Download as pdf or txt
You might also like
- Bangalore PeenyaDocument4 pagesBangalore Peenyaravishankar78% (9)
- Chronic Suppurative Otitis Media in AdultsDocument10 pagesChronic Suppurative Otitis Media in AdultsRstadam TagalogNo ratings yet
- CPG On CsomDocument8 pagesCPG On CsomRobert Ross DulayNo ratings yet
- Jurnal THT NiaDocument5 pagesJurnal THT NianiajaplaniNo ratings yet
- 9009 44225 1 PB PDFDocument5 pages9009 44225 1 PB PDFwandajunitasNo ratings yet
- Research Article: Tympanometric Findings Among Children With Adenoid Hypertrophy in Port Harcourt, NigeriaDocument4 pagesResearch Article: Tympanometric Findings Among Children With Adenoid Hypertrophy in Port Harcourt, NigeriaDwi Ayu KusumawardaniNo ratings yet
- Sinonasal Polyposis and Fungus:A Growing RelationshipDocument5 pagesSinonasal Polyposis and Fungus:A Growing RelationshipMariam AslamNo ratings yet
- Hearing Loss in Children With Otitis Media With Effusion A Systematic ReviewDocument14 pagesHearing Loss in Children With Otitis Media With Effusion A Systematic ReviewTrần Văn TâmNo ratings yet
- Adenoid Hypertrophy in Adult Patients and Its Relation With Various FactorsDocument3 pagesAdenoid Hypertrophy in Adult Patients and Its Relation With Various FactorsshanizaNo ratings yet
- VCS 8Document6 pagesVCS 8Carolina UrrutiaNo ratings yet
- Removal of Foreign Body (Denture) in Esophagus With Rigid EsophagoscopeDocument6 pagesRemoval of Foreign Body (Denture) in Esophagus With Rigid EsophagoscopetaagrettaaNo ratings yet
- Adenoid HipertrofiDocument6 pagesAdenoid HipertrofirahmaputraNo ratings yet
- Electronic Physician (ISSN: 2008-5842) : 1.1. BackgroundDocument5 pagesElectronic Physician (ISSN: 2008-5842) : 1.1. BackgroundFi NoNo ratings yet
- Relation Between Adenoid Size and Otitis Media With EffusionDocument4 pagesRelation Between Adenoid Size and Otitis Media With EffusionnadaNo ratings yet
- A Clinicopathological Study of Supraglottic Malignancy at A Tertiary Care Centre in Central India - May - 2023 - 1448516048 - 6309584Document3 pagesA Clinicopathological Study of Supraglottic Malignancy at A Tertiary Care Centre in Central India - May - 2023 - 1448516048 - 6309584surgeonforlifeNo ratings yet
- S 410Document6 pagesS 410Boca PetualangNo ratings yet
- Journal Pone 0193913Document10 pagesJournal Pone 0193913tiara nadya putriandaNo ratings yet
- AsdfasfasDocument5 pagesAsdfasfasHusain RezaNo ratings yet
- Comparison of Endoscopic Cartilage Myringoplasty in Dry and Wet Ears With Chronic Suppurative Otitis MediaDocument6 pagesComparison of Endoscopic Cartilage Myringoplasty in Dry and Wet Ears With Chronic Suppurative Otitis MediafatinfatharaniNo ratings yet
- Ceo 3 110 PDFDocument5 pagesCeo 3 110 PDFCut Nanda FitriNo ratings yet
- Otolaryngology Service Usage in Children With Cleft PalateDocument4 pagesOtolaryngology Service Usage in Children With Cleft PalateCatherine nOCUANo ratings yet
- Management of Common Voice DisordersDocument16 pagesManagement of Common Voice Disordersrowin93No ratings yet
- 10 1016@j Ijporl 2019 06 019Document7 pages10 1016@j Ijporl 2019 06 019Eva PerdanaNo ratings yet
- Endoscopic Examination of The Nasal Cavity and Nasopharynx in Patients With Otitis MediaDocument8 pagesEndoscopic Examination of The Nasal Cavity and Nasopharynx in Patients With Otitis Mediagemala wahabNo ratings yet
- Evaluation of Type I Tympanoplasty in Children in Upper Egypt 2161 119X 100Document5 pagesEvaluation of Type I Tympanoplasty in Children in Upper Egypt 2161 119X 100Yogi Ardhi IrafaniNo ratings yet
- Upper Airway Obstructions and Chronic Otitis Media: A Clinical StudyDocument4 pagesUpper Airway Obstructions and Chronic Otitis Media: A Clinical StudyMuhammadImamNo ratings yet
- A Retrospective Review of Complicated Foreign BodiDocument5 pagesA Retrospective Review of Complicated Foreign Bodimanoj kumarNo ratings yet
- J Voice 2019 33 5 708-711Document4 pagesJ Voice 2019 33 5 708-711baltazarottonelloNo ratings yet
- Research: Pattern of Otitis Externa in Kaduna NigeriaDocument4 pagesResearch: Pattern of Otitis Externa in Kaduna NigeriaRicky AmeNo ratings yet
- Serous Otitis Media Clinical and Therapeutic ConsiDocument5 pagesSerous Otitis Media Clinical and Therapeutic Consiheidi leeNo ratings yet
- PARS Reader's Digest - July 2013 IssueDocument9 pagesPARS Reader's Digest - July 2013 Issueinfo8673No ratings yet
- Ohki2019 PDFDocument9 pagesOhki2019 PDFajaymanvikar007No ratings yet
- Jurnal OMSK 1Document12 pagesJurnal OMSK 1Ani SeptyaningsihNo ratings yet
- d098 PDFDocument7 pagesd098 PDFMayiz Renata LimerseNo ratings yet
- Tubercular Otitis Media: Demystifying Its Nuances and An Update On The Tenets of Emerging PerspectivesDocument9 pagesTubercular Otitis Media: Demystifying Its Nuances and An Update On The Tenets of Emerging PerspectivesAditya HendraNo ratings yet
- Parapharyngeal Abscess in Children - Five Year Retrospective StudyDocument5 pagesParapharyngeal Abscess in Children - Five Year Retrospective StudyciciNo ratings yet
- Traumatic Perforations of Tympanic Membrane: Our Experience: Original Research ArticleDocument4 pagesTraumatic Perforations of Tympanic Membrane: Our Experience: Original Research ArticleXlr8zzNo ratings yet
- Article 2.2Document9 pagesArticle 2.2jessika yanceNo ratings yet
- Medip,+15 59 1 CEDocument7 pagesMedip,+15 59 1 CEKabir Ahmed LaskarNo ratings yet
- A Prospective Study of Sinonasal and Nasopharyngeal Pathology in Chronic Otitis MediaDocument5 pagesA Prospective Study of Sinonasal and Nasopharyngeal Pathology in Chronic Otitis MediaAmalia OkvitariandariNo ratings yet
- 1191 4833 2 PBDocument6 pages1191 4833 2 PBWilson WibisonoNo ratings yet
- Article in Press: Journal of Oral and Maxillofacial Surgery, Medicine, and PathologyDocument7 pagesArticle in Press: Journal of Oral and Maxillofacial Surgery, Medicine, and PathologyNizajaulNo ratings yet
- Correlation Between Sensorineural Hearing Loss andDocument5 pagesCorrelation Between Sensorineural Hearing Loss andWilson WibisonoNo ratings yet
- Bmri2021 5550267Document13 pagesBmri2021 5550267Shahid ShaikhNo ratings yet
- Xu 2020Document6 pagesXu 2020Cintya RambuNo ratings yet
- Ear, Nose and Throat Foreign Bodies Removed Under General Anaesthesia: A Retrospective StudyDocument4 pagesEar, Nose and Throat Foreign Bodies Removed Under General Anaesthesia: A Retrospective StudyAulia NurrahmahNo ratings yet
- Adenoid Radiologic MeasurementDocument5 pagesAdenoid Radiologic MeasurementfantamerahNo ratings yet
- Otolaryngological Manifestations in Hiv Infected Patients Tehran Iran 2155 6113.1000160Document4 pagesOtolaryngological Manifestations in Hiv Infected Patients Tehran Iran 2155 6113.1000160Adhelline RansunNo ratings yet
- Safety of Tongue Base Procedures For Sleep Apnoea in Adults: A Systematic Review and Metanalysis From The Yo-Ifos Study GroupDocument10 pagesSafety of Tongue Base Procedures For Sleep Apnoea in Adults: A Systematic Review and Metanalysis From The Yo-Ifos Study GroupIñaki ErdozáinNo ratings yet
- 2018 Article 1359Document5 pages2018 Article 1359SaskiahNo ratings yet
- Predisposing Factors For The Complications of Deep Neck InfectionDocument6 pagesPredisposing Factors For The Complications of Deep Neck InfectionAndy ShariffNo ratings yet
- Jurnal 3Document6 pagesJurnal 3Dheana IsmaniarNo ratings yet
- Association Between Otitis Media and Gastroesophageal Reflux: A Systematic ReviewDocument8 pagesAssociation Between Otitis Media and Gastroesophageal Reflux: A Systematic Reviewputri balqisNo ratings yet
- Dreyer - Et - Al-2018-J Periodon ResDocument25 pagesDreyer - Et - Al-2018-J Periodon ResAFKs GamerNo ratings yet
- Emergency Medicine:: Pediatric Deep Neck Space Abscesses: A Prospective Observational StudyDocument6 pagesEmergency Medicine:: Pediatric Deep Neck Space Abscesses: A Prospective Observational StudyG Virucha Meivila IINo ratings yet
- Adenoid HipertropiDocument6 pagesAdenoid HipertropiTeuku AndyNo ratings yet
- Allergic Rhinitis in Adults With Chronic Suppurative Otitis MediaDocument6 pagesAllergic Rhinitis in Adults With Chronic Suppurative Otitis MediaBayu WidhiarsaNo ratings yet
- International Journal of Pediatric OtorhinolaryngologyDocument5 pagesInternational Journal of Pediatric OtorhinolaryngologyAcoet MiezarNo ratings yet
- Respirador BucalDocument8 pagesRespirador Bucalyessenia armijosNo ratings yet
- Examination of Ulcero-Proliferative Lesions of Oropharynx and Oral Cavity - A Clinical PerspectiveDocument7 pagesExamination of Ulcero-Proliferative Lesions of Oropharynx and Oral Cavity - A Clinical PerspectiveInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- OHNS--Otolaryngology; Head and Neck surgery: pocket field guideFrom EverandOHNS--Otolaryngology; Head and Neck surgery: pocket field guideNo ratings yet
- Functional Safety and IEC 61508 A Basic Guide PDFDocument9 pagesFunctional Safety and IEC 61508 A Basic Guide PDFfitasmounirNo ratings yet
- WantedDocument4 pagesWantedMansoor TheenNo ratings yet
- 6. 350-500FR2英文TSM50663-02 - 631461 - 705Document49 pages6. 350-500FR2英文TSM50663-02 - 631461 - 705Hernando Fang PedrozaNo ratings yet
- Aggregate Impact ValueDocument4 pagesAggregate Impact ValuevinoNo ratings yet
- Summation of The Sciencemadness Phosphorous ThreadDocument29 pagesSummation of The Sciencemadness Phosphorous ThreadImranNo ratings yet
- 350 ML (Amount of Beer) × 0.05 (Alcoholic Content) × 0.792 (Alcoholic Density) 13.860 G Theoretical Blood Alcohol Concentration 13,860 MG / 52,500 ML 0.264 MG/MLDocument5 pages350 ML (Amount of Beer) × 0.05 (Alcoholic Content) × 0.792 (Alcoholic Density) 13.860 G Theoretical Blood Alcohol Concentration 13,860 MG / 52,500 ML 0.264 MG/MLSava VijakNo ratings yet
- USS Springfield Sailor Receives Proclamation From Ledyard Mayor For Act of HeroismDocument8 pagesUSS Springfield Sailor Receives Proclamation From Ledyard Mayor For Act of HeroismdolphingrlzNo ratings yet
- Gun Water PDFDocument4 pagesGun Water PDFAlejandro MontecilloNo ratings yet
- Car List Ecu DimsportDocument421 pagesCar List Ecu DimsportJames wilder llican sanchezNo ratings yet
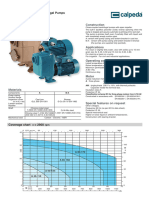
- 1 - A 40-110A - B Self-Priming Centrifugal PumpDocument6 pages1 - A 40-110A - B Self-Priming Centrifugal Pump3dpshabbirNo ratings yet
- CIS Electrical Standard Rev 001Document46 pagesCIS Electrical Standard Rev 001Tarek AbulailNo ratings yet
- Workbook Grade 11&12 English-1Document40 pagesWorkbook Grade 11&12 English-1Kamil Ali33% (3)
- Academy of Economic Studies of Moldova: Performed by Artur CatanoiDocument3 pagesAcademy of Economic Studies of Moldova: Performed by Artur CatanoiArtur CatanoiNo ratings yet
- Multi-Split Type Air Conditioners: DC Inverter Control Cooling Only and Reverse Cycle 50 HZDocument31 pagesMulti-Split Type Air Conditioners: DC Inverter Control Cooling Only and Reverse Cycle 50 HZvphuc1984No ratings yet
- Mental ManipulationDocument2 pagesMental ManipulationSunčica Nisam100% (2)
- Medicine Triple ADocument186 pagesMedicine Triple AAnup Bhele100% (1)
- 460 Lesson PlanDocument5 pages460 Lesson Planapi-237881244No ratings yet
- Fluorescence SpectrosDocument52 pagesFluorescence Spectroshafsa BNo ratings yet
- EMPM5103-PQMP Assignment - Part BDocument60 pagesEMPM5103-PQMP Assignment - Part Bnorizam32100% (2)
- ME-52023 Internal Combustion Engines: Technological University (Hmawbi) Department of Mechanical EngineeringDocument25 pagesME-52023 Internal Combustion Engines: Technological University (Hmawbi) Department of Mechanical EngineeringSi Thu Aung100% (1)
- C1-Introduction To MobileDocument10 pagesC1-Introduction To MobileRheden GimenaNo ratings yet
- Recount Text MATERI X TSM 3 TGL 142019Document3 pagesRecount Text MATERI X TSM 3 TGL 142019smkn 8 jemberNo ratings yet
- Resume 1Document1 pageResume 1api-336472593No ratings yet
- Sales Executives Promote Products and Services To Customers and Negotiate Contracts With The Aim of Maximising ProfitsDocument2 pagesSales Executives Promote Products and Services To Customers and Negotiate Contracts With The Aim of Maximising ProfitsNikhil MauryaNo ratings yet
- TKN - VELP Application NoteDocument4 pagesTKN - VELP Application NoteAshraf MohamedNo ratings yet
- Kirloskar Brothers LimitedDocument36 pagesKirloskar Brothers Limitedgopalakrishnannrm1202No ratings yet
- Sade SatiDocument6 pagesSade SatiRavi GoyalNo ratings yet
- Air Quality Impacts of Biodiesel in The European UnionDocument2 pagesAir Quality Impacts of Biodiesel in The European UnionThe International Council on Clean TransportationNo ratings yet
- Fine Love Dolls User ManualDocument11 pagesFine Love Dolls User ManualFine Love Dolls (Ultra Realistic TPE Dolls)33% (3)