Download as pdf or txt
You might also like
- Park Ranger Training PackDocument10 pagesPark Ranger Training PackSantiago Luengo FernandezNo ratings yet
- Research ProposalDocument23 pagesResearch ProposalNwaefuna Ekene86% (7)
- Malaria Updatemar 2019Document4 pagesMalaria Updatemar 2019Priya SahNo ratings yet
- Background/Situational AnalysisDocument7 pagesBackground/Situational AnalysisSimon DzokotoNo ratings yet
- Malaria in IndiaDocument5 pagesMalaria in IndiaRanveer Raj BhatnagarNo ratings yet
- 2017 Article 2875Document7 pages2017 Article 2875IFan Erian KurniawanNo ratings yet
- Uganda NATIONAL MALARIA CONTROL POLICY - 2011Document19 pagesUganda NATIONAL MALARIA CONTROL POLICY - 2011KASADHA PATRICKNo ratings yet
- Guidelines Malaria Di MalaysiaDocument61 pagesGuidelines Malaria Di MalaysianalmifaNo ratings yet
- Treatment Failure of Malaria Control in PakistanDocument26 pagesTreatment Failure of Malaria Control in Pakistandr_hammadNo ratings yet
- 1 MalariaDocument17 pages1 Malariasunita gurungNo ratings yet
- Evaluationa Vivaks LembataDocument10 pagesEvaluationa Vivaks Lembatamichael biaNo ratings yet
- 217170-Article Text-534583-1-10-20211109Document8 pages217170-Article Text-534583-1-10-20211109SMA N 1 TOROHNo ratings yet
- Novel Plasmodium Falciparum k13 Gene Polymorphisms From Kisii County, Kenya During An Era of Artemisinin-Based Combination Therapy DeploymentDocument13 pagesNovel Plasmodium Falciparum k13 Gene Polymorphisms From Kisii County, Kenya During An Era of Artemisinin-Based Combination Therapy DeploymentDian DamNo ratings yet
- EPI.2006.Unger - Tmih.can Malaria Be Controlled Where Basic Health Services Are Not UsedDocument9 pagesEPI.2006.Unger - Tmih.can Malaria Be Controlled Where Basic Health Services Are Not UsedderekwwillisNo ratings yet
- Guidelines South African Guidelines For The Prevention of Malaria 2017 Final - zp135472Document43 pagesGuidelines South African Guidelines For The Prevention of Malaria 2017 Final - zp135472Sudhakar Kuppireddy100% (1)
- Framework To Implement The Global Technical Strategy For Malaria 2016 - 2030 in The African RegionDocument22 pagesFramework To Implement The Global Technical Strategy For Malaria 2016 - 2030 in The African RegionPhilip TosinNo ratings yet
- 2011 National Policy On Diagnosis and Treatment of MalariaDocument34 pages2011 National Policy On Diagnosis and Treatment of MalarianoblefxNo ratings yet
- Vector Borne Disease Control Programme: Department of Public Health, Ministry of HealthDocument10 pagesVector Borne Disease Control Programme: Department of Public Health, Ministry of HealthSathish KumarNo ratings yet
- Malaria - (Still) A Global Health PriorityDocument1 pageMalaria - (Still) A Global Health PriorityErika OliveiraNo ratings yet
- Evaluation of Malaria Surveillance System in NigeriaDocument14 pagesEvaluation of Malaria Surveillance System in NigeriaMamadou CoulibalyNo ratings yet
- Evarle - Module Exam 1 - STSDocument6 pagesEvarle - Module Exam 1 - STSJeaness EvarleNo ratings yet
- Malaria 4Document16 pagesMalaria 4Andres RomeroNo ratings yet
- Yemen - Anti-Malaria Drug Policy Updated - ENDocument19 pagesYemen - Anti-Malaria Drug Policy Updated - ENAmmarNo ratings yet
- Efficacy of Artemisinin-Lumefantrine For The TreatDocument19 pagesEfficacy of Artemisinin-Lumefantrine For The Treatdavid mchembeNo ratings yet
- Update On MalariaDocument8 pagesUpdate On MalariaVivi DeviyanaNo ratings yet
- Draft AMD Version English - 2018 PDFDocument17 pagesDraft AMD Version English - 2018 PDFAmmarNo ratings yet
- 1 s2.0 S2387020620304745 MainDocument8 pages1 s2.0 S2387020620304745 MainabirackshaanwirajayaNo ratings yet
- Plasmotec MalariaDocument11 pagesPlasmotec MalariaZero_SugarNo ratings yet
- Brit J Clinical Pharma - 2021 - Kiguba - Pharmacovigilance in Low and Middle Income Countries A Review With ParticularDocument19 pagesBrit J Clinical Pharma - 2021 - Kiguba - Pharmacovigilance in Low and Middle Income Countries A Review With ParticularlizaNo ratings yet
- Factors Associated With Utilization of Malaria Preventive and Control Measures Among Pregnant Women Attending Antenatal Clinic at Kisumu County Referral Hospital in Kisumu City Western KenyaDocument22 pagesFactors Associated With Utilization of Malaria Preventive and Control Measures Among Pregnant Women Attending Antenatal Clinic at Kisumu County Referral Hospital in Kisumu City Western KenyaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Arnold Work On Gametocidal Activity of CryptolepineDocument9 pagesArnold Work On Gametocidal Activity of CryptolepineTetteh JudeNo ratings yet
- Drug Resistant Tuberculosis and Associated Factors Among Residents of Port Harcourt, Nigeria.Document6 pagesDrug Resistant Tuberculosis and Associated Factors Among Residents of Port Harcourt, Nigeria.ijmb333No ratings yet
- Efficacy of Artemether Lumefantrine Versus DihydroartemisininDocument8 pagesEfficacy of Artemether Lumefantrine Versus DihydroartemisininAnida HasnaNo ratings yet
- Jurnal ThalDocument13 pagesJurnal Thalvouwije323No ratings yet
- Vol. 1 Issue 4 April 2008 - 1Document6 pagesVol. 1 Issue 4 April 2008 - 1Maricris RicanaNo ratings yet
- Drug Policy 08Document13 pagesDrug Policy 08egalivanNo ratings yet
- Prevalence and Determinants of Malaria Infection Among Pregnant Women AttendingDocument26 pagesPrevalence and Determinants of Malaria Infection Among Pregnant Women AttendingsemabiaabenaNo ratings yet
- NigeriaDocument8 pagesNigeriaRaden AkbarNo ratings yet
- Malaria PreventionDocument35 pagesMalaria PreventionRaúlNo ratings yet
- 2011 - Frank Baiden - TMIH - Would Rational Use of Antibiotics Be Compromised in Era of TestingDocument3 pages2011 - Frank Baiden - TMIH - Would Rational Use of Antibiotics Be Compromised in Era of TestinggrowlfunNo ratings yet
- Global Malaria Control and Elimination:: Report of A Technical ReviewDocument54 pagesGlobal Malaria Control and Elimination:: Report of A Technical ReviewNeha PalsikarNo ratings yet
- A Bayesian Spatio-Temporal Analysis of Malaria in The Greater Accra Region of Ghana From 2015 To 2019Document15 pagesA Bayesian Spatio-Temporal Analysis of Malaria in The Greater Accra Region of Ghana From 2015 To 2019Francisca CatacutanNo ratings yet
- Antimalaria Drug PolicyDocument35 pagesAntimalaria Drug PolicyBobskinny100% (1)
- Priority and Emerging Diseases and Their Impact On Health Promotion Programmes - 2023Document40 pagesPriority and Emerging Diseases and Their Impact On Health Promotion Programmes - 2023Incredible EbenNo ratings yet
- Malaria Prevention Practices and Associated Factors Among Households of Hawassa City Administration, Southern Ethiopia, 2020Document12 pagesMalaria Prevention Practices and Associated Factors Among Households of Hawassa City Administration, Southern Ethiopia, 2020yowan wandikboNo ratings yet
- Molecules 26 02304 With CoverDocument20 pagesMolecules 26 02304 With CoveralibuxsoomroNo ratings yet
- Improved Malaria Case Management in Formal Private Sector Through Public Private Partnership in Ethiopia: Retrospective Descriptive StudyDocument11 pagesImproved Malaria Case Management in Formal Private Sector Through Public Private Partnership in Ethiopia: Retrospective Descriptive StudyTesfayeNo ratings yet
- CD6 Challenges in Controlling Malaria in India & InitiativesDocument12 pagesCD6 Challenges in Controlling Malaria in India & InitiativesPrema DharshniNo ratings yet
- Management - Guidelines - of - Malaria - in - Malaysia - (Final) v2 PDFDocument63 pagesManagement - Guidelines - of - Malaria - in - Malaysia - (Final) v2 PDFaiyuanNo ratings yet
- Evaluation of The Challenges Faced by Health Workers Managing Patients With Severe Malaria in Kanyabwanga Health Centre III Mitooma District UgandaDocument16 pagesEvaluation of The Challenges Faced by Health Workers Managing Patients With Severe Malaria in Kanyabwanga Health Centre III Mitooma District UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Eng PDFDocument232 pagesEng PDFAbubakar JallohNo ratings yet
- Malaria JournalDocument8 pagesMalaria JournalMridula RajprakashNo ratings yet
- Jurnal Internasional Mikrobiologi Dan Parasitologi-Malaria Di NigeriaDocument15 pagesJurnal Internasional Mikrobiologi Dan Parasitologi-Malaria Di NigeriaVicka Fitri EnjelinaNo ratings yet
- Project WorkDocument45 pagesProject WorkFanenter EmmanuelNo ratings yet
- Awareness and Use of Malaria Prevention Measures Among Child-Bearing Aged Women in Jere Local Government Area, Borno State, NigeriaDocument21 pagesAwareness and Use of Malaria Prevention Measures Among Child-Bearing Aged Women in Jere Local Government Area, Borno State, NigeriaIJMSRTNo ratings yet
- Invited Speakers' Abstracts: Track 1: Infectious and Neglected DiseasesDocument47 pagesInvited Speakers' Abstracts: Track 1: Infectious and Neglected DiseasesMiguel AlcaNo ratings yet
- 2015 Article 794Document9 pages2015 Article 794Hyung ArdiNo ratings yet
- Eng PDFDocument232 pagesEng PDFFallen StarNo ratings yet
- 1 - Malaria VaccineDocument10 pages1 - Malaria VaccineAda NwamemeNo ratings yet
- Epidemiology and Control of Malaria (With A Focus On Sub-Saharan Africa)Document30 pagesEpidemiology and Control of Malaria (With A Focus On Sub-Saharan Africa)Suchie ILyasNo ratings yet
- Encyclopedia of Infectious Diseases: Modern MethodologiesFrom EverandEncyclopedia of Infectious Diseases: Modern MethodologiesMichel TibayrencNo ratings yet
- IOCLDocument94 pagesIOCLDebabrat SaikiaNo ratings yet
- 4 Mass Transfer Coefficients PDFDocument17 pages4 Mass Transfer Coefficients PDFYee LingNo ratings yet
- Sirona C5+ Dental Unit Cleaning InstructionsDocument38 pagesSirona C5+ Dental Unit Cleaning InstructionsRoberto FalconeNo ratings yet
- Khwaja Sara Activism: The Politics of Gender Ambiguity in Pakistan (Faris A. Khan)Document11 pagesKhwaja Sara Activism: The Politics of Gender Ambiguity in Pakistan (Faris A. Khan)Faris A. KhanNo ratings yet
- Codein 15 MG Aptil - Mei 2023Document4 pagesCodein 15 MG Aptil - Mei 2023Nikolas EdwinNo ratings yet
- 9 Pamphlet-Healthy-RelationshipDocument2 pages9 Pamphlet-Healthy-Relationshipapi-277292908No ratings yet
- Reassessment Form (Fillable)Document4 pagesReassessment Form (Fillable)Jason Tutt GinNo ratings yet
- Module 1: An Introduction To Psychology: What You Will LearnDocument16 pagesModule 1: An Introduction To Psychology: What You Will LearnDiana PascuNo ratings yet
- Paragraphs: A. B. C. D. E. FDocument4 pagesParagraphs: A. B. C. D. E. FAnh Cường ĐỗNo ratings yet
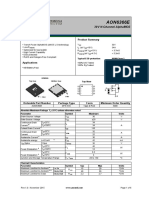
- AON6366E: General Description Product SummaryDocument6 pagesAON6366E: General Description Product SummaryHumberto YumaNo ratings yet
- Chapter IiiDocument5 pagesChapter IiiAjzNo ratings yet
- Southeast Asia Youth Leadership Program: Student Application FormDocument3 pagesSoutheast Asia Youth Leadership Program: Student Application FormAn ViNo ratings yet
- Temperature of Food - FinalDocument1 pageTemperature of Food - FinalMMNo ratings yet
- Ethical and Professional Issues in Group PracticeDocument16 pagesEthical and Professional Issues in Group PracticeTrini Atters50% (2)
- CHN RleDocument5 pagesCHN RleAntoinette Peleña100% (1)
- Wendra Deka Saputra: P R O F Il EDocument1 pageWendra Deka Saputra: P R O F Il EvheNo ratings yet
- Post Incident Damage Assessment ChecklistDocument9 pagesPost Incident Damage Assessment ChecklistFerdinand M. TurbanosNo ratings yet
- Cyto 2.4Document5 pagesCyto 2.4Medtech SoonNo ratings yet
- CESC - Lesson 2 - Community DynamicsDocument25 pagesCESC - Lesson 2 - Community DynamicsZaharaNo ratings yet
- API 651 QuestionsDocument4 pagesAPI 651 QuestionsMohammed YoussefNo ratings yet
- KVK ReportDocument27 pagesKVK ReportAniNo ratings yet
- Ins CICADocument2 pagesIns CICARyan Burnang PurbaNo ratings yet
- Learning To Manage Health Information: A Theme For Clinical EducationDocument48 pagesLearning To Manage Health Information: A Theme For Clinical EducationPatients Know Best100% (2)
- National Institute of Textile Engineering and Research (NITER)Document6 pagesNational Institute of Textile Engineering and Research (NITER)shahadat hossainNo ratings yet
- Dheeraj Coca Cola MbaDocument84 pagesDheeraj Coca Cola Mbaranaindia2011100% (1)
- ECG Holter H12+Document2 pagesECG Holter H12+Dhilah 9246No ratings yet
- Work Program For RoadsDocument8 pagesWork Program For RoadsSupun KariyawasamNo ratings yet
- Texto - Banting DietDocument33 pagesTexto - Banting Diettmendes00No ratings yet
- Sound Proof Canopy Model:: Industrial RangeDocument1 pageSound Proof Canopy Model:: Industrial Rangesales3 iaescoNo ratings yet