Download as docx, pdf, or txt
You might also like
- Full Download Solution Manual For Holes Human Anatomy Physiology 16th Edition Charles Welsh Cynthia Prentice Craver PDF Full ChapterDocument36 pagesFull Download Solution Manual For Holes Human Anatomy Physiology 16th Edition Charles Welsh Cynthia Prentice Craver PDF Full Chaptertracikennedyvw3z8d100% (23)
- 30-Second Anatomy: The 50 most important structures and systems in the human body each explained in under half a minuteFrom Everand30-Second Anatomy: The 50 most important structures and systems in the human body each explained in under half a minuteRating: 2.5 out of 5 stars2.5/5 (2)
- Masterplan TemplateDocument72 pagesMasterplan TemplateMostafa FawzyNo ratings yet
- Spss 1Document2 pagesSpss 1DebiNo ratings yet
- Category: Grading Rubric For Storyboard ProjectDocument1 pageCategory: Grading Rubric For Storyboard ProjectRyan EstonioNo ratings yet
- Edit Source Editbeta: Constituents of The Human Body Constituent Weight Percent of AtomsDocument13 pagesEdit Source Editbeta: Constituents of The Human Body Constituent Weight Percent of AtomsRanbir SinghNo ratings yet
- Human BodyDocument27 pagesHuman BodyRanbir Singh100% (1)
- Physical EducationDocument2 pagesPhysical EducationPRINTDESK by DanNo ratings yet
- Anaphysio Lab Exercises 1Document5 pagesAnaphysio Lab Exercises 1Juan Miguel SalvadorNo ratings yet
- About Human BodyDocument16 pagesAbout Human BodyApril Lavenia BarrientosNo ratings yet
- EC2021 Medical Electronics Notes For AllDocument99 pagesEC2021 Medical Electronics Notes For All6025 MOHAMMED THAJUDEEN R GCE TJ II ECENo ratings yet
- Basic A&p Booklet Short Version 3Document228 pagesBasic A&p Booklet Short Version 3Hilary Christopher100% (1)
- TSC Study Material EditedDocument128 pagesTSC Study Material EditedNaina ShendeNo ratings yet
- Solution Manual For Holes Human Anatomy Physiology 16th Edition Charles Welsh Cynthia Prentice CraverDocument36 pagesSolution Manual For Holes Human Anatomy Physiology 16th Edition Charles Welsh Cynthia Prentice Cravertroul.cubit.nwjkgf100% (44)
- Human Body'S Systems: Circulatory SystemDocument24 pagesHuman Body'S Systems: Circulatory SystemsrathinakumarNo ratings yet
- Textos I Medicina Level I 2020Document18 pagesTextos I Medicina Level I 2020Valeria DonzelliNo ratings yet
- MyBodyMySenses PrintDocument68 pagesMyBodyMySenses PrintnicoletagrNo ratings yet
- Activity of The 1st SessionDocument11 pagesActivity of The 1st SessionShaneNo ratings yet
- Physical EducationDocument8 pagesPhysical EducationChristianLouisNoquisNo ratings yet
- What Is AnatomyDocument14 pagesWhat Is AnatomyRina Hayatun NufusNo ratings yet
- Asia Pacific College of Advanced Studies, Inc.: City of Balanga, BataanDocument13 pagesAsia Pacific College of Advanced Studies, Inc.: City of Balanga, Bataan속강대No ratings yet
- W2 - Human BodyDocument11 pagesW2 - Human BodyNella Riznanda RachmadantiNo ratings yet
- Pathfit 1 Chapter 2 Introduction To AnatomyDocument20 pagesPathfit 1 Chapter 2 Introduction To AnatomyadamigzhylynNo ratings yet
- Health Information Part 7Document24 pagesHealth Information Part 7TimothyNo ratings yet
- Unit 1 Study GuideDocument4 pagesUnit 1 Study GuideNic Alcala100% (1)
- Systems of Human BodyDocument13 pagesSystems of Human BodyMahesh BabuNo ratings yet
- Parts and Functions of The Circulatory SystemDocument12 pagesParts and Functions of The Circulatory SystemKristine Joy JaroNo ratings yet
- Anatomy and Physiology Lecture Notes Sevilla C. Yobueno, Ph.D. SPAMAST Malita Campus I. Cells, Tissues and MembranesDocument5 pagesAnatomy and Physiology Lecture Notes Sevilla C. Yobueno, Ph.D. SPAMAST Malita Campus I. Cells, Tissues and MembranesReuben EscarlanNo ratings yet
- List of Human Body Parts With DiagramDocument13 pagesList of Human Body Parts With DiagramPankaj Pandya100% (1)
- Anatomy Exploring The Human BodyDocument15 pagesAnatomy Exploring The Human BodyZack Aarton100% (2)
- Brain Anatomy and FunctionDocument24 pagesBrain Anatomy and FunctionAdamu GudinaNo ratings yet
- Textos I, Kinesio, Instr. Q. Level I '20Document9 pagesTextos I, Kinesio, Instr. Q. Level I '20Valeria DonzelliNo ratings yet
- The Human Body Is A Complex SystemDocument6 pagesThe Human Body Is A Complex SystemGabriela BrardaNo ratings yet
- Anatomy Powerpoint 23Document188 pagesAnatomy Powerpoint 23Abdihamid Sheikh DaudNo ratings yet
- Class 5 - Science Chapter 3Document18 pagesClass 5 - Science Chapter 3deviNo ratings yet
- EpithelialDocument8 pagesEpithelialRushyl Angela FaeldanNo ratings yet
- Unit 7: Anatomy: Excerpt From A LectureDocument4 pagesUnit 7: Anatomy: Excerpt From A LectureAnonymous Wfl201YbYoNo ratings yet
- 3k221273 - M Syahreza A - Mid InggrisDocument7 pages3k221273 - M Syahreza A - Mid InggrisFirman KurniawanNo ratings yet
- Lecture 1 CHAPTER ONE INTRODUCTION TO HUMAN ANATOMY AND PHYSIOLOGYDocument10 pagesLecture 1 CHAPTER ONE INTRODUCTION TO HUMAN ANATOMY AND PHYSIOLOGYAsharAnisNo ratings yet
- Y6 Being HumanDocument2 pagesY6 Being Humansadviau3No ratings yet
- SHANEDocument8 pagesSHANERomlen Ramiro OrtegaNo ratings yet
- Partes Del CuerpoDocument9 pagesPartes Del CuerpoArgenis SurielNo ratings yet
- Human ScienceDocument8 pagesHuman ScienceOscar MasindeNo ratings yet
- Ch.7 NotesDocument8 pagesCh.7 NotesMohd ShaikhNo ratings yet
- Human Anatomy and PhysiologyDocument123 pagesHuman Anatomy and PhysiologyWilliamMindoro100% (2)
- Human Body Anatomy Bahasa Inggris SalinanDocument21 pagesHuman Body Anatomy Bahasa Inggris SalinanDina LestariNo ratings yet
- Duty Human Anatomy and PhysiologiDocument8 pagesDuty Human Anatomy and PhysiologiSumiati FranNo ratings yet
- Why Human Beings Are Considered Complex Organisms Group 5Document37 pagesWhy Human Beings Are Considered Complex Organisms Group 5Nuraini Zul100% (3)
- Holy Child Colleges of ButuanDocument8 pagesHoly Child Colleges of ButuanJoseph Mark Ocampo ArtiagaNo ratings yet
- The-Immune-System Vitamins Minerals Sir-FlemingDocument5 pagesThe-Immune-System Vitamins Minerals Sir-FlemingD IngaNo ratings yet
- Co2 Lesson 1.1 Human Anatomy Week 4Document10 pagesCo2 Lesson 1.1 Human Anatomy Week 4accfor everythingNo ratings yet
- Introduction To Human Anatomy and PhysiologyDocument42 pagesIntroduction To Human Anatomy and PhysiologyDump Acc 2100% (1)
- JSS2 Basic Science Lesson Note PDFDocument40 pagesJSS2 Basic Science Lesson Note PDFJuddy ScienceNo ratings yet
- The Human Body SystemsDocument5 pagesThe Human Body SystemsSaurav AcharyaNo ratings yet
- P.E Anatomical TermsDocument26 pagesP.E Anatomical TermsGerald Mapalo FactorNo ratings yet
- Module 1 INTRODUCTIONDocument7 pagesModule 1 INTRODUCTIONMisha WilliamsNo ratings yet
- Human Body DR MellaliDocument20 pagesHuman Body DR MellaliSarah MellaliNo ratings yet
- Human OrganDocument3 pagesHuman OrganAdrian AgujeroNo ratings yet
- Deciphering nCoV19, Quest for Cure, Prophylaxis, and VaccineFrom EverandDeciphering nCoV19, Quest for Cure, Prophylaxis, and VaccineNo ratings yet
- The Human Body: The Facts Book for Future Doctors - Biology Books for Kids | Children's Biology BooksFrom EverandThe Human Body: The Facts Book for Future Doctors - Biology Books for Kids | Children's Biology BooksNo ratings yet
- Data Base Hands OnDocument5 pagesData Base Hands OnMichaelAngeloDelaCruzNo ratings yet
- Report Feasibility WordDocument7 pagesReport Feasibility WordMichaelAngeloDelaCruzNo ratings yet
- Computer Department: Rizal Technological University College of Engineering and Industrial TechnologyDocument2 pagesComputer Department: Rizal Technological University College of Engineering and Industrial TechnologyMichaelAngeloDelaCruzNo ratings yet
- Marriott CS-MNL - Access UAT - Wave3Document2 pagesMarriott CS-MNL - Access UAT - Wave3MichaelAngeloDelaCruzNo ratings yet
- Osgood-Schramm Model of Communication: in Communication Models, Interpersonal CommunicationDocument2 pagesOsgood-Schramm Model of Communication: in Communication Models, Interpersonal CommunicationMichaelAngeloDelaCruzNo ratings yet
- Pollero, Pamela E. What Is The Importance of Studying Movement Enhancement?Document2 pagesPollero, Pamela E. What Is The Importance of Studying Movement Enhancement?MichaelAngeloDelaCruzNo ratings yet
- General Terms and Conditions As of October 17 2018Document5 pagesGeneral Terms and Conditions As of October 17 2018MichaelAngeloDelaCruzNo ratings yet
- 2N3055 (NPN), MJ2955 (PNP) Complementary Silicon Power TransistorsDocument3 pages2N3055 (NPN), MJ2955 (PNP) Complementary Silicon Power TransistorsMichaelAngeloDelaCruzNo ratings yet
- ICEfaces Asynchronous HTTP ServerDocument33 pagesICEfaces Asynchronous HTTP ServerIniyaNo ratings yet
- Arts 8Document34 pagesArts 8Joanna joannaNo ratings yet
- Gas Supply Agreement 148393.1Document5 pagesGas Supply Agreement 148393.1waking_days100% (1)
- En 288 377Document90 pagesEn 288 377Vitaliy KlimenkoNo ratings yet
- 1 s2.0 S0160738323001846 MainDocument4 pages1 s2.0 S0160738323001846 Mainussual humanNo ratings yet
- Pythagoras' Theorem: HapterDocument13 pagesPythagoras' Theorem: HapterBunga NoionlaNo ratings yet
- CHN Transes Week 1Document5 pagesCHN Transes Week 1cheskalyka.asiloNo ratings yet
- Information Booklet Awards Day 2012Document16 pagesInformation Booklet Awards Day 2012kartytyNo ratings yet
- Chemical Analysis of Caustic Soda and Caustic Potash (Sodium Hydroxide and Potassium Hydroxide)Document16 pagesChemical Analysis of Caustic Soda and Caustic Potash (Sodium Hydroxide and Potassium Hydroxide)wilfred gomezNo ratings yet
- 86% Strike - 97% Stop Loss - 2 Months - EUR: Bullish Mini-Futures On The German Stock Index Future of June 2010Document1 page86% Strike - 97% Stop Loss - 2 Months - EUR: Bullish Mini-Futures On The German Stock Index Future of June 2010api-25889552No ratings yet
- Chapter IIIDocument3 pagesChapter IIIRenan S. GuerreroNo ratings yet
- Project Report On Customer Satisfaction Towards LGDocument52 pagesProject Report On Customer Satisfaction Towards LGrajasekar100% (2)
- Edmentum TrainingDocument20 pagesEdmentum Trainingapi-557217750No ratings yet
- 9.3.4 Packet Tracer IPv6 Neighbor Discovery AnsDocument6 pages9.3.4 Packet Tracer IPv6 Neighbor Discovery Ansssf 2018No ratings yet
- PUSTAK SOOCHI 15 Pages 2022Document16 pagesPUSTAK SOOCHI 15 Pages 2022राहुल चाहरNo ratings yet
- Reviewer in Machine ShorthandDocument6 pagesReviewer in Machine ShorthandChristian CuberoNo ratings yet
- Psychoanalysis: ArticleDocument21 pagesPsychoanalysis: ArticleAqsa ParveenNo ratings yet
- M-Sand in Tamil NaduDocument9 pagesM-Sand in Tamil Nadurameshkanu1No ratings yet
- Portfolio Isaac B 1Document17 pagesPortfolio Isaac B 1api-690889230No ratings yet
- Monteverdi Clorinda e TancrediDocument19 pagesMonteverdi Clorinda e TancrediFelipeCussenNo ratings yet
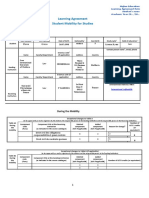
- Learning Agreement During The MobilityDocument3 pagesLearning Agreement During The MobilityVictoria GrosuNo ratings yet
- Vivo Placement Papers PDF Download PDFDocument28 pagesVivo Placement Papers PDF Download PDFNikhil VermaNo ratings yet
- PAS 28 - Investments in Associates and Joint Ventures-1Document12 pagesPAS 28 - Investments in Associates and Joint Ventures-1Krizzia DizonNo ratings yet
- TarzanDocument2 pagesTarzanmaris quilantangNo ratings yet
- Prepositions After AdjectivesDocument2 pagesPrepositions After AdjectivesJosé María OrtigueiraNo ratings yet
- ATPAR ReviewerDocument25 pagesATPAR ReviewerJohn Paul BuliyatNo ratings yet
- Unit 10: Sitcom: Tonight, I'm CookingDocument3 pagesUnit 10: Sitcom: Tonight, I'm CookingDaissy FonsecaNo ratings yet