
Emerging Risk Factors For CAD - PDF
Emerging Risk Factors For CAD - PDF
You might also like
- Risk Factors & Prognosis For USMLE STEP 3 PDFDocument182 pagesRisk Factors & Prognosis For USMLE STEP 3 PDFSadia GhaniNo ratings yet
- Dyslipidemia MXDocument72 pagesDyslipidemia MXsruthimeena6891No ratings yet
- Chronic Kidney Disease and Its ComplicationsDocument6 pagesChronic Kidney Disease and Its ComplicationsmedicalNo ratings yet
- Primary Prevention of CVDDocument53 pagesPrimary Prevention of CVDYibeltal AssefaNo ratings yet
- Δείκτες φλεγμονήςDocument48 pagesΔείκτες φλεγμονήςeliotkanNo ratings yet
- High Sensitivity CRPDocument10 pagesHigh Sensitivity CRPChrishan ShivanthanNo ratings yet
- Leo Atp IvDocument25 pagesLeo Atp IvLeonardo MedinaNo ratings yet
- Low-Density Lipoprotein Cholesterol and Stroke: How Low Should We Go?Document3 pagesLow-Density Lipoprotein Cholesterol and Stroke: How Low Should We Go?pitiwararom rachtipatNo ratings yet
- Journal Presentation 1Document61 pagesJournal Presentation 1Shalini RachaNo ratings yet
- AtherosclerosisDocument29 pagesAtherosclerosisneeraj banaNo ratings yet
- Coronary Heart Disease Risk Factors Among UniversiDocument6 pagesCoronary Heart Disease Risk Factors Among UniversiMuhammad Irfan JamilNo ratings yet
- Article 164163-PrintDocument22 pagesArticle 164163-PrintIribuka JonathanNo ratings yet
- Dyslipidemia Guidelines Presentation v2Document39 pagesDyslipidemia Guidelines Presentation v2avicennaxNo ratings yet
- Cardiovascular Complication in CKD 28.8.18Document65 pagesCardiovascular Complication in CKD 28.8.18Hemanth PrakashNo ratings yet
- Abstract and IntroductionDocument14 pagesAbstract and Introductiondavid_lg6179No ratings yet
- Case Study 2 MNTDocument11 pagesCase Study 2 MNTapi-242547654No ratings yet
- Raza2004 PDFDocument12 pagesRaza2004 PDFIvana RuseskaNo ratings yet
- Atherosclerosis, Dyslipidaemia and Diabetes SlidesDocument83 pagesAtherosclerosis, Dyslipidaemia and Diabetes SlidesTatiana GobjilăNo ratings yet
- Association of Hypertriglyceridemia With Ischemic Stroke, Study in A Tertiary Care Hospital in BangladeshDocument6 pagesAssociation of Hypertriglyceridemia With Ischemic Stroke, Study in A Tertiary Care Hospital in BangladeshRay HannaNo ratings yet
- 1996 USPSTF High Blood Cholesterol and Other Lipid Abnormalities ScreeningDocument24 pages1996 USPSTF High Blood Cholesterol and Other Lipid Abnormalities ScreeningScott LinNo ratings yet
- Cardiovascular Disorders: Annette HaynesDocument69 pagesCardiovascular Disorders: Annette HaynesBinh Yen Quach TranNo ratings yet
- Original Article Evaluation of Dyslipidaemia in Type 2 Diabetes Mellitus PatientsDocument6 pagesOriginal Article Evaluation of Dyslipidaemia in Type 2 Diabetes Mellitus PatientsEnvhy AmaliaNo ratings yet
- Hiperlipidemia 1-Indah 2017Document16 pagesHiperlipidemia 1-Indah 2017Meg Meg Mega DwiNo ratings yet
- Ischemic Stroke: Prevention Cardioembolism Revascularisation Procedures Stroke in Special CircumstancesDocument24 pagesIschemic Stroke: Prevention Cardioembolism Revascularisation Procedures Stroke in Special Circumstancesnisha24100% (1)
- IncidenceDocument3 pagesIncidenceapi-26340035100% (1)
- 23 Preventive Heart Disease, Dyslipidemia and HTNDocument13 pages23 Preventive Heart Disease, Dyslipidemia and HTNVictor PazNo ratings yet
- Hypertriglyceridemia As A Possible Independent Risk Factor For StrokeDocument6 pagesHypertriglyceridemia As A Possible Independent Risk Factor For StrokeFilbert WashingtonNo ratings yet
- Cardiac Biomarkers: Cardiac Enzymes and BiomarkerDocument21 pagesCardiac Biomarkers: Cardiac Enzymes and Biomarkeranamika sharmaNo ratings yet
- South African Dyslipedemia GuidelineDocument11 pagesSouth African Dyslipedemia Guidelinesmaug_11No ratings yet
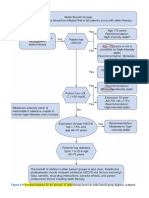
- Recommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (AdaptedDocument8 pagesRecommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (Adaptedعزالدين الطيارNo ratings yet
- AtherosclerosisDocument9 pagesAtherosclerosisSharmila SeeralanNo ratings yet
- Coronary Calcium ScoreDocument49 pagesCoronary Calcium ScoreBinod KumarNo ratings yet
- High Sensitivity C-Reactive ProteinDocument100 pagesHigh Sensitivity C-Reactive ProteinFast ComposersNo ratings yet
- Pharmacology & Therapeutics: Anette Varbo, Marianne Benn, Børge G. NordestgaardDocument10 pagesPharmacology & Therapeutics: Anette Varbo, Marianne Benn, Børge G. NordestgaardIonuț CozmaNo ratings yet
- Lipoprotein Paper Academia ZaragedDocument29 pagesLipoprotein Paper Academia Zaragedpawovem755No ratings yet
- Predictive Mortality Risk Factors in Diabetes MellitusDocument6 pagesPredictive Mortality Risk Factors in Diabetes MellitusblueiceNo ratings yet
- Hyper Cholesterol Emi ADocument7 pagesHyper Cholesterol Emi AMohamed EssallaaNo ratings yet
- Diretriz - Dislipidemia EndocrinologiaDocument70 pagesDiretriz - Dislipidemia EndocrinologiaSamara QueirozNo ratings yet
- Dyson LineDocument10 pagesDyson LineSharly DwijayantiNo ratings yet
- Efficacy and Safety of High-Density Lipoprotein Cholesterol-Increasing CompoundsDocument13 pagesEfficacy and Safety of High-Density Lipoprotein Cholesterol-Increasing CompoundsAdityasekar WangiNo ratings yet
- Polygenic HypercholesterolemiaDocument6 pagesPolygenic HypercholesterolemiaSamhitha Ayurvedic ChennaiNo ratings yet
- Coronary Artery DiseaseDocument80 pagesCoronary Artery Diseaseamelia pratiwiNo ratings yet
- C-Reactive Protein (CRP) : Erythrocyte Sedimentation Rate Blood Platelet CountDocument23 pagesC-Reactive Protein (CRP) : Erythrocyte Sedimentation Rate Blood Platelet Countikillyou1900No ratings yet
- Pharmacological Treatment of HyperlipiedmiaDocument8 pagesPharmacological Treatment of HyperlipiedmiajeffaguilarNo ratings yet
- Dyslipidemia Management in Women and Men: Exploring Potential Gender DifferencesDocument7 pagesDyslipidemia Management in Women and Men: Exploring Potential Gender DifferencesAmelie AnsonNo ratings yet
- 2013 ACC/AHA Guideline On The Treatment of Blood Cholesterol To Reduce Atherosclerotic Cardiovascular Risk in AdultsDocument37 pages2013 ACC/AHA Guideline On The Treatment of Blood Cholesterol To Reduce Atherosclerotic Cardiovascular Risk in AdultsIman SaksoukNo ratings yet
- Dyslipidemia Guidelines Feb2010 PDFDocument4 pagesDyslipidemia Guidelines Feb2010 PDFImam Rosyada RijalulhaqNo ratings yet
- Diagnostic Tests and ProceduresDocument49 pagesDiagnostic Tests and Procedurespmahi8854No ratings yet
- Dyslipidemia: Signs and SymptomsDocument24 pagesDyslipidemia: Signs and Symptomschrissanto chandraNo ratings yet
- Association Between Lipid Fractions and Age of First Myocardial InfarctionDocument7 pagesAssociation Between Lipid Fractions and Age of First Myocardial InfarctionAnonymous plYGwXNo ratings yet
- Medical TerminologyDocument17 pagesMedical TerminologySofia Isabelle GarciaNo ratings yet
- Li 2017Document32 pagesLi 2017akshayNo ratings yet
- MR Sayan Project (Hyperkalemia in CKD Patient) PDFDocument27 pagesMR Sayan Project (Hyperkalemia in CKD Patient) PDFManjurul RahamanNo ratings yet
- Inborn Errors of Lipid MetabolismDocument41 pagesInborn Errors of Lipid MetabolismWalterNo ratings yet
- ehab771-2Document3 pagesehab771-2andresadarvegNo ratings yet
- 8 Meq/L PH 7.2) May Require Iv Therapy (See Chap. 51) .: Evaluation of Therapeutic OutcomesDocument2 pages8 Meq/L PH 7.2) May Require Iv Therapy (See Chap. 51) .: Evaluation of Therapeutic OutcomesDebbyNovriozaNo ratings yet
- Optimalmedicaltherapyfor Stableischemicheart Diseasein2024: Focus On Blood Pressure and LipidsDocument13 pagesOptimalmedicaltherapyfor Stableischemicheart Diseasein2024: Focus On Blood Pressure and LipidsCarlos Hernan Castañeda RuizNo ratings yet
- Clinical Surgery Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2From EverandClinical Surgery Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2No ratings yet
- Textbook of Pediatrics, 18th Edition. Philadelphia: Elsevier Inc 2007Document1 pageTextbook of Pediatrics, 18th Edition. Philadelphia: Elsevier Inc 2007dinnhanifahNo ratings yet
- Daftar Pustaka: Biotechnology. 27 (5) : 427-433Document8 pagesDaftar Pustaka: Biotechnology. 27 (5) : 427-433dinnhanifahNo ratings yet
- Textbook of Pediatrics, 18th Edition. Philadelphia: Elsevier Inc 2007Document1 pageTextbook of Pediatrics, 18th Edition. Philadelphia: Elsevier Inc 2007dinnhanifahNo ratings yet
- ACOG Practice Bulletin No 183 Postpartum-Hemorrhage-2017Document19 pagesACOG Practice Bulletin No 183 Postpartum-Hemorrhage-2017dinnhanifahNo ratings yet
- Bipolar in Kaplan & Sadock's Comprehensive Textbook of Psychiatry, 10Document2 pagesBipolar in Kaplan & Sadock's Comprehensive Textbook of Psychiatry, 10dinnhanifahNo ratings yet
- 971S FullDocument3 pages971S FulldinnhanifahNo ratings yet
- Collodion Baby: Presented byDocument10 pagesCollodion Baby: Presented byNoor AhamedNo ratings yet
- Transfusion Reaction PDFDocument1 pageTransfusion Reaction PDFKah Man GohNo ratings yet
- Adapted From Family Planning Competency-Based Training: Basic Course HandbookDocument4 pagesAdapted From Family Planning Competency-Based Training: Basic Course HandbookVanessa EnteroNo ratings yet
- Makalah Bahasa Inggris 2Document7 pagesMakalah Bahasa Inggris 2azizah LasimpalaNo ratings yet
- Pediatric Nursing Dissertation TopicsDocument8 pagesPediatric Nursing Dissertation TopicsCustomCollegePaperCanada100% (1)
- Medical & Homeopathic Research, Homeopathic Medical Collage and ResearchDocument145 pagesMedical & Homeopathic Research, Homeopathic Medical Collage and ResearchMitesh KinariwalaNo ratings yet
- Hemolytic Disease of NewbornDocument41 pagesHemolytic Disease of NewbornRaja100% (3)
- Ground FloorDocument1 pageGround FloorJeya AtharshikaNo ratings yet
- Palliative Care - End of Life Care - Northern HealthDocument8 pagesPalliative Care - End of Life Care - Northern HealthDiklatpimempat AngkatanlimabelasNo ratings yet
- GMP FinalDocument37 pagesGMP FinalekramNo ratings yet
- LP in Science 12 (Basic First Aid)Document9 pagesLP in Science 12 (Basic First Aid)Alvin Cabanela100% (1)
- Seasonal Affective Disorder StudyDocument7 pagesSeasonal Affective Disorder Studyvidro3No ratings yet
- ISlabDocument3 pagesISlabpixiedustNo ratings yet
- SR Diabetic Foot UlcerDocument11 pagesSR Diabetic Foot UlcerDeka AdeNo ratings yet
- Non-Pharmacological Treatment of HypertensionDocument25 pagesNon-Pharmacological Treatment of Hypertensionastrid abrahams0% (2)
- Summary of Benefits: Quartz Medicare Advantage (HMO), in Partnership With UW HealthDocument20 pagesSummary of Benefits: Quartz Medicare Advantage (HMO), in Partnership With UW HealthChris CoulmanNo ratings yet
- Quality and Safety in Compounding Non-Sterile PreparationsDocument5 pagesQuality and Safety in Compounding Non-Sterile PreparationsPruessada DeeyingNo ratings yet
- Nasal Lacrimal Duct ObstructionDocument2 pagesNasal Lacrimal Duct ObstructionAgitha Melita PutriNo ratings yet
- Venous ThromboembolismDocument11 pagesVenous ThromboembolismKrsna Navera100% (1)
- Pertanyaan JurnalDocument2 pagesPertanyaan JurnalodivarNo ratings yet
- Cavernous Sinus Thrombosis of Odontogenic Origin: March 2016Document8 pagesCavernous Sinus Thrombosis of Odontogenic Origin: March 2016Putu WidiastriNo ratings yet
- Contoh Naskah Presentasi KD 26Document3 pagesContoh Naskah Presentasi KD 26Kharisma Nur FajriyahNo ratings yet
- DNB Radio Diagnosis Paper1Document4 pagesDNB Radio Diagnosis Paper1Taha IsmailNo ratings yet
- Robert G. Gish, MD CV - January 2014Document221 pagesRobert G. Gish, MD CV - January 2014Robert G. Gish, MDNo ratings yet
- Soap Note-Heidi Martinez PedsDocument6 pagesSoap Note-Heidi Martinez PedsHeidi Martinez100% (2)
- Fatigue: What Is Anemia?Document3 pagesFatigue: What Is Anemia?Annapurna DangetiNo ratings yet
- Tugas Basing 1Document2 pagesTugas Basing 1Alfrits TampemawaNo ratings yet
- ACLS Skills ChecklistDocument2 pagesACLS Skills ChecklistabdullahNo ratings yet
- Possession and Exorcism in The New Testament and Early ChristianityDocument320 pagesPossession and Exorcism in The New Testament and Early ChristianityLarryNo ratings yet
- Valproic AcidDocument4 pagesValproic AcidReneé Camille0% (1)






























































































Download as pdf or txt
You might also like
- Risk Factors & Prognosis For USMLE STEP 3 PDFDocument182 pagesRisk Factors & Prognosis For USMLE STEP 3 PDFSadia GhaniNo ratings yet
- Dyslipidemia MXDocument72 pagesDyslipidemia MXsruthimeena6891No ratings yet
- Chronic Kidney Disease and Its ComplicationsDocument6 pagesChronic Kidney Disease and Its ComplicationsmedicalNo ratings yet
- Primary Prevention of CVDDocument53 pagesPrimary Prevention of CVDYibeltal AssefaNo ratings yet
- Δείκτες φλεγμονήςDocument48 pagesΔείκτες φλεγμονήςeliotkanNo ratings yet
- High Sensitivity CRPDocument10 pagesHigh Sensitivity CRPChrishan ShivanthanNo ratings yet
- Leo Atp IvDocument25 pagesLeo Atp IvLeonardo MedinaNo ratings yet
- Low-Density Lipoprotein Cholesterol and Stroke: How Low Should We Go?Document3 pagesLow-Density Lipoprotein Cholesterol and Stroke: How Low Should We Go?pitiwararom rachtipatNo ratings yet
- Journal Presentation 1Document61 pagesJournal Presentation 1Shalini RachaNo ratings yet
- AtherosclerosisDocument29 pagesAtherosclerosisneeraj banaNo ratings yet
- Coronary Heart Disease Risk Factors Among UniversiDocument6 pagesCoronary Heart Disease Risk Factors Among UniversiMuhammad Irfan JamilNo ratings yet
- Article 164163-PrintDocument22 pagesArticle 164163-PrintIribuka JonathanNo ratings yet
- Dyslipidemia Guidelines Presentation v2Document39 pagesDyslipidemia Guidelines Presentation v2avicennaxNo ratings yet
- Cardiovascular Complication in CKD 28.8.18Document65 pagesCardiovascular Complication in CKD 28.8.18Hemanth PrakashNo ratings yet
- Abstract and IntroductionDocument14 pagesAbstract and Introductiondavid_lg6179No ratings yet
- Case Study 2 MNTDocument11 pagesCase Study 2 MNTapi-242547654No ratings yet
- Raza2004 PDFDocument12 pagesRaza2004 PDFIvana RuseskaNo ratings yet
- Atherosclerosis, Dyslipidaemia and Diabetes SlidesDocument83 pagesAtherosclerosis, Dyslipidaemia and Diabetes SlidesTatiana GobjilăNo ratings yet
- Association of Hypertriglyceridemia With Ischemic Stroke, Study in A Tertiary Care Hospital in BangladeshDocument6 pagesAssociation of Hypertriglyceridemia With Ischemic Stroke, Study in A Tertiary Care Hospital in BangladeshRay HannaNo ratings yet
- 1996 USPSTF High Blood Cholesterol and Other Lipid Abnormalities ScreeningDocument24 pages1996 USPSTF High Blood Cholesterol and Other Lipid Abnormalities ScreeningScott LinNo ratings yet
- Cardiovascular Disorders: Annette HaynesDocument69 pagesCardiovascular Disorders: Annette HaynesBinh Yen Quach TranNo ratings yet
- Original Article Evaluation of Dyslipidaemia in Type 2 Diabetes Mellitus PatientsDocument6 pagesOriginal Article Evaluation of Dyslipidaemia in Type 2 Diabetes Mellitus PatientsEnvhy AmaliaNo ratings yet
- Hiperlipidemia 1-Indah 2017Document16 pagesHiperlipidemia 1-Indah 2017Meg Meg Mega DwiNo ratings yet
- Ischemic Stroke: Prevention Cardioembolism Revascularisation Procedures Stroke in Special CircumstancesDocument24 pagesIschemic Stroke: Prevention Cardioembolism Revascularisation Procedures Stroke in Special Circumstancesnisha24100% (1)
- IncidenceDocument3 pagesIncidenceapi-26340035100% (1)
- 23 Preventive Heart Disease, Dyslipidemia and HTNDocument13 pages23 Preventive Heart Disease, Dyslipidemia and HTNVictor PazNo ratings yet
- Hypertriglyceridemia As A Possible Independent Risk Factor For StrokeDocument6 pagesHypertriglyceridemia As A Possible Independent Risk Factor For StrokeFilbert WashingtonNo ratings yet
- Cardiac Biomarkers: Cardiac Enzymes and BiomarkerDocument21 pagesCardiac Biomarkers: Cardiac Enzymes and Biomarkeranamika sharmaNo ratings yet
- South African Dyslipedemia GuidelineDocument11 pagesSouth African Dyslipedemia Guidelinesmaug_11No ratings yet
- Recommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (AdaptedDocument8 pagesRecommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (Adaptedعزالدين الطيارNo ratings yet
- AtherosclerosisDocument9 pagesAtherosclerosisSharmila SeeralanNo ratings yet
- Coronary Calcium ScoreDocument49 pagesCoronary Calcium ScoreBinod KumarNo ratings yet
- High Sensitivity C-Reactive ProteinDocument100 pagesHigh Sensitivity C-Reactive ProteinFast ComposersNo ratings yet
- Pharmacology & Therapeutics: Anette Varbo, Marianne Benn, Børge G. NordestgaardDocument10 pagesPharmacology & Therapeutics: Anette Varbo, Marianne Benn, Børge G. NordestgaardIonuț CozmaNo ratings yet
- Lipoprotein Paper Academia ZaragedDocument29 pagesLipoprotein Paper Academia Zaragedpawovem755No ratings yet
- Predictive Mortality Risk Factors in Diabetes MellitusDocument6 pagesPredictive Mortality Risk Factors in Diabetes MellitusblueiceNo ratings yet
- Hyper Cholesterol Emi ADocument7 pagesHyper Cholesterol Emi AMohamed EssallaaNo ratings yet
- Diretriz - Dislipidemia EndocrinologiaDocument70 pagesDiretriz - Dislipidemia EndocrinologiaSamara QueirozNo ratings yet
- Dyson LineDocument10 pagesDyson LineSharly DwijayantiNo ratings yet
- Efficacy and Safety of High-Density Lipoprotein Cholesterol-Increasing CompoundsDocument13 pagesEfficacy and Safety of High-Density Lipoprotein Cholesterol-Increasing CompoundsAdityasekar WangiNo ratings yet
- Polygenic HypercholesterolemiaDocument6 pagesPolygenic HypercholesterolemiaSamhitha Ayurvedic ChennaiNo ratings yet
- Coronary Artery DiseaseDocument80 pagesCoronary Artery Diseaseamelia pratiwiNo ratings yet
- C-Reactive Protein (CRP) : Erythrocyte Sedimentation Rate Blood Platelet CountDocument23 pagesC-Reactive Protein (CRP) : Erythrocyte Sedimentation Rate Blood Platelet Countikillyou1900No ratings yet
- Pharmacological Treatment of HyperlipiedmiaDocument8 pagesPharmacological Treatment of HyperlipiedmiajeffaguilarNo ratings yet
- Dyslipidemia Management in Women and Men: Exploring Potential Gender DifferencesDocument7 pagesDyslipidemia Management in Women and Men: Exploring Potential Gender DifferencesAmelie AnsonNo ratings yet
- 2013 ACC/AHA Guideline On The Treatment of Blood Cholesterol To Reduce Atherosclerotic Cardiovascular Risk in AdultsDocument37 pages2013 ACC/AHA Guideline On The Treatment of Blood Cholesterol To Reduce Atherosclerotic Cardiovascular Risk in AdultsIman SaksoukNo ratings yet
- Dyslipidemia Guidelines Feb2010 PDFDocument4 pagesDyslipidemia Guidelines Feb2010 PDFImam Rosyada RijalulhaqNo ratings yet
- Diagnostic Tests and ProceduresDocument49 pagesDiagnostic Tests and Procedurespmahi8854No ratings yet
- Dyslipidemia: Signs and SymptomsDocument24 pagesDyslipidemia: Signs and Symptomschrissanto chandraNo ratings yet
- Association Between Lipid Fractions and Age of First Myocardial InfarctionDocument7 pagesAssociation Between Lipid Fractions and Age of First Myocardial InfarctionAnonymous plYGwXNo ratings yet
- Medical TerminologyDocument17 pagesMedical TerminologySofia Isabelle GarciaNo ratings yet
- Li 2017Document32 pagesLi 2017akshayNo ratings yet
- MR Sayan Project (Hyperkalemia in CKD Patient) PDFDocument27 pagesMR Sayan Project (Hyperkalemia in CKD Patient) PDFManjurul RahamanNo ratings yet
- Inborn Errors of Lipid MetabolismDocument41 pagesInborn Errors of Lipid MetabolismWalterNo ratings yet
- ehab771-2Document3 pagesehab771-2andresadarvegNo ratings yet
- 8 Meq/L PH 7.2) May Require Iv Therapy (See Chap. 51) .: Evaluation of Therapeutic OutcomesDocument2 pages8 Meq/L PH 7.2) May Require Iv Therapy (See Chap. 51) .: Evaluation of Therapeutic OutcomesDebbyNovriozaNo ratings yet
- Optimalmedicaltherapyfor Stableischemicheart Diseasein2024: Focus On Blood Pressure and LipidsDocument13 pagesOptimalmedicaltherapyfor Stableischemicheart Diseasein2024: Focus On Blood Pressure and LipidsCarlos Hernan Castañeda RuizNo ratings yet
- Clinical Surgery Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2From EverandClinical Surgery Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2No ratings yet
- Textbook of Pediatrics, 18th Edition. Philadelphia: Elsevier Inc 2007Document1 pageTextbook of Pediatrics, 18th Edition. Philadelphia: Elsevier Inc 2007dinnhanifahNo ratings yet
- Daftar Pustaka: Biotechnology. 27 (5) : 427-433Document8 pagesDaftar Pustaka: Biotechnology. 27 (5) : 427-433dinnhanifahNo ratings yet
- Textbook of Pediatrics, 18th Edition. Philadelphia: Elsevier Inc 2007Document1 pageTextbook of Pediatrics, 18th Edition. Philadelphia: Elsevier Inc 2007dinnhanifahNo ratings yet
- ACOG Practice Bulletin No 183 Postpartum-Hemorrhage-2017Document19 pagesACOG Practice Bulletin No 183 Postpartum-Hemorrhage-2017dinnhanifahNo ratings yet
- Bipolar in Kaplan & Sadock's Comprehensive Textbook of Psychiatry, 10Document2 pagesBipolar in Kaplan & Sadock's Comprehensive Textbook of Psychiatry, 10dinnhanifahNo ratings yet
- 971S FullDocument3 pages971S FulldinnhanifahNo ratings yet
- Collodion Baby: Presented byDocument10 pagesCollodion Baby: Presented byNoor AhamedNo ratings yet
- Transfusion Reaction PDFDocument1 pageTransfusion Reaction PDFKah Man GohNo ratings yet
- Adapted From Family Planning Competency-Based Training: Basic Course HandbookDocument4 pagesAdapted From Family Planning Competency-Based Training: Basic Course HandbookVanessa EnteroNo ratings yet
- Makalah Bahasa Inggris 2Document7 pagesMakalah Bahasa Inggris 2azizah LasimpalaNo ratings yet
- Pediatric Nursing Dissertation TopicsDocument8 pagesPediatric Nursing Dissertation TopicsCustomCollegePaperCanada100% (1)
- Medical & Homeopathic Research, Homeopathic Medical Collage and ResearchDocument145 pagesMedical & Homeopathic Research, Homeopathic Medical Collage and ResearchMitesh KinariwalaNo ratings yet
- Hemolytic Disease of NewbornDocument41 pagesHemolytic Disease of NewbornRaja100% (3)
- Ground FloorDocument1 pageGround FloorJeya AtharshikaNo ratings yet
- Palliative Care - End of Life Care - Northern HealthDocument8 pagesPalliative Care - End of Life Care - Northern HealthDiklatpimempat AngkatanlimabelasNo ratings yet
- GMP FinalDocument37 pagesGMP FinalekramNo ratings yet
- LP in Science 12 (Basic First Aid)Document9 pagesLP in Science 12 (Basic First Aid)Alvin Cabanela100% (1)
- Seasonal Affective Disorder StudyDocument7 pagesSeasonal Affective Disorder Studyvidro3No ratings yet
- ISlabDocument3 pagesISlabpixiedustNo ratings yet
- SR Diabetic Foot UlcerDocument11 pagesSR Diabetic Foot UlcerDeka AdeNo ratings yet
- Non-Pharmacological Treatment of HypertensionDocument25 pagesNon-Pharmacological Treatment of Hypertensionastrid abrahams0% (2)
- Summary of Benefits: Quartz Medicare Advantage (HMO), in Partnership With UW HealthDocument20 pagesSummary of Benefits: Quartz Medicare Advantage (HMO), in Partnership With UW HealthChris CoulmanNo ratings yet
- Quality and Safety in Compounding Non-Sterile PreparationsDocument5 pagesQuality and Safety in Compounding Non-Sterile PreparationsPruessada DeeyingNo ratings yet
- Nasal Lacrimal Duct ObstructionDocument2 pagesNasal Lacrimal Duct ObstructionAgitha Melita PutriNo ratings yet
- Venous ThromboembolismDocument11 pagesVenous ThromboembolismKrsna Navera100% (1)
- Pertanyaan JurnalDocument2 pagesPertanyaan JurnalodivarNo ratings yet
- Cavernous Sinus Thrombosis of Odontogenic Origin: March 2016Document8 pagesCavernous Sinus Thrombosis of Odontogenic Origin: March 2016Putu WidiastriNo ratings yet
- Contoh Naskah Presentasi KD 26Document3 pagesContoh Naskah Presentasi KD 26Kharisma Nur FajriyahNo ratings yet
- DNB Radio Diagnosis Paper1Document4 pagesDNB Radio Diagnosis Paper1Taha IsmailNo ratings yet
- Robert G. Gish, MD CV - January 2014Document221 pagesRobert G. Gish, MD CV - January 2014Robert G. Gish, MDNo ratings yet
- Soap Note-Heidi Martinez PedsDocument6 pagesSoap Note-Heidi Martinez PedsHeidi Martinez100% (2)
- Fatigue: What Is Anemia?Document3 pagesFatigue: What Is Anemia?Annapurna DangetiNo ratings yet
- Tugas Basing 1Document2 pagesTugas Basing 1Alfrits TampemawaNo ratings yet
- ACLS Skills ChecklistDocument2 pagesACLS Skills ChecklistabdullahNo ratings yet
- Possession and Exorcism in The New Testament and Early ChristianityDocument320 pagesPossession and Exorcism in The New Testament and Early ChristianityLarryNo ratings yet
- Valproic AcidDocument4 pagesValproic AcidReneé Camille0% (1)