
Autism and Seizures
Autism and Seizures
You might also like
- ASD Questionnaire For ParentsDocument8 pagesASD Questionnaire For ParentsSuleman Malik100% (1)
- Speech and Language DisorderDocument6 pagesSpeech and Language Disorderapi-362628618No ratings yet
- Hoof Print-AutisticDocument4 pagesHoof Print-Autisticapi-286772409100% (1)
- Early Behavioral InterventionDocument29 pagesEarly Behavioral InterventionMariaNo ratings yet
- Brisbane EBLT Complete TestDocument32 pagesBrisbane EBLT Complete TestomeraNo ratings yet
- Asperger's Syndrome An Introduction For EducatorsDocument7 pagesAsperger's Syndrome An Introduction For EducatorsDruga DanutNo ratings yet
- PowerBI Interview Questions and AnswersDocument8 pagesPowerBI Interview Questions and AnswersexbisNo ratings yet
- Doterra Pasttense Essential Oil BlendDocument1 pageDoterra Pasttense Essential Oil BlendAlexandru Eduard RotaruNo ratings yet
- Autism DyslexiaDocument2 pagesAutism DyslexiaAutismDyslexiaNo ratings yet
- BEAT AUTISM NOW (BAN) - Booklet 1 – Logically, effectively and inexpensivelyFrom EverandBEAT AUTISM NOW (BAN) - Booklet 1 – Logically, effectively and inexpensivelyNo ratings yet
- Asd-Biomedical Treatments Research EssayDocument5 pagesAsd-Biomedical Treatments Research Essayapi-526505312No ratings yet
- Language Disorder: English Language and Literature Humanities Faculty Jenderal Soedirman University Purwokerto 2016Document12 pagesLanguage Disorder: English Language and Literature Humanities Faculty Jenderal Soedirman University Purwokerto 2016widya khNo ratings yet
- Autism AmishDocument2 pagesAutism AmishPower one100% (1)
- Autism X - ChromosomeDocument190 pagesAutism X - ChromosomeDanciu CristinaNo ratings yet
- AUTISMDocument18 pagesAUTISMNycoNo ratings yet
- Caroline - Walrad - The Autistic Spectrum NotesDocument14 pagesCaroline - Walrad - The Autistic Spectrum Notesnamkay_tenzynNo ratings yet
- Autism Metabolism, Mitochondria, and The MicrobiomeDocument15 pagesAutism Metabolism, Mitochondria, and The MicrobiomeJorge AlvesNo ratings yet
- Risk Factors, Diagnosis, Prognosis and Treatment of AutismDocument36 pagesRisk Factors, Diagnosis, Prognosis and Treatment of AutismCarlos Peña PaterninaNo ratings yet
- Autism and AirportDocument76 pagesAutism and AirportNoraz CompanyNo ratings yet
- Protocols by Resham Malhotra PDFDocument7 pagesProtocols by Resham Malhotra PDFScience NerdNo ratings yet
- Autism Spectrum Disorders in Extremely Preterm Children OriginalDocument9 pagesAutism Spectrum Disorders in Extremely Preterm Children Originalesteban_falcón_12No ratings yet
- Emily Iland Webinar With Autism NOW September 6, 2011Document36 pagesEmily Iland Webinar With Autism NOW September 6, 2011The Autism NOW CenterNo ratings yet
- Diet Texture Progression For Individuals With Autism ASHADocument81 pagesDiet Texture Progression For Individuals With Autism ASHAjhebetaNo ratings yet
- High Rates of Autism Found in Federal Vaccine Injury ProgramDocument4 pagesHigh Rates of Autism Found in Federal Vaccine Injury ProgramTyrone PenningNo ratings yet
- Increasing Speech SouIncreasing Speech Sound Production of Children With Autisnd Production of Children With AutismDocument34 pagesIncreasing Speech SouIncreasing Speech Sound Production of Children With Autisnd Production of Children With AutismPrapanit PntNo ratings yet
- Autism and EpilepsyDocument9 pagesAutism and EpilepsyTessa CruzNo ratings yet
- Autism SchoolDocument5 pagesAutism SchoolBhuvanesh Krishnan100% (1)
- UNCC 300 Assess 2Document2 pagesUNCC 300 Assess 2Usman Farooq100% (1)
- Genetic Causes of Syndromic and Non-Syndromic Autism PDFDocument9 pagesGenetic Causes of Syndromic and Non-Syndromic Autism PDFRaisa CoppolaNo ratings yet
- Angelman SyndromeDocument13 pagesAngelman Syndromeapi-388959318No ratings yet
- Asperger Syndrome SymptomsDocument8 pagesAsperger Syndrome Symptomsapi-277147828No ratings yet
- Autism, Recovery (To Normalcy) ,'' and The Politics of HopeDocument19 pagesAutism, Recovery (To Normalcy) ,'' and The Politics of HopeadhortizNo ratings yet
- Autism Resources: Information For FamiliesDocument1 pageAutism Resources: Information For FamiliesDesislava PeevaNo ratings yet
- Autism Therapy PresentationDocument13 pagesAutism Therapy Presentationapi-339989348No ratings yet
- Brain FogDocument9 pagesBrain FogIsmailNo ratings yet
- O o o o O: Assessment For IdentificationDocument9 pagesO o o o O: Assessment For IdentificationJong Suk Joo (Shuru)No ratings yet
- Specific Language ImpairmentDocument106 pagesSpecific Language ImpairmentKUNNAMPALLIL GEJO JOHNNo ratings yet
- The Impacts of Autism On The FamilyDocument4 pagesThe Impacts of Autism On The FamilyRuth Arcibal RomeroNo ratings yet
- Speech and Language Impairments in Children: Causes, Characteristics, Intervention and OutcomeDocument17 pagesSpeech and Language Impairments in Children: Causes, Characteristics, Intervention and OutcomeCelu CeluNo ratings yet
- Autism Spectrum and Open-MindednessDocument2 pagesAutism Spectrum and Open-MindednessJaime MontoyaNo ratings yet
- Measuring Television AddictionDocument24 pagesMeasuring Television Addictionciprian72100% (1)
- Restricted and Repetitive Behaviors As Strengths Not WeaknessesDocument213 pagesRestricted and Repetitive Behaviors As Strengths Not WeaknessesTomas Torres BarberoNo ratings yet
- Sensory Storytime How-To GuideDocument4 pagesSensory Storytime How-To GuideSaidJanNo ratings yet
- Listen, Screen & Recognize The Red Flags For Autism Spectrum DisordersDocument28 pagesListen, Screen & Recognize The Red Flags For Autism Spectrum DisordersThe Autism NOW CenterNo ratings yet
- AutismDocument34 pagesAutismSrm Genetics100% (1)
- Effects of A Brief Early Start Denver Model (ESDM) - Based Parent Intervention On Toddlers at Risk For Autism Spectrum Disorders A Randomized Controlled TrialDocument14 pagesEffects of A Brief Early Start Denver Model (ESDM) - Based Parent Intervention On Toddlers at Risk For Autism Spectrum Disorders A Randomized Controlled TrialLuis Seixas100% (1)
- Classification of Feeding and Eating DisordersDocument13 pagesClassification of Feeding and Eating DisordersMagito JayaNo ratings yet
- Behavioral Treatment and Normal Educational and Intellectual Functioning in /bung Autistic ChildrenDocument7 pagesBehavioral Treatment and Normal Educational and Intellectual Functioning in /bung Autistic ChildrenMariaNo ratings yet
- The Spectrum of Mitochondrial Disease Ep-3-10Document8 pagesThe Spectrum of Mitochondrial Disease Ep-3-10F4AR100% (1)
- Autism-Strategies For CommunicationDocument21 pagesAutism-Strategies For CommunicationMs.Aishwarya Nallamuthu, Dept. of SLHS, SRIHERNo ratings yet
- What Is AutismDocument4 pagesWhat Is Autismidno1008No ratings yet
- ASD Recovery 2019Document5 pagesASD Recovery 2019verdantlaw100% (1)
- Lovaas BookDocument338 pagesLovaas BooklicheiNo ratings yet
- Autism and EpilepsyDocument5 pagesAutism and Epilepsyclarajimena25No ratings yet
- Childhood DisordersDocument7 pagesChildhood DisordersApOlle Defiesta - DOminguezNo ratings yet
- InTech-Sensory Motor Development in AutismDocument26 pagesInTech-Sensory Motor Development in AutismTânia DiasNo ratings yet
- Promoting Healthy Eating Behaviors in A Safe and Supportive Environment For ChildrenDocument7 pagesPromoting Healthy Eating Behaviors in A Safe and Supportive Environment For Childrenapi-604622509No ratings yet
- Analysis and Evaluation of ASD TheoriesDocument9 pagesAnalysis and Evaluation of ASD Theoriestracycw100% (1)
- Research Supporting DIRDocument6 pagesResearch Supporting DIRsegurryNo ratings yet
- Sexual Recovery Institute - Summer & Fall Saturday Lecture SeriesDocument2 pagesSexual Recovery Institute - Summer & Fall Saturday Lecture SeriesSexRecoveryNo ratings yet
- How To Change Connections in Portfolio Slicer For Power BI Desktop Model - Portfolio SlicerDocument4 pagesHow To Change Connections in Portfolio Slicer For Power BI Desktop Model - Portfolio SlicerexbisNo ratings yet
- Demystifying Chart Types and Design Principles in Power BIDocument61 pagesDemystifying Chart Types and Design Principles in Power BIexbisNo ratings yet
- Power Bi Data Viz Usability Checklist2Document5 pagesPower Bi Data Viz Usability Checklist2exbisNo ratings yet
- So You Want To Be A Business Intelligence (BI) DeveloperDocument5 pagesSo You Want To Be A Business Intelligence (BI) DeveloperexbisNo ratings yet
- Power BI Assessment Dashboard WalkthroughDocument35 pagesPower BI Assessment Dashboard WalkthroughexbisNo ratings yet
- Web Content: With The SQL Server 2008R2 PlatformDocument4 pagesWeb Content: With The SQL Server 2008R2 PlatformexbisNo ratings yet
- PASS - 19 - Corp - Template - v2 - IaaS - Vs - PaaS FinalDocument33 pagesPASS - 19 - Corp - Template - v2 - IaaS - Vs - PaaS FinalexbisNo ratings yet
- Business Intelligence Requirements GatheringDocument2 pagesBusiness Intelligence Requirements GatheringexbisNo ratings yet
- Tracking Data Changes: With Temporal Tables and MoreDocument22 pagesTracking Data Changes: With Temporal Tables and MoreexbisNo ratings yet
- Company Jobtitle Startdate EnddateDocument18 pagesCompany Jobtitle Startdate EnddateexbisNo ratings yet
- Using Ssas 2005 As Ds For Power PivotDocument1 pageUsing Ssas 2005 As Ds For Power PivotexbisNo ratings yet
- Different Types of ForEachLoop EnumeratorDocument38 pagesDifferent Types of ForEachLoop EnumeratorexbisNo ratings yet
- 22 SQL For ModelingDocument51 pages22 SQL For ModelingexbisNo ratings yet
- Multidimensional ModelingDocument12 pagesMultidimensional ModelingexbisNo ratings yet
- Using SSAS 2005 As DS - Calculated MembersDocument4 pagesUsing SSAS 2005 As DS - Calculated MembersexbisNo ratings yet
- Migrating Content Between Report ServersDocument14 pagesMigrating Content Between Report ServersexbisNo ratings yet
- Chart Suggestions - A Thought-StarterDocument1 pageChart Suggestions - A Thought-StarterDoc AllaínNo ratings yet
- Wanna Be A SQL ConsultantDocument20 pagesWanna Be A SQL ConsultantexbisNo ratings yet
- Checklist For Ssas Tabular Model DevelopmentDocument1 pageChecklist For Ssas Tabular Model DevelopmentexbisNo ratings yet
- PL SQL Interview - Career Ride - ImpDocument392 pagesPL SQL Interview - Career Ride - ImpexbisNo ratings yet
- Mesenchymal Stem Cell-Conditioned Medium (Secretome) in Skin Aging A Systematic ReviewDocument24 pagesMesenchymal Stem Cell-Conditioned Medium (Secretome) in Skin Aging A Systematic ReviewThomas UtomoNo ratings yet
- Greenland 2256 2513 6Document258 pagesGreenland 2256 2513 6seacoastonlineNo ratings yet
- Pharm Calcium Channel Blockers (Bahar&Amy) "Vera Dialed The Calcium Channel To Buy A Knife" Verapramil, Diltizaem, NifedipineDocument7 pagesPharm Calcium Channel Blockers (Bahar&Amy) "Vera Dialed The Calcium Channel To Buy A Knife" Verapramil, Diltizaem, Nifedipinecherrybombaz100% (4)
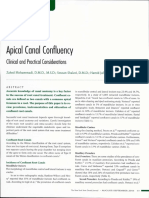
- Apical Canal ConfuencyDocument7 pagesApical Canal ConfuencyPanxo14No ratings yet
- Comprehensive List of American and British Spelling DifferencesDocument36 pagesComprehensive List of American and British Spelling DifferencesshivaNo ratings yet
- Dams Lastlook Microbiology PDFDocument27 pagesDams Lastlook Microbiology PDFChauhan Monika100% (1)
- Asparaginase / Erwinia AsparaginaseDocument10 pagesAsparaginase / Erwinia AsparaginaseMohammed HaiderNo ratings yet
- Bench-To-bedside Review An Approach To Hemodynamic Monitoring Guyton at Bedside - Magder 2012Document7 pagesBench-To-bedside Review An Approach To Hemodynamic Monitoring Guyton at Bedside - Magder 2012Fransisca Dewi KumalaNo ratings yet
- Nursing LeadershipDocument6 pagesNursing LeadershipAyanne03No ratings yet
- Dermoneuromodulation Rev 03Document57 pagesDermoneuromodulation Rev 03dasamoro100% (1)
- Ophthalmonics 1st EditionDocument116 pagesOphthalmonics 1st Editiondhavalb2086% (7)
- Volume 2 GDVs and More - Rev1 Ed6jvjDocument39 pagesVolume 2 GDVs and More - Rev1 Ed6jvjErhan ErtuçNo ratings yet
- PR 1Document47 pagesPR 1Daniel MagcalasNo ratings yet
- September 26, 2018 by Sagar Aryal: Antigen-Properties, Types and Determinants of AntigenicityDocument23 pagesSeptember 26, 2018 by Sagar Aryal: Antigen-Properties, Types and Determinants of AntigenicityEzekiel GantiedNo ratings yet
- CANINE-Canine Transfusion Reactions - Part 2.prevention and TreatmentDocument7 pagesCANINE-Canine Transfusion Reactions - Part 2.prevention and Treatmenttaner_soysurenNo ratings yet
- 6 Yoga Poses You Can Do in Bed Before Sleeping For Better Health PDFDocument21 pages6 Yoga Poses You Can Do in Bed Before Sleeping For Better Health PDFAsfaq SumraNo ratings yet
- Vivir Con ParkinsonDocument22 pagesVivir Con ParkinsonAlexis Muñoz TrincadoNo ratings yet
- Water Electrolytes Part Clinical BiochemistryDocument27 pagesWater Electrolytes Part Clinical BiochemistryAshraf FirdadNo ratings yet
- Afi48 123Document192 pagesAfi48 123nazario1719011No ratings yet
- Mapeh Department: Daily Lesson PlanDocument8 pagesMapeh Department: Daily Lesson PlanJessie FranciscoNo ratings yet
- Nutraceuticals: April 2016Document9 pagesNutraceuticals: April 2016nikita bindakNo ratings yet
- Important Drug Nutrient Interactions: Pamela MasonDocument35 pagesImportant Drug Nutrient Interactions: Pamela MasonRijantono Franciscus MariaNo ratings yet
- KariesDocument4 pagesKariesSherlocknovNo ratings yet
- Care of Low Birth Weight BabiesDocument102 pagesCare of Low Birth Weight Babiesvarshasharma050% (2)
- A Countdown To Orthognathic SurgeryDocument5 pagesA Countdown To Orthognathic SurgeryhaneefmdfNo ratings yet
- Autism - Gender and GeneticsDocument12 pagesAutism - Gender and GeneticsAggrey SmartfieldNo ratings yet
- MIT 9.00 Exam 1 2007 AnswersDocument16 pagesMIT 9.00 Exam 1 2007 AnswersbitternessinmymouthNo ratings yet
- Ethics Assignment Sem 3Document9 pagesEthics Assignment Sem 3api-314566363No ratings yet
- Zeway ReportDocument8 pagesZeway Reportbereket rikitaNo ratings yet













































































































Download as pdf or txt
You might also like
- ASD Questionnaire For ParentsDocument8 pagesASD Questionnaire For ParentsSuleman Malik100% (1)
- Speech and Language DisorderDocument6 pagesSpeech and Language Disorderapi-362628618No ratings yet
- Hoof Print-AutisticDocument4 pagesHoof Print-Autisticapi-286772409100% (1)
- Early Behavioral InterventionDocument29 pagesEarly Behavioral InterventionMariaNo ratings yet
- Brisbane EBLT Complete TestDocument32 pagesBrisbane EBLT Complete TestomeraNo ratings yet
- Asperger's Syndrome An Introduction For EducatorsDocument7 pagesAsperger's Syndrome An Introduction For EducatorsDruga DanutNo ratings yet
- PowerBI Interview Questions and AnswersDocument8 pagesPowerBI Interview Questions and AnswersexbisNo ratings yet
- Doterra Pasttense Essential Oil BlendDocument1 pageDoterra Pasttense Essential Oil BlendAlexandru Eduard RotaruNo ratings yet
- Autism DyslexiaDocument2 pagesAutism DyslexiaAutismDyslexiaNo ratings yet
- BEAT AUTISM NOW (BAN) - Booklet 1 – Logically, effectively and inexpensivelyFrom EverandBEAT AUTISM NOW (BAN) - Booklet 1 – Logically, effectively and inexpensivelyNo ratings yet
- Asd-Biomedical Treatments Research EssayDocument5 pagesAsd-Biomedical Treatments Research Essayapi-526505312No ratings yet
- Language Disorder: English Language and Literature Humanities Faculty Jenderal Soedirman University Purwokerto 2016Document12 pagesLanguage Disorder: English Language and Literature Humanities Faculty Jenderal Soedirman University Purwokerto 2016widya khNo ratings yet
- Autism AmishDocument2 pagesAutism AmishPower one100% (1)
- Autism X - ChromosomeDocument190 pagesAutism X - ChromosomeDanciu CristinaNo ratings yet
- AUTISMDocument18 pagesAUTISMNycoNo ratings yet
- Caroline - Walrad - The Autistic Spectrum NotesDocument14 pagesCaroline - Walrad - The Autistic Spectrum Notesnamkay_tenzynNo ratings yet
- Autism Metabolism, Mitochondria, and The MicrobiomeDocument15 pagesAutism Metabolism, Mitochondria, and The MicrobiomeJorge AlvesNo ratings yet
- Risk Factors, Diagnosis, Prognosis and Treatment of AutismDocument36 pagesRisk Factors, Diagnosis, Prognosis and Treatment of AutismCarlos Peña PaterninaNo ratings yet
- Autism and AirportDocument76 pagesAutism and AirportNoraz CompanyNo ratings yet
- Protocols by Resham Malhotra PDFDocument7 pagesProtocols by Resham Malhotra PDFScience NerdNo ratings yet
- Autism Spectrum Disorders in Extremely Preterm Children OriginalDocument9 pagesAutism Spectrum Disorders in Extremely Preterm Children Originalesteban_falcón_12No ratings yet
- Emily Iland Webinar With Autism NOW September 6, 2011Document36 pagesEmily Iland Webinar With Autism NOW September 6, 2011The Autism NOW CenterNo ratings yet
- Diet Texture Progression For Individuals With Autism ASHADocument81 pagesDiet Texture Progression For Individuals With Autism ASHAjhebetaNo ratings yet
- High Rates of Autism Found in Federal Vaccine Injury ProgramDocument4 pagesHigh Rates of Autism Found in Federal Vaccine Injury ProgramTyrone PenningNo ratings yet
- Increasing Speech SouIncreasing Speech Sound Production of Children With Autisnd Production of Children With AutismDocument34 pagesIncreasing Speech SouIncreasing Speech Sound Production of Children With Autisnd Production of Children With AutismPrapanit PntNo ratings yet
- Autism and EpilepsyDocument9 pagesAutism and EpilepsyTessa CruzNo ratings yet
- Autism SchoolDocument5 pagesAutism SchoolBhuvanesh Krishnan100% (1)
- UNCC 300 Assess 2Document2 pagesUNCC 300 Assess 2Usman Farooq100% (1)
- Genetic Causes of Syndromic and Non-Syndromic Autism PDFDocument9 pagesGenetic Causes of Syndromic and Non-Syndromic Autism PDFRaisa CoppolaNo ratings yet
- Angelman SyndromeDocument13 pagesAngelman Syndromeapi-388959318No ratings yet
- Asperger Syndrome SymptomsDocument8 pagesAsperger Syndrome Symptomsapi-277147828No ratings yet
- Autism, Recovery (To Normalcy) ,'' and The Politics of HopeDocument19 pagesAutism, Recovery (To Normalcy) ,'' and The Politics of HopeadhortizNo ratings yet
- Autism Resources: Information For FamiliesDocument1 pageAutism Resources: Information For FamiliesDesislava PeevaNo ratings yet
- Autism Therapy PresentationDocument13 pagesAutism Therapy Presentationapi-339989348No ratings yet
- Brain FogDocument9 pagesBrain FogIsmailNo ratings yet
- O o o o O: Assessment For IdentificationDocument9 pagesO o o o O: Assessment For IdentificationJong Suk Joo (Shuru)No ratings yet
- Specific Language ImpairmentDocument106 pagesSpecific Language ImpairmentKUNNAMPALLIL GEJO JOHNNo ratings yet
- The Impacts of Autism On The FamilyDocument4 pagesThe Impacts of Autism On The FamilyRuth Arcibal RomeroNo ratings yet
- Speech and Language Impairments in Children: Causes, Characteristics, Intervention and OutcomeDocument17 pagesSpeech and Language Impairments in Children: Causes, Characteristics, Intervention and OutcomeCelu CeluNo ratings yet
- Autism Spectrum and Open-MindednessDocument2 pagesAutism Spectrum and Open-MindednessJaime MontoyaNo ratings yet
- Measuring Television AddictionDocument24 pagesMeasuring Television Addictionciprian72100% (1)
- Restricted and Repetitive Behaviors As Strengths Not WeaknessesDocument213 pagesRestricted and Repetitive Behaviors As Strengths Not WeaknessesTomas Torres BarberoNo ratings yet
- Sensory Storytime How-To GuideDocument4 pagesSensory Storytime How-To GuideSaidJanNo ratings yet
- Listen, Screen & Recognize The Red Flags For Autism Spectrum DisordersDocument28 pagesListen, Screen & Recognize The Red Flags For Autism Spectrum DisordersThe Autism NOW CenterNo ratings yet
- AutismDocument34 pagesAutismSrm Genetics100% (1)
- Effects of A Brief Early Start Denver Model (ESDM) - Based Parent Intervention On Toddlers at Risk For Autism Spectrum Disorders A Randomized Controlled TrialDocument14 pagesEffects of A Brief Early Start Denver Model (ESDM) - Based Parent Intervention On Toddlers at Risk For Autism Spectrum Disorders A Randomized Controlled TrialLuis Seixas100% (1)
- Classification of Feeding and Eating DisordersDocument13 pagesClassification of Feeding and Eating DisordersMagito JayaNo ratings yet
- Behavioral Treatment and Normal Educational and Intellectual Functioning in /bung Autistic ChildrenDocument7 pagesBehavioral Treatment and Normal Educational and Intellectual Functioning in /bung Autistic ChildrenMariaNo ratings yet
- The Spectrum of Mitochondrial Disease Ep-3-10Document8 pagesThe Spectrum of Mitochondrial Disease Ep-3-10F4AR100% (1)
- Autism-Strategies For CommunicationDocument21 pagesAutism-Strategies For CommunicationMs.Aishwarya Nallamuthu, Dept. of SLHS, SRIHERNo ratings yet
- What Is AutismDocument4 pagesWhat Is Autismidno1008No ratings yet
- ASD Recovery 2019Document5 pagesASD Recovery 2019verdantlaw100% (1)
- Lovaas BookDocument338 pagesLovaas BooklicheiNo ratings yet
- Autism and EpilepsyDocument5 pagesAutism and Epilepsyclarajimena25No ratings yet
- Childhood DisordersDocument7 pagesChildhood DisordersApOlle Defiesta - DOminguezNo ratings yet
- InTech-Sensory Motor Development in AutismDocument26 pagesInTech-Sensory Motor Development in AutismTânia DiasNo ratings yet
- Promoting Healthy Eating Behaviors in A Safe and Supportive Environment For ChildrenDocument7 pagesPromoting Healthy Eating Behaviors in A Safe and Supportive Environment For Childrenapi-604622509No ratings yet
- Analysis and Evaluation of ASD TheoriesDocument9 pagesAnalysis and Evaluation of ASD Theoriestracycw100% (1)
- Research Supporting DIRDocument6 pagesResearch Supporting DIRsegurryNo ratings yet
- Sexual Recovery Institute - Summer & Fall Saturday Lecture SeriesDocument2 pagesSexual Recovery Institute - Summer & Fall Saturday Lecture SeriesSexRecoveryNo ratings yet
- How To Change Connections in Portfolio Slicer For Power BI Desktop Model - Portfolio SlicerDocument4 pagesHow To Change Connections in Portfolio Slicer For Power BI Desktop Model - Portfolio SlicerexbisNo ratings yet
- Demystifying Chart Types and Design Principles in Power BIDocument61 pagesDemystifying Chart Types and Design Principles in Power BIexbisNo ratings yet
- Power Bi Data Viz Usability Checklist2Document5 pagesPower Bi Data Viz Usability Checklist2exbisNo ratings yet
- So You Want To Be A Business Intelligence (BI) DeveloperDocument5 pagesSo You Want To Be A Business Intelligence (BI) DeveloperexbisNo ratings yet
- Power BI Assessment Dashboard WalkthroughDocument35 pagesPower BI Assessment Dashboard WalkthroughexbisNo ratings yet
- Web Content: With The SQL Server 2008R2 PlatformDocument4 pagesWeb Content: With The SQL Server 2008R2 PlatformexbisNo ratings yet
- PASS - 19 - Corp - Template - v2 - IaaS - Vs - PaaS FinalDocument33 pagesPASS - 19 - Corp - Template - v2 - IaaS - Vs - PaaS FinalexbisNo ratings yet
- Business Intelligence Requirements GatheringDocument2 pagesBusiness Intelligence Requirements GatheringexbisNo ratings yet
- Tracking Data Changes: With Temporal Tables and MoreDocument22 pagesTracking Data Changes: With Temporal Tables and MoreexbisNo ratings yet
- Company Jobtitle Startdate EnddateDocument18 pagesCompany Jobtitle Startdate EnddateexbisNo ratings yet
- Using Ssas 2005 As Ds For Power PivotDocument1 pageUsing Ssas 2005 As Ds For Power PivotexbisNo ratings yet
- Different Types of ForEachLoop EnumeratorDocument38 pagesDifferent Types of ForEachLoop EnumeratorexbisNo ratings yet
- 22 SQL For ModelingDocument51 pages22 SQL For ModelingexbisNo ratings yet
- Multidimensional ModelingDocument12 pagesMultidimensional ModelingexbisNo ratings yet
- Using SSAS 2005 As DS - Calculated MembersDocument4 pagesUsing SSAS 2005 As DS - Calculated MembersexbisNo ratings yet
- Migrating Content Between Report ServersDocument14 pagesMigrating Content Between Report ServersexbisNo ratings yet
- Chart Suggestions - A Thought-StarterDocument1 pageChart Suggestions - A Thought-StarterDoc AllaínNo ratings yet
- Wanna Be A SQL ConsultantDocument20 pagesWanna Be A SQL ConsultantexbisNo ratings yet
- Checklist For Ssas Tabular Model DevelopmentDocument1 pageChecklist For Ssas Tabular Model DevelopmentexbisNo ratings yet
- PL SQL Interview - Career Ride - ImpDocument392 pagesPL SQL Interview - Career Ride - ImpexbisNo ratings yet
- Mesenchymal Stem Cell-Conditioned Medium (Secretome) in Skin Aging A Systematic ReviewDocument24 pagesMesenchymal Stem Cell-Conditioned Medium (Secretome) in Skin Aging A Systematic ReviewThomas UtomoNo ratings yet
- Greenland 2256 2513 6Document258 pagesGreenland 2256 2513 6seacoastonlineNo ratings yet
- Pharm Calcium Channel Blockers (Bahar&Amy) "Vera Dialed The Calcium Channel To Buy A Knife" Verapramil, Diltizaem, NifedipineDocument7 pagesPharm Calcium Channel Blockers (Bahar&Amy) "Vera Dialed The Calcium Channel To Buy A Knife" Verapramil, Diltizaem, Nifedipinecherrybombaz100% (4)
- Apical Canal ConfuencyDocument7 pagesApical Canal ConfuencyPanxo14No ratings yet
- Comprehensive List of American and British Spelling DifferencesDocument36 pagesComprehensive List of American and British Spelling DifferencesshivaNo ratings yet
- Dams Lastlook Microbiology PDFDocument27 pagesDams Lastlook Microbiology PDFChauhan Monika100% (1)
- Asparaginase / Erwinia AsparaginaseDocument10 pagesAsparaginase / Erwinia AsparaginaseMohammed HaiderNo ratings yet
- Bench-To-bedside Review An Approach To Hemodynamic Monitoring Guyton at Bedside - Magder 2012Document7 pagesBench-To-bedside Review An Approach To Hemodynamic Monitoring Guyton at Bedside - Magder 2012Fransisca Dewi KumalaNo ratings yet
- Nursing LeadershipDocument6 pagesNursing LeadershipAyanne03No ratings yet
- Dermoneuromodulation Rev 03Document57 pagesDermoneuromodulation Rev 03dasamoro100% (1)
- Ophthalmonics 1st EditionDocument116 pagesOphthalmonics 1st Editiondhavalb2086% (7)
- Volume 2 GDVs and More - Rev1 Ed6jvjDocument39 pagesVolume 2 GDVs and More - Rev1 Ed6jvjErhan ErtuçNo ratings yet
- PR 1Document47 pagesPR 1Daniel MagcalasNo ratings yet
- September 26, 2018 by Sagar Aryal: Antigen-Properties, Types and Determinants of AntigenicityDocument23 pagesSeptember 26, 2018 by Sagar Aryal: Antigen-Properties, Types and Determinants of AntigenicityEzekiel GantiedNo ratings yet
- CANINE-Canine Transfusion Reactions - Part 2.prevention and TreatmentDocument7 pagesCANINE-Canine Transfusion Reactions - Part 2.prevention and Treatmenttaner_soysurenNo ratings yet
- 6 Yoga Poses You Can Do in Bed Before Sleeping For Better Health PDFDocument21 pages6 Yoga Poses You Can Do in Bed Before Sleeping For Better Health PDFAsfaq SumraNo ratings yet
- Vivir Con ParkinsonDocument22 pagesVivir Con ParkinsonAlexis Muñoz TrincadoNo ratings yet
- Water Electrolytes Part Clinical BiochemistryDocument27 pagesWater Electrolytes Part Clinical BiochemistryAshraf FirdadNo ratings yet
- Afi48 123Document192 pagesAfi48 123nazario1719011No ratings yet
- Mapeh Department: Daily Lesson PlanDocument8 pagesMapeh Department: Daily Lesson PlanJessie FranciscoNo ratings yet
- Nutraceuticals: April 2016Document9 pagesNutraceuticals: April 2016nikita bindakNo ratings yet
- Important Drug Nutrient Interactions: Pamela MasonDocument35 pagesImportant Drug Nutrient Interactions: Pamela MasonRijantono Franciscus MariaNo ratings yet
- KariesDocument4 pagesKariesSherlocknovNo ratings yet
- Care of Low Birth Weight BabiesDocument102 pagesCare of Low Birth Weight Babiesvarshasharma050% (2)
- A Countdown To Orthognathic SurgeryDocument5 pagesA Countdown To Orthognathic SurgeryhaneefmdfNo ratings yet
- Autism - Gender and GeneticsDocument12 pagesAutism - Gender and GeneticsAggrey SmartfieldNo ratings yet
- MIT 9.00 Exam 1 2007 AnswersDocument16 pagesMIT 9.00 Exam 1 2007 AnswersbitternessinmymouthNo ratings yet
- Ethics Assignment Sem 3Document9 pagesEthics Assignment Sem 3api-314566363No ratings yet
- Zeway ReportDocument8 pagesZeway Reportbereket rikitaNo ratings yet