Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Understanding LORMS in SBQDocument12 pagesUnderstanding LORMS in SBQshahrilmohdshah100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
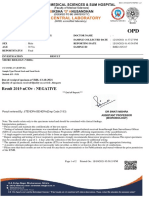
- Patient Name Doctor Name Pat Reg Id Sample Collected Date SEX Reporting Date AGE Sample Id ReportstatusDocument2 pagesPatient Name Doctor Name Pat Reg Id Sample Collected Date SEX Reporting Date AGE Sample Id ReportstatusThushar P kumarNo ratings yet
- Moniginis Case StudyDocument11 pagesMoniginis Case StudyNikhil AroraNo ratings yet
- P2X3 Receptor Expression in Dorsal Horn of Spinal Cord and Pain Threshold After Estrogen Therapy For Prevention Therapy in Neuropathic PainDocument7 pagesP2X3 Receptor Expression in Dorsal Horn of Spinal Cord and Pain Threshold After Estrogen Therapy For Prevention Therapy in Neuropathic PainInggitaDarmawanNo ratings yet
- Annals of Medicine and SurgeryDocument7 pagesAnnals of Medicine and SurgeryInggitaDarmawanNo ratings yet
- Role of MLC901 in Increasing Neurogenesis in Rats With Traumatic Brain InjuryDocument5 pagesRole of MLC901 in Increasing Neurogenesis in Rats With Traumatic Brain InjuryInggitaDarmawanNo ratings yet
- Annals of Medicine and Surgery: Cohort StudyDocument6 pagesAnnals of Medicine and Surgery: Cohort StudyInggitaDarmawanNo ratings yet
- Ear Trauma: Kylee Eagles,, Laura Fralich,, J. Herbert StevensonDocument14 pagesEar Trauma: Kylee Eagles,, Laura Fralich,, J. Herbert StevensonInggitaDarmawanNo ratings yet
- The Worldwide Incidence of Neonaticide: A Systematic ReviewDocument8 pagesThe Worldwide Incidence of Neonaticide: A Systematic ReviewInggitaDarmawanNo ratings yet
- Refractive Errors Among School Children in Addis Ababa EthiopiaDocument6 pagesRefractive Errors Among School Children in Addis Ababa EthiopiaInggitaDarmawanNo ratings yet
- Update On Astigmatism ManagementDocument5 pagesUpdate On Astigmatism ManagementInggitaDarmawanNo ratings yet
- Syntax ScoreDocument10 pagesSyntax ScoreInggitaDarmawanNo ratings yet
- Leukemia & LymphomaDocument6 pagesLeukemia & LymphomaInggitaDarmawanNo ratings yet
- The High Prevalence of Low HDL-Cholesterol Levels and Dyslipidemia in Rural Populations in Northwestern ChinaDocument13 pagesThe High Prevalence of Low HDL-Cholesterol Levels and Dyslipidemia in Rural Populations in Northwestern ChinaInggitaDarmawanNo ratings yet
- Vaginal DischargeDocument7 pagesVaginal DischargeInggitaDarmawanNo ratings yet
- High Density Lipoprotein Structure-Function and Role in Reverse Cholesterol TransportDocument44 pagesHigh Density Lipoprotein Structure-Function and Role in Reverse Cholesterol TransportInggitaDarmawanNo ratings yet
- Eph GestosisDocument9 pagesEph GestosisInggitaDarmawanNo ratings yet
- A1 English Listening Test - What Is Your JobDocument6 pagesA1 English Listening Test - What Is Your JobTrang NguyenNo ratings yet
- To BeDocument7 pagesTo BeSamuel Celedonio RodriguezNo ratings yet
- Operating Room TechniqueDocument2 pagesOperating Room TechniqueDENNROSE DECLARONo ratings yet
- 1 Intermolecular InteractionsDocument64 pages1 Intermolecular InteractionsAz Zahra Assyifa UshwahNo ratings yet
- Final Report 4, Temperature Control PDFDocument30 pagesFinal Report 4, Temperature Control PDFmelanNo ratings yet
- 067 People v. DalawisDocument2 pages067 People v. DalawisRS SuyosaNo ratings yet
- Selection and Grading of ContentDocument36 pagesSelection and Grading of ContentAli Gamil100% (1)
- 1Document4 pages1Surya TejaNo ratings yet
- Ambag Ni Dexter Beig Sa Meridian HehezDocument4 pagesAmbag Ni Dexter Beig Sa Meridian HehezALLYSSA JEAN ASCANNo ratings yet
- List of Private B.Ed. Colleges of Assam Recognized by NCTE (Approved Intake Capacity) For The Year (2017-18)Document4 pagesList of Private B.Ed. Colleges of Assam Recognized by NCTE (Approved Intake Capacity) For The Year (2017-18)munmun islamNo ratings yet
- The Steak N Shake Company Code of Business Conduct and EthicsDocument16 pagesThe Steak N Shake Company Code of Business Conduct and Ethicsapi-355261274No ratings yet
- Capital One Doing Business The Digital Way 0Document7 pagesCapital One Doing Business The Digital Way 0Santanu MukherjeeNo ratings yet
- Doing InterviewsDocument10 pagesDoing InterviewsmorningstxrrNo ratings yet
- Hazrat Sumayyah Bint KhayyatDocument4 pagesHazrat Sumayyah Bint KhayyatMom MareemNo ratings yet
- 2) There Was A Murder Last Night. What Were They Doing When The Murder Happened?Document2 pages2) There Was A Murder Last Night. What Were They Doing When The Murder Happened?Pilar Gonzalez PinillaNo ratings yet
- Revised Corporation Code of The PhilippinesDocument15 pagesRevised Corporation Code of The PhilippinesStarr Weigand100% (8)
- Parabola: Property of Cid - Deped Lipa City Under Learning From Home Scheme 2020Document20 pagesParabola: Property of Cid - Deped Lipa City Under Learning From Home Scheme 2020Charles Acielo100% (1)
- Fin Man HW1Document3 pagesFin Man HW1KingkongNo ratings yet
- Lesson Plan-Test Taking FinalDocument7 pagesLesson Plan-Test Taking FinalStefanNo ratings yet
- Bo5550077 PDFDocument4 pagesBo5550077 PDFBlagoje0% (1)
- 09 Chapter IDocument45 pages09 Chapter ISYED TAYYABNo ratings yet
- Ethics in PracticeDocument14 pagesEthics in PracticedanielktingNo ratings yet
- Vasoline Bass (Ver 4) by Stone Temple Pilotstabs at Ultimate Guitar ArchiveDocument7 pagesVasoline Bass (Ver 4) by Stone Temple Pilotstabs at Ultimate Guitar ArchiveJazz QuevedoNo ratings yet
- Master Thesis Mit TemplateDocument7 pagesMaster Thesis Mit Templateafloattaxmxufr100% (2)
- DMRC Procurement Manual 2012Document53 pagesDMRC Procurement Manual 2012Cane CirpoNo ratings yet
- Infrasound Recording SystemDocument7 pagesInfrasound Recording SystemarunpdnNo ratings yet
- Defense of The AncientsDocument3 pagesDefense of The AncientsNissa CleopatraNo ratings yet