
Fee Schedule Blue (D) PDF
Fee Schedule Blue (D) PDF
You might also like
- Ada CodesDocument9 pagesAda CodesEdna Jaquez0% (1)
- Meril Suture Catalogue Final Pages Deleted (1 24.40 44.50 64)Document44 pagesMeril Suture Catalogue Final Pages Deleted (1 24.40 44.50 64)threwaway75% (4)
- Dental Charting (Updated)Document56 pagesDental Charting (Updated)Rose Antoinette Umayam100% (1)
- CPT CodesDocument9 pagesCPT CodesSheree AnnNo ratings yet
- CDT 2017 - Code On Dental Proc - Nomenclature OnlineDocument20 pagesCDT 2017 - Code On Dental Proc - Nomenclature OnlineErwin FelipeNo ratings yet
- Ada CodesDocument4 pagesAda CodestedyNo ratings yet
- Drilling Fluids ManualDocument486 pagesDrilling Fluids ManualParaZzzit100% (12)
- Fee Schedule Yellow (A) UpdatedDocument2 pagesFee Schedule Yellow (A) Updatedade melly septianaNo ratings yet
- Fee Schedull Provider (Ace Dental)Document1 pageFee Schedull Provider (Ace Dental)primazamsaNo ratings yet
- 2013 CA Dental OverviewDocument6 pages2013 CA Dental OverviewsvlimNo ratings yet
- Cigna Dental Care Patient Charge Schedule: (Dhmo)Document16 pagesCigna Dental Care Patient Charge Schedule: (Dhmo)Susanta BeheraNo ratings yet
- Patient Encounter Form: Facility Number: Facility Name: Facility Address: NPI NumberDocument2 pagesPatient Encounter Form: Facility Number: Facility Name: Facility Address: NPI NumberJayNo ratings yet
- Orthodontic CDTDocument2 pagesOrthodontic CDTnaharmampillyNo ratings yet
- Translation of Current Dental Terminology American Dental Association (Updated July 2020)Document22 pagesTranslation of Current Dental Terminology American Dental Association (Updated July 2020)Nouran Ayman Mahmoud Kamal Mahmoud Ghonime Nouran Ayman Mahmoud Kamal Mahmoud GhonimeNo ratings yet
- CDT CodesDocument32 pagesCDT CodesTariq KhalidNo ratings yet
- Dental RVU Cookbook: Washington State Health Care AuthorityDocument9 pagesDental RVU Cookbook: Washington State Health Care AuthorityPaul GNo ratings yet
- Aetna Dental Low DmoDocument9 pagesAetna Dental Low DmoBeau PeskaNo ratings yet
- PMW 0031 2.19 PDFDocument13 pagesPMW 0031 2.19 PDFFelton Small Jr.No ratings yet
- MSBY Medical Package ListDocument32 pagesMSBY Medical Package ListSakshi G AwasthiNo ratings yet
- Screenshot 2023-01-25 at 15.07.02Document1 pageScreenshot 2023-01-25 at 15.07.02PikynelPykinescuNo ratings yet
- ADA Ortho CodesDocument1 pageADA Ortho CodesAmerican Aesthetic MCNo ratings yet
- UPCD Dental Services Clinical FeesDocument2 pagesUPCD Dental Services Clinical FeescreamyfrappeNo ratings yet
- 2023 ADA Code List For Microsoft PlansDocument54 pages2023 ADA Code List For Microsoft PlansAngelica PillaNo ratings yet
- Dent CPD KalbarDocument46 pagesDent CPD KalbarHardiansyah HardiNo ratings yet
- Important RQS:: Ait Is Asda Question and Answer Confirmed From Mastry AppDocument64 pagesImportant RQS:: Ait Is Asda Question and Answer Confirmed From Mastry AppParamjit KaurNo ratings yet
- PG Dental Fee and Seat 2020Document1 pagePG Dental Fee and Seat 2020Saurav SumanNo ratings yet
- Medicare Excel FileDocument22 pagesMedicare Excel FileshobhaNo ratings yet
- Company: Plan: XD04 Annual Fee:: CE Limited (博苗有限公司)Document2 pagesCompany: Plan: XD04 Annual Fee:: CE Limited (博苗有限公司)碌葛一No ratings yet
- 價目表 Price ListDocument3 pages價目表 Price ListPatrick WongNo ratings yet
- Life Line Dental Pricelist (Revised)Document6 pagesLife Line Dental Pricelist (Revised)drsobanNo ratings yet
- Dental PricingDocument4 pagesDental PricingsolutionbeautyNo ratings yet
- Translation of Current Dental Terminology American Dental Association (Updated July 2020)Document2 pagesTranslation of Current Dental Terminology American Dental Association (Updated July 2020)ABNo ratings yet
- 2022-Pricelist Feb2022 PDFDocument2 pages2022-Pricelist Feb2022 PDFjackNo ratings yet
- Cubierta Dental D-611 P.ideal C.P. 2Document4 pagesCubierta Dental D-611 P.ideal C.P. 2JessicaNo ratings yet
- Inbound 6373724171176570885Document19 pagesInbound 6373724171176570885Diácono Rui Cunha CamposNo ratings yet
- 2023 Dental Benefit Criteria GuidanceDocument18 pages2023 Dental Benefit Criteria GuidancebrennanandbrennanlawNo ratings yet
- Dental PlanDocument5 pagesDental PlanBhavna ChakrabortyNo ratings yet
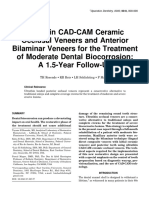
- Ultrathin CAD-CAM Ceramic Occlusal Veneers and Anterior Bilaminar Veneers For The Treatment of Moderate Dental Biocorrosion: A 1.5-Year Follow-UpDocument10 pagesUltrathin CAD-CAM Ceramic Occlusal Veneers and Anterior Bilaminar Veneers For The Treatment of Moderate Dental Biocorrosion: A 1.5-Year Follow-Upharshal shetyeNo ratings yet
- TPA & INSURANCE Rates - HDFC eRGODocument2 pagesTPA & INSURANCE Rates - HDFC eRGORahul WaskelNo ratings yet
- Daftar Barang Yang Masuk Di Ekatalog 2019: No. Jenis Produk Nama Produk Merek Dan Type Produk HargaDocument7 pagesDaftar Barang Yang Masuk Di Ekatalog 2019: No. Jenis Produk Nama Produk Merek Dan Type Produk HargaRakhmayanto AbizulfaNo ratings yet
- LSG DentalDocument1 pageLSG Dentalres6250No ratings yet
- DtFLHumana FL HI215 11.2012Document6 pagesDtFLHumana FL HI215 11.2012jeff-swansonNo ratings yet
- CDocument4 pagesCdentcare.insuNo ratings yet
- Setoran Umum Gigi Mei 2022Document4 pagesSetoran Umum Gigi Mei 2022Agatha PutriNo ratings yet
- Bhamashah Swasthya Bima Yojana 2017-19: S. No. Final Package Name Package Type Proposed Rate Speciality Code Short NameDocument21 pagesBhamashah Swasthya Bima Yojana 2017-19: S. No. Final Package Name Package Type Proposed Rate Speciality Code Short Nameswastik hospitalNo ratings yet
- Mapping MGDocument4 pagesMapping MGdentcare.insuNo ratings yet
- Cobertura ODO562Document6 pagesCobertura ODO562Juan Manuel FerreroNo ratings yet
- COTATION AFCOTT CAM SARL - Fr.enDocument1 pageCOTATION AFCOTT CAM SARL - Fr.enMichel erickson talom waboNo ratings yet
- Price List CAB Dental 2016Document12 pagesPrice List CAB Dental 2016Fachrul Latif DentistNo ratings yet
- 2023 Pricelist Grey Gables Dental PracticeDocument2 pages2023 Pricelist Grey Gables Dental Practicevioleta.dan91No ratings yet
- Pc-1000 Panoramic X-Ray Service ManualDocument4 pagesPc-1000 Panoramic X-Ray Service ManualJosé Luís Cheo Barrios CristóbalNo ratings yet
- 2022 Republic Services REPU - 20221014Document2 pages2022 Republic Services REPU - 20221014kenneth.chronister9458No ratings yet
- ExodontiasDocument19 pagesExodontiasmameekasim75No ratings yet
- Unitedhealthcare Dental Ppo Plan 2022 Summary of Benefits and CoverageDocument1 pageUnitedhealthcare Dental Ppo Plan 2022 Summary of Benefits and CoverageAdam CliftonNo ratings yet
- Traducere in Engleza Site Spring Dental Mihaela VelcuDocument11 pagesTraducere in Engleza Site Spring Dental Mihaela VelcuFlorin Cornel VelcuNo ratings yet
- ArticleDocument8 pagesArticleMairaMaraviChavezNo ratings yet
- Harga Bahan DentalDocument19 pagesHarga Bahan Dentalarief hendra wijayaNo ratings yet
- Esthetic Oral Rehabilitation with Veneers: A Guide to Treatment Preparation and Clinical ConceptsFrom EverandEsthetic Oral Rehabilitation with Veneers: A Guide to Treatment Preparation and Clinical ConceptsRichard D. TrushkowskyNo ratings yet
- DENTURES: The Ultimate Guide to Dentures & Denture Care for a Beautifully Restored SmileFrom EverandDENTURES: The Ultimate Guide to Dentures & Denture Care for a Beautifully Restored SmileNo ratings yet
- Cone Beam Computed Tomography: Oral and Maxillofacial Diagnosis and ApplicationsFrom EverandCone Beam Computed Tomography: Oral and Maxillofacial Diagnosis and ApplicationsDavid SarmentNo ratings yet
- Digits and Widgets: (With Reference To A Wise Mother, The Golden BookDocument7 pagesDigits and Widgets: (With Reference To A Wise Mother, The Golden Bookloristahl8340No ratings yet
- Maintenance Manual SinotruckDocument21 pagesMaintenance Manual SinotruckCôn LuânNo ratings yet
- A Recommender System Based On PersonalDocument15 pagesA Recommender System Based On Personalreiko-sanNo ratings yet
- EscortsDocument59 pagesEscortsVijay Malik100% (2)
- Double Wedding Ring Size Fabric Requirements EditedDocument3 pagesDouble Wedding Ring Size Fabric Requirements EditedfrapatchNo ratings yet
- District CalendarDocument1 pageDistrict Calendarapi-271737972No ratings yet
- PPG TestDocument2 pagesPPG TestAljon MendozaNo ratings yet
- Bryce Boerste - Personal College Essay - Draft 2Document3 pagesBryce Boerste - Personal College Essay - Draft 2api-492128881No ratings yet
- Logging InnovationDocument8 pagesLogging InnovationAnkit ChourasiaNo ratings yet
- Prelims-Arche 4 Sy 2122-StudentsDocument3 pagesPrelims-Arche 4 Sy 2122-StudentsAaron CansinoNo ratings yet
- Democratization of Secondary School in MalaysiaDocument12 pagesDemocratization of Secondary School in MalaysiaKavinesh Kaneson100% (1)
- Deteqstandart PDFDocument4 pagesDeteqstandart PDFMoaed KanbarNo ratings yet
- Proverbs 18-24 Ronnie LoudermilkDocument1 pageProverbs 18-24 Ronnie LoudermilkKeneth Chris NamocNo ratings yet
- 8 Fall of The Ottoman EmpireDocument10 pages8 Fall of The Ottoman Empireapi-303147801No ratings yet
- Load Cell Input ModuleDocument3 pagesLoad Cell Input Moduleabo omrNo ratings yet
- Classroom Accommodations For Students With Learning Difficulties and DisabilitiesDocument2 pagesClassroom Accommodations For Students With Learning Difficulties and Disabilitiesapi-359063455No ratings yet
- Indian Heart JournalDocument18 pagesIndian Heart JournalSanaSofiyahNo ratings yet
- Tushar Kumar B P Operating Systems Digital Assignment-2Document5 pagesTushar Kumar B P Operating Systems Digital Assignment-2Chirosuke TashiNo ratings yet
- SCADA System PDFDocument420 pagesSCADA System PDFbambang_gastomoNo ratings yet
- Freezing Baked GoodsDocument9 pagesFreezing Baked GoodsBenjamin DoverNo ratings yet
- Missalette FINAL PDFDocument32 pagesMissalette FINAL PDFJohnpaul MenchavezNo ratings yet
- Thời gian làm bài 120 phút, không kể thời gian giao đềDocument9 pagesThời gian làm bài 120 phút, không kể thời gian giao đềĐỗ Hoàng DũngNo ratings yet
- Solucion Listening Unit 5Document2 pagesSolucion Listening Unit 5ManoloNo ratings yet
- Study Guide For Tanizaki Jun'ichirō "The Secret" (Himitsu, 1911, Tr. A. Chambers)Document3 pagesStudy Guide For Tanizaki Jun'ichirō "The Secret" (Himitsu, 1911, Tr. A. Chambers)BeholdmyswarthyfaceNo ratings yet
- To Biochemistry: Murang'a University of TechnologyDocument6 pagesTo Biochemistry: Murang'a University of TechnologyJoseph NyabugaNo ratings yet
- Marketing Advanced HW 3 A5-7, A9-12Document3 pagesMarketing Advanced HW 3 A5-7, A9-12ruf62ny5No ratings yet
- Optical Communication NetworksDocument4 pagesOptical Communication Networksarivurp100% (1)
- Sony Kdl32!37!40s5600 Chassis Ex2n-PeppermintDocument57 pagesSony Kdl32!37!40s5600 Chassis Ex2n-Peppermintvideoson100% (1)






















































































Download as pdf or txt
You might also like
- Ada CodesDocument9 pagesAda CodesEdna Jaquez0% (1)
- Meril Suture Catalogue Final Pages Deleted (1 24.40 44.50 64)Document44 pagesMeril Suture Catalogue Final Pages Deleted (1 24.40 44.50 64)threwaway75% (4)
- Dental Charting (Updated)Document56 pagesDental Charting (Updated)Rose Antoinette Umayam100% (1)
- CPT CodesDocument9 pagesCPT CodesSheree AnnNo ratings yet
- CDT 2017 - Code On Dental Proc - Nomenclature OnlineDocument20 pagesCDT 2017 - Code On Dental Proc - Nomenclature OnlineErwin FelipeNo ratings yet
- Ada CodesDocument4 pagesAda CodestedyNo ratings yet
- Drilling Fluids ManualDocument486 pagesDrilling Fluids ManualParaZzzit100% (12)
- Fee Schedule Yellow (A) UpdatedDocument2 pagesFee Schedule Yellow (A) Updatedade melly septianaNo ratings yet
- Fee Schedull Provider (Ace Dental)Document1 pageFee Schedull Provider (Ace Dental)primazamsaNo ratings yet
- 2013 CA Dental OverviewDocument6 pages2013 CA Dental OverviewsvlimNo ratings yet
- Cigna Dental Care Patient Charge Schedule: (Dhmo)Document16 pagesCigna Dental Care Patient Charge Schedule: (Dhmo)Susanta BeheraNo ratings yet
- Patient Encounter Form: Facility Number: Facility Name: Facility Address: NPI NumberDocument2 pagesPatient Encounter Form: Facility Number: Facility Name: Facility Address: NPI NumberJayNo ratings yet
- Orthodontic CDTDocument2 pagesOrthodontic CDTnaharmampillyNo ratings yet
- Translation of Current Dental Terminology American Dental Association (Updated July 2020)Document22 pagesTranslation of Current Dental Terminology American Dental Association (Updated July 2020)Nouran Ayman Mahmoud Kamal Mahmoud Ghonime Nouran Ayman Mahmoud Kamal Mahmoud GhonimeNo ratings yet
- CDT CodesDocument32 pagesCDT CodesTariq KhalidNo ratings yet
- Dental RVU Cookbook: Washington State Health Care AuthorityDocument9 pagesDental RVU Cookbook: Washington State Health Care AuthorityPaul GNo ratings yet
- Aetna Dental Low DmoDocument9 pagesAetna Dental Low DmoBeau PeskaNo ratings yet
- PMW 0031 2.19 PDFDocument13 pagesPMW 0031 2.19 PDFFelton Small Jr.No ratings yet
- MSBY Medical Package ListDocument32 pagesMSBY Medical Package ListSakshi G AwasthiNo ratings yet
- Screenshot 2023-01-25 at 15.07.02Document1 pageScreenshot 2023-01-25 at 15.07.02PikynelPykinescuNo ratings yet
- ADA Ortho CodesDocument1 pageADA Ortho CodesAmerican Aesthetic MCNo ratings yet
- UPCD Dental Services Clinical FeesDocument2 pagesUPCD Dental Services Clinical FeescreamyfrappeNo ratings yet
- 2023 ADA Code List For Microsoft PlansDocument54 pages2023 ADA Code List For Microsoft PlansAngelica PillaNo ratings yet
- Dent CPD KalbarDocument46 pagesDent CPD KalbarHardiansyah HardiNo ratings yet
- Important RQS:: Ait Is Asda Question and Answer Confirmed From Mastry AppDocument64 pagesImportant RQS:: Ait Is Asda Question and Answer Confirmed From Mastry AppParamjit KaurNo ratings yet
- PG Dental Fee and Seat 2020Document1 pagePG Dental Fee and Seat 2020Saurav SumanNo ratings yet
- Medicare Excel FileDocument22 pagesMedicare Excel FileshobhaNo ratings yet
- Company: Plan: XD04 Annual Fee:: CE Limited (博苗有限公司)Document2 pagesCompany: Plan: XD04 Annual Fee:: CE Limited (博苗有限公司)碌葛一No ratings yet
- 價目表 Price ListDocument3 pages價目表 Price ListPatrick WongNo ratings yet
- Life Line Dental Pricelist (Revised)Document6 pagesLife Line Dental Pricelist (Revised)drsobanNo ratings yet
- Dental PricingDocument4 pagesDental PricingsolutionbeautyNo ratings yet
- Translation of Current Dental Terminology American Dental Association (Updated July 2020)Document2 pagesTranslation of Current Dental Terminology American Dental Association (Updated July 2020)ABNo ratings yet
- 2022-Pricelist Feb2022 PDFDocument2 pages2022-Pricelist Feb2022 PDFjackNo ratings yet
- Cubierta Dental D-611 P.ideal C.P. 2Document4 pagesCubierta Dental D-611 P.ideal C.P. 2JessicaNo ratings yet
- Inbound 6373724171176570885Document19 pagesInbound 6373724171176570885Diácono Rui Cunha CamposNo ratings yet
- 2023 Dental Benefit Criteria GuidanceDocument18 pages2023 Dental Benefit Criteria GuidancebrennanandbrennanlawNo ratings yet
- Dental PlanDocument5 pagesDental PlanBhavna ChakrabortyNo ratings yet
- Ultrathin CAD-CAM Ceramic Occlusal Veneers and Anterior Bilaminar Veneers For The Treatment of Moderate Dental Biocorrosion: A 1.5-Year Follow-UpDocument10 pagesUltrathin CAD-CAM Ceramic Occlusal Veneers and Anterior Bilaminar Veneers For The Treatment of Moderate Dental Biocorrosion: A 1.5-Year Follow-Upharshal shetyeNo ratings yet
- TPA & INSURANCE Rates - HDFC eRGODocument2 pagesTPA & INSURANCE Rates - HDFC eRGORahul WaskelNo ratings yet
- Daftar Barang Yang Masuk Di Ekatalog 2019: No. Jenis Produk Nama Produk Merek Dan Type Produk HargaDocument7 pagesDaftar Barang Yang Masuk Di Ekatalog 2019: No. Jenis Produk Nama Produk Merek Dan Type Produk HargaRakhmayanto AbizulfaNo ratings yet
- LSG DentalDocument1 pageLSG Dentalres6250No ratings yet
- DtFLHumana FL HI215 11.2012Document6 pagesDtFLHumana FL HI215 11.2012jeff-swansonNo ratings yet
- CDocument4 pagesCdentcare.insuNo ratings yet
- Setoran Umum Gigi Mei 2022Document4 pagesSetoran Umum Gigi Mei 2022Agatha PutriNo ratings yet
- Bhamashah Swasthya Bima Yojana 2017-19: S. No. Final Package Name Package Type Proposed Rate Speciality Code Short NameDocument21 pagesBhamashah Swasthya Bima Yojana 2017-19: S. No. Final Package Name Package Type Proposed Rate Speciality Code Short Nameswastik hospitalNo ratings yet
- Mapping MGDocument4 pagesMapping MGdentcare.insuNo ratings yet
- Cobertura ODO562Document6 pagesCobertura ODO562Juan Manuel FerreroNo ratings yet
- COTATION AFCOTT CAM SARL - Fr.enDocument1 pageCOTATION AFCOTT CAM SARL - Fr.enMichel erickson talom waboNo ratings yet
- Price List CAB Dental 2016Document12 pagesPrice List CAB Dental 2016Fachrul Latif DentistNo ratings yet
- 2023 Pricelist Grey Gables Dental PracticeDocument2 pages2023 Pricelist Grey Gables Dental Practicevioleta.dan91No ratings yet
- Pc-1000 Panoramic X-Ray Service ManualDocument4 pagesPc-1000 Panoramic X-Ray Service ManualJosé Luís Cheo Barrios CristóbalNo ratings yet
- 2022 Republic Services REPU - 20221014Document2 pages2022 Republic Services REPU - 20221014kenneth.chronister9458No ratings yet
- ExodontiasDocument19 pagesExodontiasmameekasim75No ratings yet
- Unitedhealthcare Dental Ppo Plan 2022 Summary of Benefits and CoverageDocument1 pageUnitedhealthcare Dental Ppo Plan 2022 Summary of Benefits and CoverageAdam CliftonNo ratings yet
- Traducere in Engleza Site Spring Dental Mihaela VelcuDocument11 pagesTraducere in Engleza Site Spring Dental Mihaela VelcuFlorin Cornel VelcuNo ratings yet
- ArticleDocument8 pagesArticleMairaMaraviChavezNo ratings yet
- Harga Bahan DentalDocument19 pagesHarga Bahan Dentalarief hendra wijayaNo ratings yet
- Esthetic Oral Rehabilitation with Veneers: A Guide to Treatment Preparation and Clinical ConceptsFrom EverandEsthetic Oral Rehabilitation with Veneers: A Guide to Treatment Preparation and Clinical ConceptsRichard D. TrushkowskyNo ratings yet
- DENTURES: The Ultimate Guide to Dentures & Denture Care for a Beautifully Restored SmileFrom EverandDENTURES: The Ultimate Guide to Dentures & Denture Care for a Beautifully Restored SmileNo ratings yet
- Cone Beam Computed Tomography: Oral and Maxillofacial Diagnosis and ApplicationsFrom EverandCone Beam Computed Tomography: Oral and Maxillofacial Diagnosis and ApplicationsDavid SarmentNo ratings yet
- Digits and Widgets: (With Reference To A Wise Mother, The Golden BookDocument7 pagesDigits and Widgets: (With Reference To A Wise Mother, The Golden Bookloristahl8340No ratings yet
- Maintenance Manual SinotruckDocument21 pagesMaintenance Manual SinotruckCôn LuânNo ratings yet
- A Recommender System Based On PersonalDocument15 pagesA Recommender System Based On Personalreiko-sanNo ratings yet
- EscortsDocument59 pagesEscortsVijay Malik100% (2)
- Double Wedding Ring Size Fabric Requirements EditedDocument3 pagesDouble Wedding Ring Size Fabric Requirements EditedfrapatchNo ratings yet
- District CalendarDocument1 pageDistrict Calendarapi-271737972No ratings yet
- PPG TestDocument2 pagesPPG TestAljon MendozaNo ratings yet
- Bryce Boerste - Personal College Essay - Draft 2Document3 pagesBryce Boerste - Personal College Essay - Draft 2api-492128881No ratings yet
- Logging InnovationDocument8 pagesLogging InnovationAnkit ChourasiaNo ratings yet
- Prelims-Arche 4 Sy 2122-StudentsDocument3 pagesPrelims-Arche 4 Sy 2122-StudentsAaron CansinoNo ratings yet
- Democratization of Secondary School in MalaysiaDocument12 pagesDemocratization of Secondary School in MalaysiaKavinesh Kaneson100% (1)
- Deteqstandart PDFDocument4 pagesDeteqstandart PDFMoaed KanbarNo ratings yet
- Proverbs 18-24 Ronnie LoudermilkDocument1 pageProverbs 18-24 Ronnie LoudermilkKeneth Chris NamocNo ratings yet
- 8 Fall of The Ottoman EmpireDocument10 pages8 Fall of The Ottoman Empireapi-303147801No ratings yet
- Load Cell Input ModuleDocument3 pagesLoad Cell Input Moduleabo omrNo ratings yet
- Classroom Accommodations For Students With Learning Difficulties and DisabilitiesDocument2 pagesClassroom Accommodations For Students With Learning Difficulties and Disabilitiesapi-359063455No ratings yet
- Indian Heart JournalDocument18 pagesIndian Heart JournalSanaSofiyahNo ratings yet
- Tushar Kumar B P Operating Systems Digital Assignment-2Document5 pagesTushar Kumar B P Operating Systems Digital Assignment-2Chirosuke TashiNo ratings yet
- SCADA System PDFDocument420 pagesSCADA System PDFbambang_gastomoNo ratings yet
- Freezing Baked GoodsDocument9 pagesFreezing Baked GoodsBenjamin DoverNo ratings yet
- Missalette FINAL PDFDocument32 pagesMissalette FINAL PDFJohnpaul MenchavezNo ratings yet
- Thời gian làm bài 120 phút, không kể thời gian giao đềDocument9 pagesThời gian làm bài 120 phút, không kể thời gian giao đềĐỗ Hoàng DũngNo ratings yet
- Solucion Listening Unit 5Document2 pagesSolucion Listening Unit 5ManoloNo ratings yet
- Study Guide For Tanizaki Jun'ichirō "The Secret" (Himitsu, 1911, Tr. A. Chambers)Document3 pagesStudy Guide For Tanizaki Jun'ichirō "The Secret" (Himitsu, 1911, Tr. A. Chambers)BeholdmyswarthyfaceNo ratings yet
- To Biochemistry: Murang'a University of TechnologyDocument6 pagesTo Biochemistry: Murang'a University of TechnologyJoseph NyabugaNo ratings yet
- Marketing Advanced HW 3 A5-7, A9-12Document3 pagesMarketing Advanced HW 3 A5-7, A9-12ruf62ny5No ratings yet
- Optical Communication NetworksDocument4 pagesOptical Communication Networksarivurp100% (1)
- Sony Kdl32!37!40s5600 Chassis Ex2n-PeppermintDocument57 pagesSony Kdl32!37!40s5600 Chassis Ex2n-Peppermintvideoson100% (1)