Download as pdf or txt
You might also like
- An Easy and Interesting Textbook of Homoeopathic Materia Medica S K Chakraborty.01756 1preface ContentsDocument18 pagesAn Easy and Interesting Textbook of Homoeopathic Materia Medica S K Chakraborty.01756 1preface ContentsMelquiades RuizNo ratings yet
- Perinatal Management of GastroschisisDocument7 pagesPerinatal Management of GastroschisisEga AihenaNo ratings yet
- Incidence, Presentation and Management of Bartholin's Gland Cysts:Abscesses A Four Year Review in Federal Teaching Hospital, Abakaliki, South-East NigeriaDocument8 pagesIncidence, Presentation and Management of Bartholin's Gland Cysts:Abscesses A Four Year Review in Federal Teaching Hospital, Abakaliki, South-East NigeriaNabil Sangga BuanaNo ratings yet
- Management of Bartholin's Gland Swelling in A Tertiary Health Institution in North-Western NigeriaDocument4 pagesManagement of Bartholin's Gland Swelling in A Tertiary Health Institution in North-Western Nigerialidwina143No ratings yet
- Bartholin gland masses - UpToDateDocument17 pagesBartholin gland masses - UpToDatechdxemailNo ratings yet
- Patil Et Al, 2007. Bartolinite e Cisto de BartolinDocument6 pagesPatil Et Al, 2007. Bartolinite e Cisto de BartolinYulian RyandraNo ratings yet
- Clinical Manifestations and Management of Hospitalized Women With Bartholin Versus Non Bartholin Vulvar AbscessDocument4 pagesClinical Manifestations and Management of Hospitalized Women With Bartholin Versus Non Bartholin Vulvar AbscessPaul HartingNo ratings yet
- Bartolinitis 110321214934 Phpapp02Document5 pagesBartolinitis 110321214934 Phpapp02Aina NurlailaNo ratings yet
- Case Report Riska Permata Sari (N 111 16 032)Document10 pagesCase Report Riska Permata Sari (N 111 16 032)syaviraNo ratings yet
- Mitchell, 1939: DefinitionsDocument4 pagesMitchell, 1939: DefinitionsIntan Nur PratiwiNo ratings yet
- Fallopian Tubes - Literature Review of Anatomy and Etiology in Female InfertilityDocument4 pagesFallopian Tubes - Literature Review of Anatomy and Etiology in Female InfertilityRekha KORANGANo ratings yet
- Urinary Tract Infection Diagnosis and Management For NursesDocument8 pagesUrinary Tract Infection Diagnosis and Management For NursesRonaica InocNo ratings yet
- Animals 12 02489 With CoverDocument17 pagesAnimals 12 02489 With Coverpalsantanu8837276365No ratings yet
- Bartholin CystDocument2 pagesBartholin CystDanielNo ratings yet
- Bartolin 1 PDFDocument6 pagesBartolin 1 PDFIzzatush SholihahNo ratings yet
- Perinatal Management of Gastroschisis PDFDocument7 pagesPerinatal Management of Gastroschisis PDFhakimrosliNo ratings yet
- Perinatal Management of Gastroschisis PDFDocument7 pagesPerinatal Management of Gastroschisis PDFhakimrosliNo ratings yet
- Sofra 1Document8 pagesSofra 1Sofranita Ladyas PutriNo ratings yet
- A Case Study On Ruptured Ectopic Pregnancy: Lyceum Northwestern UniversityDocument39 pagesA Case Study On Ruptured Ectopic Pregnancy: Lyceum Northwestern UniversityHomework PingNo ratings yet
- Paper05 Jan-Jun2007Document6 pagesPaper05 Jan-Jun2007cystanarisaNo ratings yet
- Menopause, Hormone Treatment and Urinary Incontinence at MidlifeDocument5 pagesMenopause, Hormone Treatment and Urinary Incontinence at MidlifeherryNo ratings yet
- Abnormal Uterine Bleeding in Perimenopausal WomenDocument15 pagesAbnormal Uterine Bleeding in Perimenopausal WomenOrchid LandNo ratings yet
- Female Urinary Tract Infections in Clinical PracticeFrom EverandFemale Urinary Tract Infections in Clinical PracticeBob YangNo ratings yet
- Differential Diagnosis of The Adnexal Mass - UpToDateDocument37 pagesDifferential Diagnosis of The Adnexal Mass - UpToDatedahiheg756No ratings yet
- Tubo - Ovarian ProcessDocument7 pagesTubo - Ovarian ProcessRosel RomarateNo ratings yet
- Bartholin Gland Diseases 2Document13 pagesBartholin Gland Diseases 2gabriella azaliaNo ratings yet
- Mullerian MalformationsDocument6 pagesMullerian MalformationsMau JkjlNo ratings yet
- Concept of Leucorrhoea and Its Understanding in The Light of Unani MedicineDocument8 pagesConcept of Leucorrhoea and Its Understanding in The Light of Unani Medicinedrraja543No ratings yet
- Neonatal Tetanus in African Children: Causes, Symptoms, Predisposing Factors, Prevention and ControlDocument4 pagesNeonatal Tetanus in African Children: Causes, Symptoms, Predisposing Factors, Prevention and Controlzul090No ratings yet
- Female Genital Tuberculosis-PatelDocument37 pagesFemale Genital Tuberculosis-PatelLionel BaniquedNo ratings yet
- The Gynecologic History and Pelvic Examination Up To Date 2016Document14 pagesThe Gynecologic History and Pelvic Examination Up To Date 2016Mateo GlNo ratings yet
- A Care Study of A Calculous Cholecystitis PatientDocument28 pagesA Care Study of A Calculous Cholecystitis PatientFii Tornubari SamuelNo ratings yet
- Background of CaseDocument8 pagesBackground of CaseKathleen Castro MojicaNo ratings yet
- Acute Appendicitis Caused by Endometriosis: A Case Report: Casereport Open AccessDocument5 pagesAcute Appendicitis Caused by Endometriosis: A Case Report: Casereport Open Accessbewketuabebe31No ratings yet
- Acute Appendicitis in Adults UpToDateDocument35 pagesAcute Appendicitis in Adults UpToDateAra ThalianaNo ratings yet
- Asymptomatic Bacteriuria Among Students of Igbinedion University OkadaDocument55 pagesAsymptomatic Bacteriuria Among Students of Igbinedion University Okadachigreat computersNo ratings yet
- Wjarr 2024 0858Document7 pagesWjarr 2024 0858mcvallespinNo ratings yet
- To Isolate and Identify The Etiological Agents and Establish The Co-Relation Between Pyuria and Significant Bacteriuria Among Patients Suspected of Urinary Tract InfectionDocument9 pagesTo Isolate and Identify The Etiological Agents and Establish The Co-Relation Between Pyuria and Significant Bacteriuria Among Patients Suspected of Urinary Tract InfectionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Postmenopausal Bleeding - StatPearls - NCBI BooksDocument11 pagesPostmenopausal Bleeding - StatPearls - NCBI BooksKalaivathanan VathananNo ratings yet
- Case ReportDocument5 pagesCase ReportLifia VirginiaNo ratings yet
- Osun State University, Osogbo: Department of Nursing SciencesDocument6 pagesOsun State University, Osogbo: Department of Nursing SciencesGreg Carmela annNo ratings yet
- Incidence, Diagnosis and Management of Tubal and Nontubal Ectopic Pregnancies: A ReviewDocument20 pagesIncidence, Diagnosis and Management of Tubal and Nontubal Ectopic Pregnancies: A ReviewwlNo ratings yet
- Ilovepdf MergedDocument53 pagesIlovepdf MergedHardikNo ratings yet
- The Distribution of Human Intestinal Stool Parasites With Respect To Gender and Age in A District Hospital Setting in Biyem-Assi Yaound: A Retrospective StudyDocument8 pagesThe Distribution of Human Intestinal Stool Parasites With Respect To Gender and Age in A District Hospital Setting in Biyem-Assi Yaound: A Retrospective StudyEditor IJTSRDNo ratings yet
- Cases Journal: Torsion of Ovarian Cyst During Pregnancy: A Case ReportDocument3 pagesCases Journal: Torsion of Ovarian Cyst During Pregnancy: A Case ReportAde Gustina SiahaanNo ratings yet
- IntroductionDocument2 pagesIntroductionSydelle GravadorNo ratings yet
- JETIR1808875Document8 pagesJETIR1808875UsmleNo ratings yet
- Uterine MyomaDocument38 pagesUterine MyomaErika Capitly100% (1)
- Menopausia ConsensoDocument9 pagesMenopausia ConsensoVALENTINA LICETH MEDINA JIMÉNEZNo ratings yet
- Adult Intussusception: An Institutional Experience and Review of LiteratureDocument6 pagesAdult Intussusception: An Institutional Experience and Review of LiteraturenurfitriaNo ratings yet
- Endometriosis - Pathogenesis, Clinical Features, and Diagnosis - UpToDateDocument39 pagesEndometriosis - Pathogenesis, Clinical Features, and Diagnosis - UpToDatefujimeisterNo ratings yet
- Consensus On Current Management of EndometriosisDocument17 pagesConsensus On Current Management of EndometriosisCristina BravoNo ratings yet
- Chapter I Preliminary A. BackgroundDocument14 pagesChapter I Preliminary A. BackgroundPMR SMA Negri 11 Plg PAMERABELSNo ratings yet
- Acute Appendicitis in Adults: Clinical Manifestations and Differential DiagnosisDocument35 pagesAcute Appendicitis in Adults: Clinical Manifestations and Differential DiagnosissebasNo ratings yet
- Clinical Presentations and Epidemiology of Urinary Tract InfectionsDocument11 pagesClinical Presentations and Epidemiology of Urinary Tract InfectionsdimasNo ratings yet
- An Appraisal of Retained Placenta in SokotoDocument5 pagesAn Appraisal of Retained Placenta in SokotoDerianti NurhidayahNo ratings yet
- CECAV-UTAD Publications: Advances in Medicine and Biology. Volume 94Document25 pagesCECAV-UTAD Publications: Advances in Medicine and Biology. Volume 94MicheleBerselliNo ratings yet
- Bedah - Prekas AppendisitisDocument15 pagesBedah - Prekas AppendisitisALfianca Yudha RachmandaNo ratings yet
- Torsion Ovarian CystDocument10 pagesTorsion Ovarian CystDani SetiawanNo ratings yet
- 1 Endometriosis: Epidemiology and Aetiological Factors: Paola Vigano'Document24 pages1 Endometriosis: Epidemiology and Aetiological Factors: Paola Vigano'kurniaNo ratings yet
- Brig Anti 2017Document18 pagesBrig Anti 2017Marjorie Lisseth Calderón LozanoNo ratings yet
- Structure of Cilia and Flagella: - by Neha LoharDocument18 pagesStructure of Cilia and Flagella: - by Neha Loharjoy parimalaNo ratings yet
- 13 1.lung Auscultation#8E2EDocument23 pages13 1.lung Auscultation#8E2EAlina CazanNo ratings yet
- Persuasive Position Research PaperDocument7 pagesPersuasive Position Research Paperapi-575240898No ratings yet
- GR 3 WTR SQDocument6 pagesGR 3 WTR SQDanilo Fronda Jr.No ratings yet
- Osteochondritis Dissecans: Vivek PandeyDocument25 pagesOsteochondritis Dissecans: Vivek PandeyRabin DasNo ratings yet
- INFERENCE Questions in CR and RCDocument11 pagesINFERENCE Questions in CR and RCMdFarukHossainNo ratings yet
- Skripsi Jonathan Darell Widjaja 1206230025Document41 pagesSkripsi Jonathan Darell Widjaja 1206230025Jonathan Darell WijayaNo ratings yet
- Hemostasis ReviewerDocument14 pagesHemostasis ReviewerDayledaniel SorvetoNo ratings yet
- DVM Bassem BazzezDocument2 pagesDVM Bassem Bazzezkouloud dibiNo ratings yet
- Fundamentals of Chest RadiologyDocument119 pagesFundamentals of Chest RadiologyAlexandra DîrțuNo ratings yet
- Thyroid SwellingDocument8 pagesThyroid SwellingDn Ezrinah Dn Esham50% (2)
- Price: Pediatric Nursing, 10 Edition: Open Book Quizzes Chapter 10: Disorders of The ToddlerDocument2 pagesPrice: Pediatric Nursing, 10 Edition: Open Book Quizzes Chapter 10: Disorders of The ToddlermickjagerNo ratings yet
- CASE REPORT GEA & Acute DiarrheaDocument7 pagesCASE REPORT GEA & Acute DiarrheatantsaNo ratings yet
- Jurnal Utama ProstoDocument5 pagesJurnal Utama ProstoParlin BrutuNo ratings yet
- Treatment Options For Missing Teeth PDFDocument7 pagesTreatment Options For Missing Teeth PDFNajeeb UllahNo ratings yet
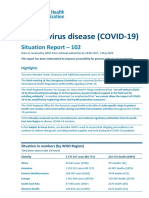
- Coronavirus Disease (COVID-19) : Situation Report - 102Document16 pagesCoronavirus Disease (COVID-19) : Situation Report - 102CityNewsTorontoNo ratings yet
- D Đoán 3Document17 pagesD Đoán 3huycomfNo ratings yet
- The SkullDocument123 pagesThe SkullAnonymous k8rDEsJsU1No ratings yet
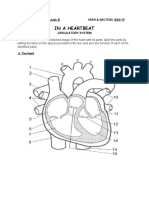
- Circulatory System ActivityDocument5 pagesCirculatory System ActivityKeen Jude CaminosNo ratings yet
- The Dharani Sutra of The Buddha On Longevity - The Extinction of Offences and The Protection of Young Children.Document16 pagesThe Dharani Sutra of The Buddha On Longevity - The Extinction of Offences and The Protection of Young Children.Nga WangNo ratings yet
- Human Digestive SystemDocument11 pagesHuman Digestive SystemSyeda NafeezaNo ratings yet
- Dumbre - 2012 - Effect of Chandraprabha Vati in Experimental Prostatic Hyperplasia and Inflammation in RatsDocument3 pagesDumbre - 2012 - Effect of Chandraprabha Vati in Experimental Prostatic Hyperplasia and Inflammation in RatsHendra Wana Nur'aminNo ratings yet
- Outsmarting Cats PDFDocument601 pagesOutsmarting Cats PDFRichard Leong100% (1)
- Kansas KCI Form B Medical ExemptionDocument1 pageKansas KCI Form B Medical ExemptionDonnaNo ratings yet
- Acariasis: ImportanceDocument17 pagesAcariasis: ImportanceCristina Maria CampeanNo ratings yet
- Benifits of SuvarnaprashanDocument2 pagesBenifits of Suvarnaprashanharish4ayur100% (1)
- PAT Bhs Inggris XIDocument7 pagesPAT Bhs Inggris XIandi taniaNo ratings yet
- Histology of Nervous TissueDocument35 pagesHistology of Nervous TissueGlenn Rey D. AninoNo ratings yet
- Physioex Lab Report: Pre-Lab Quiz ResultsDocument3 pagesPhysioex Lab Report: Pre-Lab Quiz ResultsNicole de Leon0% (1)