
Calcium Oxalate Stones
Calcium Oxalate Stones
You might also like
- Nursing Care Plans For Renal CalculiDocument3 pagesNursing Care Plans For Renal CalculiRaveen mayi77% (22)
- Healthlink Phone Call by Marie MagoonDocument17 pagesHealthlink Phone Call by Marie MagoonCTV CalgaryNo ratings yet
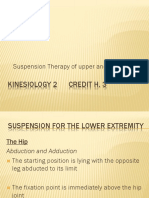
- Suspension Therapy of Upper and Lower LimbDocument23 pagesSuspension Therapy of Upper and Lower LimbM Farrukh shahzad100% (6)
- Hospital Management System PDFDocument16 pagesHospital Management System PDFsumathy83% (6)
- Spine and Spinal Cord InjuryDocument39 pagesSpine and Spinal Cord InjuryblackcatNo ratings yet
- Kidney StonesDocument6 pagesKidney StonesChris ChanNo ratings yet
- Management of Patients With Urinary and Kidney Stones: On Completion of This Chapter, The Learner Will Be Able ToDocument11 pagesManagement of Patients With Urinary and Kidney Stones: On Completion of This Chapter, The Learner Will Be Able TojhcacbszkjcnNo ratings yet
- UROLITHIASISDocument25 pagesUROLITHIASISPaulo ManlangitNo ratings yet
- UrolithiasisDocument31 pagesUrolithiasisRatih Kusumaning MumpuniNo ratings yet
- Rinary Tone Isease: Dr. Nurul Akbar, Sp.UDocument54 pagesRinary Tone Isease: Dr. Nurul Akbar, Sp.USiti NurdiantiNo ratings yet
- Kidney Stones: Signs and SymptomsDocument22 pagesKidney Stones: Signs and SymptomsSher KhanNo ratings yet
- Batu Ginjal (Kidney Stone)Document11 pagesBatu Ginjal (Kidney Stone)Qorry AmandaNo ratings yet
- Script 2 - Kidney StonesDocument3 pagesScript 2 - Kidney Stonesir_yu9840No ratings yet
- Nephrolithiasis 170409233401Document79 pagesNephrolithiasis 170409233401FeniNo ratings yet
- Kidney StonesDocument62 pagesKidney StonesAura DiscyacittaNo ratings yet
- 1.urinary LithiasisDocument22 pages1.urinary LithiasisMohamed AbduNo ratings yet
- 31 - Renal Caliculi PDFDocument33 pages31 - Renal Caliculi PDFEITHAR OmarNo ratings yet
- Av Av Av Av Av Av Av Av Av Av Av AvDocument4 pagesAv Av Av Av Av Av Av Av Av Av Av AvJoyce Ramos CadondonNo ratings yet
- Stone FormationDocument16 pagesStone Formationkulsum fatimaNo ratings yet
- Kidney Stones & Uretral Stones: What Are Stones and The Difference Between Kidney Stones and Ureteral Stones?Document21 pagesKidney Stones & Uretral Stones: What Are Stones and The Difference Between Kidney Stones and Ureteral Stones?Hendrikus Surya Adhi PutraNo ratings yet
- Dbu Collage of Medicine Suregery Lecter For Medical Students by Shitahun ADocument83 pagesDbu Collage of Medicine Suregery Lecter For Medical Students by Shitahun ASisay FentaNo ratings yet
- NephrolithiasisDocument10 pagesNephrolithiasisGERSON RYANTONo ratings yet
- Etiologi: Laporan Pendahuluan UROLITHIASISDocument14 pagesEtiologi: Laporan Pendahuluan UROLITHIASISdesiNo ratings yet
- Clinical Presentation: Kidney Stone SymptomsDocument16 pagesClinical Presentation: Kidney Stone SymptomsangelynchristabellaNo ratings yet
- Stones in KidneyDocument7 pagesStones in Kidneygujji111No ratings yet
- Surgery Urinary Lithiasis DR - HazimDocument8 pagesSurgery Urinary Lithiasis DR - Hazimhussain AltaherNo ratings yet
- UrolithiasisDocument8 pagesUrolithiasisvictor zhefaNo ratings yet
- Urolithiasis: MwashambwaDocument38 pagesUrolithiasis: Mwashambwaamira catriNo ratings yet
- DR Artur-UrolithiasisDocument6 pagesDR Artur-UrolithiasisAbeer AlsaeedNo ratings yet
- A Review On Kidney Stone and Its Herbal TreatmentDocument15 pagesA Review On Kidney Stone and Its Herbal TreatmentSabrina JonesNo ratings yet
- Urolithiasis Case ReportDocument14 pagesUrolithiasis Case ReportCarl Elexer Cuyugan Ano100% (3)
- RENAL STONES - DeletedDocument9 pagesRENAL STONES - DeletedSENTHAMIZHSELVAN ANo ratings yet
- Urolithiasis PDFDocument38 pagesUrolithiasis PDFraed ganmNo ratings yet
- Short Seminar On Renal CalculiDocument18 pagesShort Seminar On Renal CalculiBeulah DasariNo ratings yet
- Definition of NephrolithiasisDocument30 pagesDefinition of Nephrolithiasiszz_13No ratings yet
- Kidney Stone: Types of Kidney StonesDocument2 pagesKidney Stone: Types of Kidney StonesPharmacist Amy CharlieNo ratings yet
- Case Study On Kidney StoneDocument36 pagesCase Study On Kidney Stonemanojkumar200624No ratings yet
- Renal StoneDocument8 pagesRenal StonemadhuNo ratings yet
- Stones in The BodyDocument14 pagesStones in The BodyMichaelNo ratings yet
- Nursing Care of Urolithiasis: Nursing Faculty Chatolic University of Widya Mandala Surabaya 2014Document11 pagesNursing Care of Urolithiasis: Nursing Faculty Chatolic University of Widya Mandala Surabaya 2014victor zhefaNo ratings yet
- Introduction - NephrolithiasisDocument5 pagesIntroduction - NephrolithiasismissmakaiNo ratings yet
- Renal CalculiDocument27 pagesRenal CalculiElsy MayjoNo ratings yet
- Cause and Risk FactorsDocument3 pagesCause and Risk FactorsDiệp TuyềnNo ratings yet
- 55.urinary Bladder StoneDocument2 pages55.urinary Bladder Stonekirtyy20No ratings yet
- Urolithiasishellar 150216182159 Conversion Gate01Document38 pagesUrolithiasishellar 150216182159 Conversion Gate01Cindy Julia AmandaNo ratings yet
- Aka: Urolithiasis, Kidney Stone, Renal Calculi, Ureteral Calculus, Renal ColicDocument4 pagesAka: Urolithiasis, Kidney Stone, Renal Calculi, Ureteral Calculus, Renal ColicMarlin Nouelle Agpalza SacramedNo ratings yet
- RenalDocument24 pagesRenalshamiyahNo ratings yet
- Disease Etiology/ Composition Pathology Histologic Feature/Morphology Gross Appearance Incidence Clinical Presentation Treatment PrognosisDocument2 pagesDisease Etiology/ Composition Pathology Histologic Feature/Morphology Gross Appearance Incidence Clinical Presentation Treatment PrognosisKryscel CzarinahNo ratings yet
- Urolithiasis: ObjectivesDocument11 pagesUrolithiasis: ObjectivesOkki Masitah Syahfitri NasutionNo ratings yet
- Siddhars Thought On Renal CalculaiDocument78 pagesSiddhars Thought On Renal CalculaiSabaRajooNo ratings yet
- Urolithiasis PowerpointDocument41 pagesUrolithiasis PowerpointPinkrose Chiong FabellaNo ratings yet
- KB 10Document5 pagesKB 10Reband AzadNo ratings yet
- Urolithiasis PDFDocument4 pagesUrolithiasis PDFaaaNo ratings yet
- 1 Urinary StonesDocument11 pages1 Urinary StonesMohamed Al-zichrawyNo ratings yet
- Adult Nursing 1 Renal Calculi 1Document25 pagesAdult Nursing 1 Renal Calculi 1ChonnetteAshlynKingNo ratings yet
- UrolithasisDocument58 pagesUrolithasisHELL RISER GAMINGNo ratings yet
- Nephrolithiasis and UrolithiasisDocument4 pagesNephrolithiasis and UrolithiasisHaseeb RayhanNo ratings yet
- Renal Calculi: Ahmednagar Homoeopathic Medical College & Hospital AhmednagarDocument15 pagesRenal Calculi: Ahmednagar Homoeopathic Medical College & Hospital AhmednagarSuhas IngaleNo ratings yet
- Kidney Stones AdultsDocument12 pagesKidney Stones AdultsMahesh Babu.KNo ratings yet
- RENAL CALCULI ADN Group 2Document10 pagesRENAL CALCULI ADN Group 2Akhalia BrownNo ratings yet
- Diseases of Urinary SystemDocument39 pagesDiseases of Urinary SystemRupak PandeyNo ratings yet
- A Simple Guide To Urinary Stones, Diagnosis, Treatment And Related ConditionsFrom EverandA Simple Guide To Urinary Stones, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Innate Immune ResponsesDocument4 pagesInnate Immune Responsesbagas rachmadiNo ratings yet
- Effect of Patent Ductus Arteriosus On Pulmonary Vascular DiseaseDocument6 pagesEffect of Patent Ductus Arteriosus On Pulmonary Vascular Diseasebagas rachmadiNo ratings yet
- ReportDocument3 pagesReportbagas rachmadiNo ratings yet
- Transcatheter Closure of Patent Ductus ArteriosusDocument5 pagesTranscatheter Closure of Patent Ductus Arteriosusbagas rachmadiNo ratings yet
- Competitive Programming: Sistem Dan Tekonologi InformasiDocument3 pagesCompetitive Programming: Sistem Dan Tekonologi Informasibagas rachmadiNo ratings yet
- Impressions in Implant Dentistry: S. Bhakta, J. Vere, I. Calder and R. PatelDocument7 pagesImpressions in Implant Dentistry: S. Bhakta, J. Vere, I. Calder and R. Pateleswar1105820% (1)
- FasTrack - Online Tracking Program of The AMERICAN BOARD OF INTERNAL MEDICINEDocument20 pagesFasTrack - Online Tracking Program of The AMERICAN BOARD OF INTERNAL MEDICINEabimorgNo ratings yet
- Sample Acceptance & Rejection CriteriaDocument26 pagesSample Acceptance & Rejection CriteriaSayan GhoshalNo ratings yet
- Paraneoplastic DermatosesDocument57 pagesParaneoplastic DermatosesMohamed Riyaz100% (1)
- RT 255 Dsa Fluoro 2010 11Document54 pagesRT 255 Dsa Fluoro 2010 11IBRAHIM100% (1)
- Curs Epidemiologie Parte NgeneralaDocument142 pagesCurs Epidemiologie Parte NgeneralaDragomir P. AdrianNo ratings yet
- 13 14 Bro Sg2safetyneedlessyringes EngDocument2 pages13 14 Bro Sg2safetyneedlessyringes EngЭрикмартин ПересNo ratings yet
- Pre-Operative Fasting - 60 Years On From MendelsonDocument4 pagesPre-Operative Fasting - 60 Years On From MendelsonArdian PratiaksaNo ratings yet
- The 10 GodsDocument2 pagesThe 10 Godslucentum56No ratings yet
- Forxiga Presentation Kaltim - Prof AgungDocument36 pagesForxiga Presentation Kaltim - Prof AgungSanrio NeuroNo ratings yet
- HumanNutritionMSC PDFDocument28 pagesHumanNutritionMSC PDFIndunil Prasanna Bandara WarnasooriyaNo ratings yet
- Azithromycin in PediatricsDocument40 pagesAzithromycin in PediatricsKishore ChandkiNo ratings yet
- Jennifer Jones, PSY.D. LMHC: Work ExperienceDocument2 pagesJennifer Jones, PSY.D. LMHC: Work ExperienceAlam ZebNo ratings yet
- Lecture 6 - Respiratory DisordersDocument7 pagesLecture 6 - Respiratory DisordersMaikaylaNo ratings yet
- EDS Hypermobility TypeDocument3 pagesEDS Hypermobility TypeRichard NavarroNo ratings yet
- The Ancient Techniques of AcupressureDocument3 pagesThe Ancient Techniques of AcupressureunlimitivNo ratings yet
- Insert Hep B Engerix-BDocument16 pagesInsert Hep B Engerix-BshifanahmedNo ratings yet
- CellulitisDocument8 pagesCellulitisTricia Llorin100% (1)
- Hydrogen Peroxide For Ear Infections/waxDocument1 pageHydrogen Peroxide For Ear Infections/waxAishwarya KrishnanNo ratings yet
- Generic NameDocument10 pagesGeneric NameConadel AlicdanNo ratings yet
- XDocument237 pagesXsigmundmaharaja2368No ratings yet
- Erythromycin: Bacteriostatic, Protein-Synthesis Inhibitors That Target RibosomeDocument3 pagesErythromycin: Bacteriostatic, Protein-Synthesis Inhibitors That Target RibosomeJubelle Sipalay100% (1)
- Physical Examinations I (JoVE)Document119 pagesPhysical Examinations I (JoVE)Thasya RenaNo ratings yet
- Americare BrochureDocument2 pagesAmericare BrochureEthan WeisheitNo ratings yet
- A Practical Guide To Mental Health and The Law in Ontario, Revised Edition, September 2016Document174 pagesA Practical Guide To Mental Health and The Law in Ontario, Revised Edition, September 2016The London Free PressNo ratings yet
- Bioavailability - A Pharmaceutical ReviewDocument17 pagesBioavailability - A Pharmaceutical Reviewraju155940550% (2)




























































































Download as docx, pdf, or txt
You might also like
- Nursing Care Plans For Renal CalculiDocument3 pagesNursing Care Plans For Renal CalculiRaveen mayi77% (22)
- Healthlink Phone Call by Marie MagoonDocument17 pagesHealthlink Phone Call by Marie MagoonCTV CalgaryNo ratings yet
- Suspension Therapy of Upper and Lower LimbDocument23 pagesSuspension Therapy of Upper and Lower LimbM Farrukh shahzad100% (6)
- Hospital Management System PDFDocument16 pagesHospital Management System PDFsumathy83% (6)
- Spine and Spinal Cord InjuryDocument39 pagesSpine and Spinal Cord InjuryblackcatNo ratings yet
- Kidney StonesDocument6 pagesKidney StonesChris ChanNo ratings yet
- Management of Patients With Urinary and Kidney Stones: On Completion of This Chapter, The Learner Will Be Able ToDocument11 pagesManagement of Patients With Urinary and Kidney Stones: On Completion of This Chapter, The Learner Will Be Able TojhcacbszkjcnNo ratings yet
- UROLITHIASISDocument25 pagesUROLITHIASISPaulo ManlangitNo ratings yet
- UrolithiasisDocument31 pagesUrolithiasisRatih Kusumaning MumpuniNo ratings yet
- Rinary Tone Isease: Dr. Nurul Akbar, Sp.UDocument54 pagesRinary Tone Isease: Dr. Nurul Akbar, Sp.USiti NurdiantiNo ratings yet
- Kidney Stones: Signs and SymptomsDocument22 pagesKidney Stones: Signs and SymptomsSher KhanNo ratings yet
- Batu Ginjal (Kidney Stone)Document11 pagesBatu Ginjal (Kidney Stone)Qorry AmandaNo ratings yet
- Script 2 - Kidney StonesDocument3 pagesScript 2 - Kidney Stonesir_yu9840No ratings yet
- Nephrolithiasis 170409233401Document79 pagesNephrolithiasis 170409233401FeniNo ratings yet
- Kidney StonesDocument62 pagesKidney StonesAura DiscyacittaNo ratings yet
- 1.urinary LithiasisDocument22 pages1.urinary LithiasisMohamed AbduNo ratings yet
- 31 - Renal Caliculi PDFDocument33 pages31 - Renal Caliculi PDFEITHAR OmarNo ratings yet
- Av Av Av Av Av Av Av Av Av Av Av AvDocument4 pagesAv Av Av Av Av Av Av Av Av Av Av AvJoyce Ramos CadondonNo ratings yet
- Stone FormationDocument16 pagesStone Formationkulsum fatimaNo ratings yet
- Kidney Stones & Uretral Stones: What Are Stones and The Difference Between Kidney Stones and Ureteral Stones?Document21 pagesKidney Stones & Uretral Stones: What Are Stones and The Difference Between Kidney Stones and Ureteral Stones?Hendrikus Surya Adhi PutraNo ratings yet
- Dbu Collage of Medicine Suregery Lecter For Medical Students by Shitahun ADocument83 pagesDbu Collage of Medicine Suregery Lecter For Medical Students by Shitahun ASisay FentaNo ratings yet
- NephrolithiasisDocument10 pagesNephrolithiasisGERSON RYANTONo ratings yet
- Etiologi: Laporan Pendahuluan UROLITHIASISDocument14 pagesEtiologi: Laporan Pendahuluan UROLITHIASISdesiNo ratings yet
- Clinical Presentation: Kidney Stone SymptomsDocument16 pagesClinical Presentation: Kidney Stone SymptomsangelynchristabellaNo ratings yet
- Stones in KidneyDocument7 pagesStones in Kidneygujji111No ratings yet
- Surgery Urinary Lithiasis DR - HazimDocument8 pagesSurgery Urinary Lithiasis DR - Hazimhussain AltaherNo ratings yet
- UrolithiasisDocument8 pagesUrolithiasisvictor zhefaNo ratings yet
- Urolithiasis: MwashambwaDocument38 pagesUrolithiasis: Mwashambwaamira catriNo ratings yet
- DR Artur-UrolithiasisDocument6 pagesDR Artur-UrolithiasisAbeer AlsaeedNo ratings yet
- A Review On Kidney Stone and Its Herbal TreatmentDocument15 pagesA Review On Kidney Stone and Its Herbal TreatmentSabrina JonesNo ratings yet
- Urolithiasis Case ReportDocument14 pagesUrolithiasis Case ReportCarl Elexer Cuyugan Ano100% (3)
- RENAL STONES - DeletedDocument9 pagesRENAL STONES - DeletedSENTHAMIZHSELVAN ANo ratings yet
- Urolithiasis PDFDocument38 pagesUrolithiasis PDFraed ganmNo ratings yet
- Short Seminar On Renal CalculiDocument18 pagesShort Seminar On Renal CalculiBeulah DasariNo ratings yet
- Definition of NephrolithiasisDocument30 pagesDefinition of Nephrolithiasiszz_13No ratings yet
- Kidney Stone: Types of Kidney StonesDocument2 pagesKidney Stone: Types of Kidney StonesPharmacist Amy CharlieNo ratings yet
- Case Study On Kidney StoneDocument36 pagesCase Study On Kidney Stonemanojkumar200624No ratings yet
- Renal StoneDocument8 pagesRenal StonemadhuNo ratings yet
- Stones in The BodyDocument14 pagesStones in The BodyMichaelNo ratings yet
- Nursing Care of Urolithiasis: Nursing Faculty Chatolic University of Widya Mandala Surabaya 2014Document11 pagesNursing Care of Urolithiasis: Nursing Faculty Chatolic University of Widya Mandala Surabaya 2014victor zhefaNo ratings yet
- Introduction - NephrolithiasisDocument5 pagesIntroduction - NephrolithiasismissmakaiNo ratings yet
- Renal CalculiDocument27 pagesRenal CalculiElsy MayjoNo ratings yet
- Cause and Risk FactorsDocument3 pagesCause and Risk FactorsDiệp TuyềnNo ratings yet
- 55.urinary Bladder StoneDocument2 pages55.urinary Bladder Stonekirtyy20No ratings yet
- Urolithiasishellar 150216182159 Conversion Gate01Document38 pagesUrolithiasishellar 150216182159 Conversion Gate01Cindy Julia AmandaNo ratings yet
- Aka: Urolithiasis, Kidney Stone, Renal Calculi, Ureteral Calculus, Renal ColicDocument4 pagesAka: Urolithiasis, Kidney Stone, Renal Calculi, Ureteral Calculus, Renal ColicMarlin Nouelle Agpalza SacramedNo ratings yet
- RenalDocument24 pagesRenalshamiyahNo ratings yet
- Disease Etiology/ Composition Pathology Histologic Feature/Morphology Gross Appearance Incidence Clinical Presentation Treatment PrognosisDocument2 pagesDisease Etiology/ Composition Pathology Histologic Feature/Morphology Gross Appearance Incidence Clinical Presentation Treatment PrognosisKryscel CzarinahNo ratings yet
- Urolithiasis: ObjectivesDocument11 pagesUrolithiasis: ObjectivesOkki Masitah Syahfitri NasutionNo ratings yet
- Siddhars Thought On Renal CalculaiDocument78 pagesSiddhars Thought On Renal CalculaiSabaRajooNo ratings yet
- Urolithiasis PowerpointDocument41 pagesUrolithiasis PowerpointPinkrose Chiong FabellaNo ratings yet
- KB 10Document5 pagesKB 10Reband AzadNo ratings yet
- Urolithiasis PDFDocument4 pagesUrolithiasis PDFaaaNo ratings yet
- 1 Urinary StonesDocument11 pages1 Urinary StonesMohamed Al-zichrawyNo ratings yet
- Adult Nursing 1 Renal Calculi 1Document25 pagesAdult Nursing 1 Renal Calculi 1ChonnetteAshlynKingNo ratings yet
- UrolithasisDocument58 pagesUrolithasisHELL RISER GAMINGNo ratings yet
- Nephrolithiasis and UrolithiasisDocument4 pagesNephrolithiasis and UrolithiasisHaseeb RayhanNo ratings yet
- Renal Calculi: Ahmednagar Homoeopathic Medical College & Hospital AhmednagarDocument15 pagesRenal Calculi: Ahmednagar Homoeopathic Medical College & Hospital AhmednagarSuhas IngaleNo ratings yet
- Kidney Stones AdultsDocument12 pagesKidney Stones AdultsMahesh Babu.KNo ratings yet
- RENAL CALCULI ADN Group 2Document10 pagesRENAL CALCULI ADN Group 2Akhalia BrownNo ratings yet
- Diseases of Urinary SystemDocument39 pagesDiseases of Urinary SystemRupak PandeyNo ratings yet
- A Simple Guide To Urinary Stones, Diagnosis, Treatment And Related ConditionsFrom EverandA Simple Guide To Urinary Stones, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Innate Immune ResponsesDocument4 pagesInnate Immune Responsesbagas rachmadiNo ratings yet
- Effect of Patent Ductus Arteriosus On Pulmonary Vascular DiseaseDocument6 pagesEffect of Patent Ductus Arteriosus On Pulmonary Vascular Diseasebagas rachmadiNo ratings yet
- ReportDocument3 pagesReportbagas rachmadiNo ratings yet
- Transcatheter Closure of Patent Ductus ArteriosusDocument5 pagesTranscatheter Closure of Patent Ductus Arteriosusbagas rachmadiNo ratings yet
- Competitive Programming: Sistem Dan Tekonologi InformasiDocument3 pagesCompetitive Programming: Sistem Dan Tekonologi Informasibagas rachmadiNo ratings yet
- Impressions in Implant Dentistry: S. Bhakta, J. Vere, I. Calder and R. PatelDocument7 pagesImpressions in Implant Dentistry: S. Bhakta, J. Vere, I. Calder and R. Pateleswar1105820% (1)
- FasTrack - Online Tracking Program of The AMERICAN BOARD OF INTERNAL MEDICINEDocument20 pagesFasTrack - Online Tracking Program of The AMERICAN BOARD OF INTERNAL MEDICINEabimorgNo ratings yet
- Sample Acceptance & Rejection CriteriaDocument26 pagesSample Acceptance & Rejection CriteriaSayan GhoshalNo ratings yet
- Paraneoplastic DermatosesDocument57 pagesParaneoplastic DermatosesMohamed Riyaz100% (1)
- RT 255 Dsa Fluoro 2010 11Document54 pagesRT 255 Dsa Fluoro 2010 11IBRAHIM100% (1)
- Curs Epidemiologie Parte NgeneralaDocument142 pagesCurs Epidemiologie Parte NgeneralaDragomir P. AdrianNo ratings yet
- 13 14 Bro Sg2safetyneedlessyringes EngDocument2 pages13 14 Bro Sg2safetyneedlessyringes EngЭрикмартин ПересNo ratings yet
- Pre-Operative Fasting - 60 Years On From MendelsonDocument4 pagesPre-Operative Fasting - 60 Years On From MendelsonArdian PratiaksaNo ratings yet
- The 10 GodsDocument2 pagesThe 10 Godslucentum56No ratings yet
- Forxiga Presentation Kaltim - Prof AgungDocument36 pagesForxiga Presentation Kaltim - Prof AgungSanrio NeuroNo ratings yet
- HumanNutritionMSC PDFDocument28 pagesHumanNutritionMSC PDFIndunil Prasanna Bandara WarnasooriyaNo ratings yet
- Azithromycin in PediatricsDocument40 pagesAzithromycin in PediatricsKishore ChandkiNo ratings yet
- Jennifer Jones, PSY.D. LMHC: Work ExperienceDocument2 pagesJennifer Jones, PSY.D. LMHC: Work ExperienceAlam ZebNo ratings yet
- Lecture 6 - Respiratory DisordersDocument7 pagesLecture 6 - Respiratory DisordersMaikaylaNo ratings yet
- EDS Hypermobility TypeDocument3 pagesEDS Hypermobility TypeRichard NavarroNo ratings yet
- The Ancient Techniques of AcupressureDocument3 pagesThe Ancient Techniques of AcupressureunlimitivNo ratings yet
- Insert Hep B Engerix-BDocument16 pagesInsert Hep B Engerix-BshifanahmedNo ratings yet
- CellulitisDocument8 pagesCellulitisTricia Llorin100% (1)
- Hydrogen Peroxide For Ear Infections/waxDocument1 pageHydrogen Peroxide For Ear Infections/waxAishwarya KrishnanNo ratings yet
- Generic NameDocument10 pagesGeneric NameConadel AlicdanNo ratings yet
- XDocument237 pagesXsigmundmaharaja2368No ratings yet
- Erythromycin: Bacteriostatic, Protein-Synthesis Inhibitors That Target RibosomeDocument3 pagesErythromycin: Bacteriostatic, Protein-Synthesis Inhibitors That Target RibosomeJubelle Sipalay100% (1)
- Physical Examinations I (JoVE)Document119 pagesPhysical Examinations I (JoVE)Thasya RenaNo ratings yet
- Americare BrochureDocument2 pagesAmericare BrochureEthan WeisheitNo ratings yet
- A Practical Guide To Mental Health and The Law in Ontario, Revised Edition, September 2016Document174 pagesA Practical Guide To Mental Health and The Law in Ontario, Revised Edition, September 2016The London Free PressNo ratings yet
- Bioavailability - A Pharmaceutical ReviewDocument17 pagesBioavailability - A Pharmaceutical Reviewraju155940550% (2)