
Nonsurgical Management of A Periapical Cyst
Nonsurgical Management of A Periapical Cyst
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- MKSAP 19 Endocrinology and Metabolism (ACP)Document168 pagesMKSAP 19 Endocrinology and Metabolism (ACP)Emin bojec100% (3)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Med Bed Info From Skye PrinceDocument9 pagesMed Bed Info From Skye PrinceTim0% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Bacterial Infections Vs Viral ChartDocument1 pageBacterial Infections Vs Viral ChartRobert Moses LimNo ratings yet
- Magnesium ReplacementDocument4 pagesMagnesium ReplacementArvenaa SubramaniamNo ratings yet
- SynopsisDocument9 pagesSynopsisjoy parimalaNo ratings yet
- This Study Resource Was: Pediatric Case 2: Sabina VasquezDocument4 pagesThis Study Resource Was: Pediatric Case 2: Sabina VasquezKyuSheenNo ratings yet
- Therapy Format I. Therapy: News Sharing Therapy Date: July 28, 2021 II. Materials/EquipmentDocument2 pagesTherapy Format I. Therapy: News Sharing Therapy Date: July 28, 2021 II. Materials/EquipmentAesthea BondadNo ratings yet
- Purperal InfectionsDocument69 pagesPurperal InfectionsBeulah DasariNo ratings yet
- Venipuncture WorksheetDocument5 pagesVenipuncture WorksheetAmy YmaNo ratings yet
- EO 7 S 2021 Creation-Of-CODE-Team - BarangayDocument2 pagesEO 7 S 2021 Creation-Of-CODE-Team - BarangayBARANGAY MOLINO IINo ratings yet
- Hyperkalemia Treatment - EmedicineDocument16 pagesHyperkalemia Treatment - EmedicineRian Segal HidajatNo ratings yet
- Massive HemorrhageDocument17 pagesMassive HemorrhageShannen Madrid Tindugan100% (1)
- CRRT When and How Diploma 2024Document21 pagesCRRT When and How Diploma 2024wesam.uv55No ratings yet
- Antipsychotic DrugsDocument44 pagesAntipsychotic DrugsPaulus Widjanarko Brotosaputro0% (1)
- Ex LapDocument42 pagesEx LapOmar Khalif Amad PendatunNo ratings yet
- Tetanus in Cattle: Review and Case Description of Clinical Tetanus in A Holstein HeiferDocument8 pagesTetanus in Cattle: Review and Case Description of Clinical Tetanus in A Holstein HeiferSgk ManikandanNo ratings yet
- What Is Cognitive Impairmenwhat Is Cognitive Impairment?Document5 pagesWhat Is Cognitive Impairmenwhat Is Cognitive Impairment?clccornerNo ratings yet
- Kardex SystemDocument43 pagesKardex SystemBlanche MillizcentNo ratings yet
- Individual Dental Health Record: Republic of The PhilippinesDocument2 pagesIndividual Dental Health Record: Republic of The PhilippinesAto SupNo ratings yet
- Curs RJ Endoc EnglishDocument62 pagesCurs RJ Endoc EnglishArleen MatincaNo ratings yet
- Breasted. The Edwin Smith Surgical Papirus - V1Document634 pagesBreasted. The Edwin Smith Surgical Papirus - V1Juan Manuel Mendoza RodríguezNo ratings yet
- Pediatric Vaccine Àd Vaccination PDFDocument257 pagesPediatric Vaccine Àd Vaccination PDFntnquynhpro100% (2)
- LESSON PLAN Shwe Final PmsDocument14 pagesLESSON PLAN Shwe Final PmsSanthu Su100% (1)
- Perinatal Factor Journal PediatricDocument8 pagesPerinatal Factor Journal PediatricHasya KinasihNo ratings yet
- IX. Discharge PlanDocument2 pagesIX. Discharge PlanAlfrien Ivanovich LarchsonNo ratings yet
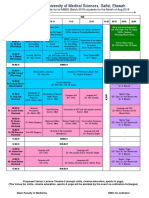
- Lunch: Foundation Course Time Table For Ist MBBS (Batch 2019) Students For The Month of Aug.2019Document2 pagesLunch: Foundation Course Time Table For Ist MBBS (Batch 2019) Students For The Month of Aug.2019Vishal SinghNo ratings yet
- Adalizumab PDFDocument12 pagesAdalizumab PDFAyu Angger PuteriNo ratings yet
- Additional EnglishDocument23 pagesAdditional Englishadv suryakant jadhav0% (1)
- Nursing Care Plan For "AIDS"Document31 pagesNursing Care Plan For "AIDS"jhonroks88% (8)
- Report On 470 Bedded General HospitalDocument16 pagesReport On 470 Bedded General HospitalkuldeepNo ratings yet





































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- MKSAP 19 Endocrinology and Metabolism (ACP)Document168 pagesMKSAP 19 Endocrinology and Metabolism (ACP)Emin bojec100% (3)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Med Bed Info From Skye PrinceDocument9 pagesMed Bed Info From Skye PrinceTim0% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Bacterial Infections Vs Viral ChartDocument1 pageBacterial Infections Vs Viral ChartRobert Moses LimNo ratings yet
- Magnesium ReplacementDocument4 pagesMagnesium ReplacementArvenaa SubramaniamNo ratings yet
- SynopsisDocument9 pagesSynopsisjoy parimalaNo ratings yet
- This Study Resource Was: Pediatric Case 2: Sabina VasquezDocument4 pagesThis Study Resource Was: Pediatric Case 2: Sabina VasquezKyuSheenNo ratings yet
- Therapy Format I. Therapy: News Sharing Therapy Date: July 28, 2021 II. Materials/EquipmentDocument2 pagesTherapy Format I. Therapy: News Sharing Therapy Date: July 28, 2021 II. Materials/EquipmentAesthea BondadNo ratings yet
- Purperal InfectionsDocument69 pagesPurperal InfectionsBeulah DasariNo ratings yet
- Venipuncture WorksheetDocument5 pagesVenipuncture WorksheetAmy YmaNo ratings yet
- EO 7 S 2021 Creation-Of-CODE-Team - BarangayDocument2 pagesEO 7 S 2021 Creation-Of-CODE-Team - BarangayBARANGAY MOLINO IINo ratings yet
- Hyperkalemia Treatment - EmedicineDocument16 pagesHyperkalemia Treatment - EmedicineRian Segal HidajatNo ratings yet
- Massive HemorrhageDocument17 pagesMassive HemorrhageShannen Madrid Tindugan100% (1)
- CRRT When and How Diploma 2024Document21 pagesCRRT When and How Diploma 2024wesam.uv55No ratings yet
- Antipsychotic DrugsDocument44 pagesAntipsychotic DrugsPaulus Widjanarko Brotosaputro0% (1)
- Ex LapDocument42 pagesEx LapOmar Khalif Amad PendatunNo ratings yet
- Tetanus in Cattle: Review and Case Description of Clinical Tetanus in A Holstein HeiferDocument8 pagesTetanus in Cattle: Review and Case Description of Clinical Tetanus in A Holstein HeiferSgk ManikandanNo ratings yet
- What Is Cognitive Impairmenwhat Is Cognitive Impairment?Document5 pagesWhat Is Cognitive Impairmenwhat Is Cognitive Impairment?clccornerNo ratings yet
- Kardex SystemDocument43 pagesKardex SystemBlanche MillizcentNo ratings yet
- Individual Dental Health Record: Republic of The PhilippinesDocument2 pagesIndividual Dental Health Record: Republic of The PhilippinesAto SupNo ratings yet
- Curs RJ Endoc EnglishDocument62 pagesCurs RJ Endoc EnglishArleen MatincaNo ratings yet
- Breasted. The Edwin Smith Surgical Papirus - V1Document634 pagesBreasted. The Edwin Smith Surgical Papirus - V1Juan Manuel Mendoza RodríguezNo ratings yet
- Pediatric Vaccine Àd Vaccination PDFDocument257 pagesPediatric Vaccine Àd Vaccination PDFntnquynhpro100% (2)
- LESSON PLAN Shwe Final PmsDocument14 pagesLESSON PLAN Shwe Final PmsSanthu Su100% (1)
- Perinatal Factor Journal PediatricDocument8 pagesPerinatal Factor Journal PediatricHasya KinasihNo ratings yet
- IX. Discharge PlanDocument2 pagesIX. Discharge PlanAlfrien Ivanovich LarchsonNo ratings yet
- Lunch: Foundation Course Time Table For Ist MBBS (Batch 2019) Students For The Month of Aug.2019Document2 pagesLunch: Foundation Course Time Table For Ist MBBS (Batch 2019) Students For The Month of Aug.2019Vishal SinghNo ratings yet
- Adalizumab PDFDocument12 pagesAdalizumab PDFAyu Angger PuteriNo ratings yet
- Additional EnglishDocument23 pagesAdditional Englishadv suryakant jadhav0% (1)
- Nursing Care Plan For "AIDS"Document31 pagesNursing Care Plan For "AIDS"jhonroks88% (8)
- Report On 470 Bedded General HospitalDocument16 pagesReport On 470 Bedded General HospitalkuldeepNo ratings yet