% (1)
- LASMARIAS IndivAct5Document25 pagesLASMARIAS IndivAct5AngelicaJaneA.SuanNo ratings yet
- UntitledDocument22 pagesUntitledAnurag DwivediNo ratings yet
- Abnormal Uterine Bleeding in Perimenopausal WomenDocument15 pagesAbnormal Uterine Bleeding in Perimenopausal WomenOrchid LandNo ratings yet
- Postoperative Peritoneal Adhesions in Adults and Their Prevention - UpToDateDocument17 pagesPostoperative Peritoneal Adhesions in Adults and Their Prevention - UpToDateDesak PramestiNo ratings yet
- Massage PerineumDocument13 pagesMassage PerineumGladys AilingNo ratings yet
- Therapeutic Potential of Mechanical Protection of Pelvic Floor During PregnancyDocument4 pagesTherapeutic Potential of Mechanical Protection of Pelvic Floor During PregnancyALfuNo ratings yet
- 1 s2.0 S183695532100014X MainDocument8 pages1 s2.0 S183695532100014X MainMetin HakkanNo ratings yet
- Uterine Prolapse: Clinical ReviewDocument5 pagesUterine Prolapse: Clinical ReviewPuannita SariNo ratings yet
- Poor Spontaneous and Oxytocin-Stimulated Contractility in Human Myometrium From Postdates PregnanciesDocument11 pagesPoor Spontaneous and Oxytocin-Stimulated Contractility in Human Myometrium From Postdates PregnanciesLauren RenNo ratings yet
- Pelvic Floor DysfunctionDocument4 pagesPelvic Floor Dysfunctionmyy.iphone1No ratings yet
- Uterine Prolapse: Presented By-Pooja Soni MSC Final Year Student Department of Obstetrics & GynecologyDocument39 pagesUterine Prolapse: Presented By-Pooja Soni MSC Final Year Student Department of Obstetrics & Gynecologyannu panchalNo ratings yet
- Ultrasonido en Infertilidad CapituloDocument20 pagesUltrasonido en Infertilidad CapituloVFJulianNo ratings yet
- Constipation in PregnancyDocument10 pagesConstipation in PregnancyMichimichi 78No ratings yet
- Abnormal Labor/Dystocia: Dystocia (Antonym Eutocia Greek: Tokos "Childbirth") Is An Abnormal orDocument12 pagesAbnormal Labor/Dystocia: Dystocia (Antonym Eutocia Greek: Tokos "Childbirth") Is An Abnormal ordinapurpleloversNo ratings yet
- NsaikilaDocument14 pagesNsaikilaayafor eric pekwalekeNo ratings yet
- Physiological Pathways and Molecular Mechanisms Regulating Uterine ContractilityDocument20 pagesPhysiological Pathways and Molecular Mechanisms Regulating Uterine ContractilityAchmad Ageng SeloNo ratings yet
- Exercise and Urinary Incontinence in WomeDocument5 pagesExercise and Urinary Incontinence in WomeKaren Itzel BlancarteNo ratings yet
- Acog Prolapso de Organos Pelvicos PDFDocument17 pagesAcog Prolapso de Organos Pelvicos PDFAnghelino Jesus Meza CentenoNo ratings yet
- Prevalence, Risk Factor, Pathophisiology of Sui: Dr. Budi Iman Santoso, Spog (K)Document11 pagesPrevalence, Risk Factor, Pathophisiology of Sui: Dr. Budi Iman Santoso, Spog (K)Komang TriwiramaNo ratings yet
- Diagnosis of Preterm Labor and Overview of Preterm BirthDocument15 pagesDiagnosis of Preterm Labor and Overview of Preterm BirthKenny IncsNo ratings yet
- Manual Therapy: Hsiu-Chuan Hung, Sheng-Mou Hsiao, Shu-Yun Chih, Ho-Hsiung Lin, Jau-Yih TsauoDocument7 pagesManual Therapy: Hsiu-Chuan Hung, Sheng-Mou Hsiao, Shu-Yun Chih, Ho-Hsiung Lin, Jau-Yih TsauoSara AguiarNo ratings yet
- La Longitud Vaginal: Análisis MultivarianteDocument42 pagesLa Longitud Vaginal: Análisis Multivariantedr.antoniogaonaNo ratings yet
- Menopause Part 1Document28 pagesMenopause Part 1Sanchita PandeyNo ratings yet
- ACOG 2019 Interim Update On POPDocument17 pagesACOG 2019 Interim Update On POPHaimanotNo ratings yet
- Jurnal Rupture Perineum 2Document9 pagesJurnal Rupture Perineum 2Muh AqwilNo ratings yet
- 10.1007@s00192 020 04302 8Document11 pages10.1007@s00192 020 04302 8Catur WulandariNo ratings yet
- Ectopic Pregnancy - StatPearls - NCBI BookshelfDocument6 pagesEctopic Pregnancy - StatPearls - NCBI BookshelfLaura valentina ramos mezaNo ratings yet
- Uterus KontaksiDocument13 pagesUterus KontaksiSuci SinagaNo ratings yet
- 2015 TJOG. Should We Add Unilateral Sacrospinous Ligament Fixation To Vaginal Hysterectomy in Management of Stage 3 and Stage 4 Pelvic Organ ProlapseDocument7 pages2015 TJOG. Should We Add Unilateral Sacrospinous Ligament Fixation To Vaginal Hysterectomy in Management of Stage 3 and Stage 4 Pelvic Organ ProlapseJoseTeodomiroQuispeRicciNo ratings yet
- The Myometrium: From Excitation To Contractions and Labour: Susan Wray and Clodagh PrendergastDocument31 pagesThe Myometrium: From Excitation To Contractions and Labour: Susan Wray and Clodagh PrendergastMBMNo ratings yet
- 10 Urogynecologic Problems in Pregnancy and Puerpurium TOG 2022Document9 pages10 Urogynecologic Problems in Pregnancy and Puerpurium TOG 2022Anna JuniedNo ratings yet
- Postpartum Stress Urinary Incontinance - Lessons From Animal ModelsDocument22 pagesPostpartum Stress Urinary Incontinance - Lessons From Animal ModelsinayahsyNo ratings yet
- Cervical and Vaginal Agenesis - A Rare Case ReportDocument5 pagesCervical and Vaginal Agenesis - A Rare Case ReportEditor_IAIMNo ratings yet
- Vaginal Vault ProlapseDocument9 pagesVaginal Vault ProlapseOanaNo ratings yet
- Print 1 FixDocument10 pagesPrint 1 Fixafriskha bulawanNo ratings yet
- Clinical Management of Bowel Endometriosis: From Diagnosis to TreatmentFrom EverandClinical Management of Bowel Endometriosis: From Diagnosis to TreatmentSimone FerreroNo ratings yet
- Psychiatric Nursing - Psycho PharmacologyDocument50 pagesPsychiatric Nursing - Psycho PharmacologyKaren MichelleNo ratings yet
- Disaster Mental Health Services: A Guidebook For Clinicians and AdministratorsDocument185 pagesDisaster Mental Health Services: A Guidebook For Clinicians and Administratorsnisabyan fansNo ratings yet
- Nursing NCP For Client With SchizophreniaDocument3 pagesNursing NCP For Client With Schizophreniaericjake_limNo ratings yet
- Emotion Release ChiroDocument12 pagesEmotion Release ChiroEurico GonçalvesNo ratings yet
- Or A SealDocument7 pagesOr A SealNo BoundariesNo ratings yet
- CV - NMCDocument2 pagesCV - NMCMav0% (1)
- Simplification of Referral System Under CGHS (Jan 2018)Document3 pagesSimplification of Referral System Under CGHS (Jan 2018)KALPUSHNo ratings yet
- By Mayo Clinic Staff: DiarrheaDocument6 pagesBy Mayo Clinic Staff: DiarrheaJamelyn GongoraNo ratings yet
- NCP BSN 3rd Yr Psychiatric WardDocument9 pagesNCP BSN 3rd Yr Psychiatric WardMary Margarett BoadoNo ratings yet
- Pharmacy Service Agreement PDFDocument164 pagesPharmacy Service Agreement PDFAnna YepNo ratings yet
- Nature's Pathways July 2014 Issue - Southeast WI EditionDocument60 pagesNature's Pathways July 2014 Issue - Southeast WI EditionNature's Pathways100% (1)
- Ortho Notes For New HODocument13 pagesOrtho Notes For New HORaja EllysyaNo ratings yet
- Pleural Effusion: PathophysiologyDocument6 pagesPleural Effusion: PathophysiologyNyamburaNo ratings yet
- Thermal BurnsDocument50 pagesThermal BurnsPooya WindyNo ratings yet
- Caton Et Al-2018-Journal of Clinical PeriodontologyDocument8 pagesCaton Et Al-2018-Journal of Clinical PeriodontologyWirajulay Pratiwi SanusiNo ratings yet
- CPG Recommendations For Patient Safety and Minimal Monitoring Standards During Anaesthesia and Recovery PDFDocument21 pagesCPG Recommendations For Patient Safety and Minimal Monitoring Standards During Anaesthesia and Recovery PDFDzarrinNo ratings yet
- Feridas Difícil CicatrizaçãoDocument22 pagesFeridas Difícil CicatrizaçãoBia BerzotiNo ratings yet
- Activities of Daily LivingDocument29 pagesActivities of Daily LivingAsraa MaryamNo ratings yet
- Role of UdvertanaDocument2 pagesRole of UdvertanaShamika Parab-KadamNo ratings yet
- Intravenous Vitamin CDocument3 pagesIntravenous Vitamin CnormaNo ratings yet
- Case WorkDocument2 pagesCase WorkDr.Laxmi PutranNo ratings yet
- Strategic PlanDocument84 pagesStrategic PlanAurutchat VichaiditNo ratings yet
- NCP Case PresDocument5 pagesNCP Case Pressyd19No ratings yet
- Journal of Anxiety Disorders: Penggunaan Realitas Virtual Dalam Penelitian Dan Penatalaksanaan AkrofobiaDocument13 pagesJournal of Anxiety Disorders: Penggunaan Realitas Virtual Dalam Penelitian Dan Penatalaksanaan AkrofobiaHerni Mariati RanganNo ratings yet
- Nephrology DR ZeinabDocument101 pagesNephrology DR ZeinabZeinab Muhammad100% (1)