Download as pdf or txt
You might also like
- Teach Yourself AbdomenDocument35 pagesTeach Yourself AbdomenSambili Tonny100% (4)
- CBT Dams Paper 1Document129 pagesCBT Dams Paper 1Gajeshwar Bahekar100% (1)
- June 2014 Questions Returned From Candidates - Thank You: Long Case 1Document14 pagesJune 2014 Questions Returned From Candidates - Thank You: Long Case 1karan270100% (1)
- Lumbosacral PlexusDocument3 pagesLumbosacral Plexusgehaoi4No ratings yet
- Acta Obstet Gynecol Scand - 2015 - Niklasson - Risk factors for persistent pain and its influence on maternal wellbeingDocument7 pagesActa Obstet Gynecol Scand - 2015 - Niklasson - Risk factors for persistent pain and its influence on maternal wellbeingRafael PivovarNo ratings yet
- Minoufia Med J 2020 33 2 427 432 EngDocument6 pagesMinoufia Med J 2020 33 2 427 432 Engaditya prakashNo ratings yet
- Single-Knot Versus Multiple-Knot Technique of Perineal Repair - A Randomised Controlled TrialDocument8 pagesSingle-Knot Versus Multiple-Knot Technique of Perineal Repair - A Randomised Controlled TrialDR RISKA WAHYUNo ratings yet
- Recurrence of Ovarian Endometrioma After Laparoscopic ExcisionDocument4 pagesRecurrence of Ovarian Endometrioma After Laparoscopic ExcisionPutri Tamara DasantosNo ratings yet
- Essential Elements For Enhanced Recovery After Intra-Abdominal SurgeryDocument4 pagesEssential Elements For Enhanced Recovery After Intra-Abdominal SurgeryJonathan MartinNo ratings yet
- Benson Relaxation Technique in Reducing Pain Intensity in Women After Cesarean SectionDocument5 pagesBenson Relaxation Technique in Reducing Pain Intensity in Women After Cesarean SectionMarinaNo ratings yet
- 1 s2.0 S1743919122006148 MainDocument9 pages1 s2.0 S1743919122006148 Mainiwm28458No ratings yet
- Blunt Trauma To Abdomen in Rural Setup: A Multiple Case StudyDocument4 pagesBlunt Trauma To Abdomen in Rural Setup: A Multiple Case StudyElis FatmayantiNo ratings yet
- 2021 Article 1523Document9 pages2021 Article 1523Pratama RiyadNo ratings yet
- Chapter No# 1: Definition of Cesarean SectionDocument27 pagesChapter No# 1: Definition of Cesarean SectionRabiaNo ratings yet
- JurnalDocument14 pagesJurnalYudha WahyuNo ratings yet
- Jurnal 10Document11 pagesJurnal 10DM internaNo ratings yet
- Is Modern Perioperative Care Too Complicated For Surgeons?: ReferencesDocument2 pagesIs Modern Perioperative Care Too Complicated For Surgeons?: ReferencesHasriana BudimanNo ratings yet
- Peahl 2020Document1 pagePeahl 2020FebbyNo ratings yet
- Intraoperative Injuries of The Urinary TractDocument14 pagesIntraoperative Injuries of The Urinary TractDEVINANo ratings yet
- Case Study in Surgical First Assistant For NursesDocument13 pagesCase Study in Surgical First Assistant For NursesQuality ResearchNo ratings yet
- Effect of Anxiolytic Dose On Incidence of Intraoperative Nausea and Vomiting in CS Under Spinal AnesthesiaDocument8 pagesEffect of Anxiolytic Dose On Incidence of Intraoperative Nausea and Vomiting in CS Under Spinal AnesthesiaCentral Asian StudiesNo ratings yet
- Jurnal 2019Document6 pagesJurnal 2019Niniek Iin FNo ratings yet
- Is The Combination of An Abdominoplasty With A Cesarean Section Safe A New Concept of Beauty LaborDocument2 pagesIs The Combination of An Abdominoplasty With A Cesarean Section Safe A New Concept of Beauty LaborChristina VasquezNo ratings yet
- Journal of Pediatric Surgery Case ReportsDocument5 pagesJournal of Pediatric Surgery Case ReportsFadhilNo ratings yet
- Aap 0000000000000641Document23 pagesAap 0000000000000641BeagabcnNo ratings yet
- Comparison of Transverse and Vertical Skin Incision ForDocument13 pagesComparison of Transverse and Vertical Skin Incision ForHerry SasukeNo ratings yet
- Macgregor 2020Document6 pagesMacgregor 2020FebbyNo ratings yet
- ARTICLEDocument8 pagesARTICLEazza atyaNo ratings yet
- Intra OpDocument12 pagesIntra OpalodiarkNo ratings yet
- To Evaluate The Efficacy of Ultrasonography Guided Pectoral Nerve Block For Postoperative Analgesia in Breast SurgeriesDocument4 pagesTo Evaluate The Efficacy of Ultrasonography Guided Pectoral Nerve Block For Postoperative Analgesia in Breast SurgeriesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 1 s2.0 S2214139116300026 Main PDFDocument8 pages1 s2.0 S2214139116300026 Main PDFAnonymous T4IxYOoBBGNo ratings yet
- 1 s2.0 S1015958422008909 MainDocument4 pages1 s2.0 S1015958422008909 MainYohan WijayabahuNo ratings yet
- Assessing Pain Relief Following Medical and Surgical Interventions For Lumbar Disc HerniationDocument4 pagesAssessing Pain Relief Following Medical and Surgical Interventions For Lumbar Disc HerniationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Bogie PDFDocument4 pagesBogie PDFIfanz AmrullahNo ratings yet
- 10.1007@s00192 020 04317 1Document9 pages10.1007@s00192 020 04317 1abdi syahputraNo ratings yet
- IndianJAnaesth6311924-2183535 060355Document8 pagesIndianJAnaesth6311924-2183535 060355Abhijeet ThakurNo ratings yet
- Clinical Study: The Comparison of Lichtenstein Procedure With and Without Mesh-Fixation For Inguinal Hernia RepairDocument5 pagesClinical Study: The Comparison of Lichtenstein Procedure With and Without Mesh-Fixation For Inguinal Hernia RepairFikri AlfarisyiNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument7 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologyOrlando Pereira CativoNo ratings yet
- Oamjms 10b 1148Document5 pagesOamjms 10b 1148hanifNo ratings yet
- Fonc 09 00597Document13 pagesFonc 09 00597Giann PersonaNo ratings yet
- Wino Cour 2014Document8 pagesWino Cour 2014Ricardo AcostaNo ratings yet
- Cesarean Delivery Procedures Recovery AnDocument13 pagesCesarean Delivery Procedures Recovery AnFitriNo ratings yet
- 6037ASTR Astr 97 103Document9 pages6037ASTR Astr 97 103LuisNavarroHernandezNo ratings yet
- KJP 34 4 487Document14 pagesKJP 34 4 487Abante_gammaNo ratings yet
- Scott 2015Document20 pagesScott 2015Raíla SoaresNo ratings yet
- Enteral FeedingDocument5 pagesEnteral Feedingricardo arreguiNo ratings yet
- 1 s2.0 S101595842100292X MainDocument7 pages1 s2.0 S101595842100292X MainNUR HAMIDAHNo ratings yet
- A Comparative Study Between Erector Spinae Plane Block With General Anesthesia Versus Conventional Intravenous Analgesics With General Anesthesia inDocument8 pagesA Comparative Study Between Erector Spinae Plane Block With General Anesthesia Versus Conventional Intravenous Analgesics With General Anesthesia inrafiaNo ratings yet
- JCM 10 00913Document11 pagesJCM 10 00913Delivery ServiceNo ratings yet
- Abdominal BinderDocument6 pagesAbdominal BinderyinvilllNo ratings yet
- 4163-Article Text-41530-4-10-20220105Document5 pages4163-Article Text-41530-4-10-20220105Redia FalaNo ratings yet
- 812-Article Text-2928-1-10-20191129 (PMR)Document6 pages812-Article Text-2928-1-10-20191129 (PMR)Azza SintaNo ratings yet
- JCM 10 01853Document16 pagesJCM 10 01853Katrina Mae FajardoNo ratings yet
- Journal Pre-Proof: Journal of The American College of SurgeonsDocument28 pagesJournal Pre-Proof: Journal of The American College of SurgeonsIvory June CadeteNo ratings yet
- Sonnykalangi,+151 +Fiska+M+Muhammad+863-68Document6 pagesSonnykalangi,+151 +Fiska+M+Muhammad+863-68Evieta CallysthaNo ratings yet
- The Effects of Continuous and Interrupted Episiotomy Repair On Pain Severity and Rate of Perineal Repair: A Controlled Randomized Clinical TrialDocument13 pagesThe Effects of Continuous and Interrupted Episiotomy Repair On Pain Severity and Rate of Perineal Repair: A Controlled Randomized Clinical TrialMarfuahRobertoNo ratings yet
- The Effect of Obesity On Surgical Treatment of Achilles Tendon RupturesDocument7 pagesThe Effect of Obesity On Surgical Treatment of Achilles Tendon RupturesMusdalipa Hi.palanroNo ratings yet
- Apendisitis AkutDocument17 pagesApendisitis AkutYola BondonkNo ratings yet
- The Role of Homoeopathic Treatment in Women Suffering From Post-CDocument10 pagesThe Role of Homoeopathic Treatment in Women Suffering From Post-CUtpal KumarNo ratings yet
- Comparison Infant Pain ScaleDocument5 pagesComparison Infant Pain ScaleDian KusumastutiNo ratings yet
- Laparoscopic Cholecystectomy Under Spinal AnaestheDocument7 pagesLaparoscopic Cholecystectomy Under Spinal Anaestherazaqhussain00No ratings yet
- 10.1007@s00192 019 03894 0Document16 pages10.1007@s00192 019 03894 0abdi syahputraNo ratings yet
- Post-cholecystectomy Bile Duct InjuryFrom EverandPost-cholecystectomy Bile Duct InjuryVinay K. KapoorNo ratings yet
- Case Studies of Postoperative Complications after Digestive SurgeryFrom EverandCase Studies of Postoperative Complications after Digestive SurgeryNo ratings yet
- Placental Anatomy and Physiology: Ppds Basic 2019Document31 pagesPlacental Anatomy and Physiology: Ppds Basic 2019Andre Putra100% (1)
- NHS PreeclampsiaDocument17 pagesNHS PreeclampsiaAndre PutraNo ratings yet
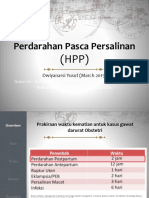
- Perdarahan Pasca Persalinan: Dwiyanarsi Yusuf (March 2015)Document26 pagesPerdarahan Pasca Persalinan: Dwiyanarsi Yusuf (March 2015)Rizur SufisonNo ratings yet
- Ajog AcsDocument3 pagesAjog AcsAndre PutraNo ratings yet
- Absent End DiastolicDocument12 pagesAbsent End DiastolicAndre PutraNo ratings yet
- Prenatal Care AndreDocument29 pagesPrenatal Care AndreAndre PutraNo ratings yet
- Prenatal Care AndreDocument29 pagesPrenatal Care AndreAndre PutraNo ratings yet
- Multiple PregnancyDocument71 pagesMultiple PregnancyAndre PutraNo ratings yet
- Ovarian Cancer SGTDocument25 pagesOvarian Cancer SGTAndre PutraNo ratings yet
- Dutch School MeetingDocument2 pagesDutch School MeetingAndre PutraNo ratings yet
- AnatomyDocument49 pagesAnatomyDrGandhi Bhaskar Patrudu Lanka50% (2)
- Fascia Iliaca GuidelineDocument12 pagesFascia Iliaca GuidelineSyahrul Mubarak Danar SumantriNo ratings yet
- Mnemonics For Block 3Document3 pagesMnemonics For Block 3sahana2791No ratings yet
- Hassan Nawaz - 202321192010Document15 pagesHassan Nawaz - 202321192010hassanNo ratings yet
- Lower Limb: Front and Medial Aspect of ThighDocument8 pagesLower Limb: Front and Medial Aspect of ThighErnie G. Bautista II, RN, MDNo ratings yet
- Lower Limb AnatomyDocument43 pagesLower Limb AnatomyJason Toniolo100% (2)
- Lower Limb BlocksDocument5 pagesLower Limb BlocksParvathy R NairNo ratings yet
- STUDY GUIDE-LOCOMOTOR-2019 1st YearDocument30 pagesSTUDY GUIDE-LOCOMOTOR-2019 1st YearhamdyyalyNo ratings yet
- Lumbosacral PlexusDocument41 pagesLumbosacral PlexusJanelle MadayagNo ratings yet
- Spinal Cord and Spinal NervesDocument9 pagesSpinal Cord and Spinal NervesJharaNo ratings yet
- Peripheral Nerve InjuriesDocument207 pagesPeripheral Nerve InjuriesAashka MahetaNo ratings yet
- Abdominal Wall: Um-Hani'S Qbank Um-Hani'S QbankDocument5 pagesAbdominal Wall: Um-Hani'S Qbank Um-Hani'S QbankmedisharedNo ratings yet
- Nerve and Blood Supply of Lower ExtremitiesDocument22 pagesNerve and Blood Supply of Lower ExtremitiesBenjamin Prabhu100% (3)
- 21 - 22 GIT - UGS - ENDO - EXT MCQs-1Document23 pages21 - 22 GIT - UGS - ENDO - EXT MCQs-1dajisafe829No ratings yet
- (TRANS) Posterior Abdominal Wall Part 2Document7 pages(TRANS) Posterior Abdominal Wall Part 2Paulina DocenaNo ratings yet
- Atlas of Nerve Conduction Studies and Electromyography (2 Ed.)Document10 pagesAtlas of Nerve Conduction Studies and Electromyography (2 Ed.)rodrigocorcino899959No ratings yet
- Axonotmesis, and Neurotmesis) and by SunderlandDocument24 pagesAxonotmesis, and Neurotmesis) and by SunderlandSakanadeNo ratings yet
- The Peripheral Nervous System (PNS)Document47 pagesThe Peripheral Nervous System (PNS)Kathleen Joy Partoza PlagataNo ratings yet
- Urinary System - Gross 2016Document73 pagesUrinary System - Gross 2016dawnparkNo ratings yet
- 210420PM PPT - Femoral NerveDocument23 pages210420PM PPT - Femoral NerveAananda Raaj V MNo ratings yet
- Lab - Manual - Spinal - Cord - and - Spinal - Nerves - Atlas - 7-9-19 2 PDFDocument30 pagesLab - Manual - Spinal - Cord - and - Spinal - Nerves - Atlas - 7-9-19 2 PDFAjaykumar C DwivediNo ratings yet
- Division of Spinal CordDocument23 pagesDivision of Spinal CordBibek SutradharNo ratings yet
- Injuries To The Lumbosacral PlexusDocument8 pagesInjuries To The Lumbosacral PlexusKhriz Ann C ÜNo ratings yet
- Essentials of Regional Anesthesia Anatomy NYSORA - The New York School of Regional AnesthesiaDocument31 pagesEssentials of Regional Anesthesia Anatomy NYSORA - The New York School of Regional Anesthesiajorge ceballos troncosoNo ratings yet
- Dr. Abdul Rashad Senior Lecturer DPT, Mphill (Opt), Mppta, MMTC (NZ), MSTC (Aus), Iastm (Greece) United College of Physical TherapyDocument41 pagesDr. Abdul Rashad Senior Lecturer DPT, Mphill (Opt), Mppta, MMTC (NZ), MSTC (Aus), Iastm (Greece) United College of Physical TherapypashaNo ratings yet
- Lecture 11 Posterior Abdominal WallDocument33 pagesLecture 11 Posterior Abdominal WallIrumNo ratings yet