Download as pdf or txt
You might also like
- ACLS Exam - A&B VersionsDocument36 pagesACLS Exam - A&B VersionsMohamed El-sayed100% (1)
- Ghaffarian2018 PDFDocument4 pagesGhaffarian2018 PDFIgor PiresNo ratings yet
- 480 FullDocument6 pages480 FullStamenko S. SusakNo ratings yet
- Pi Is 0003497500014818Document7 pagesPi Is 0003497500014818GKNo ratings yet
- Ali TransechoDocument2 pagesAli TransechoUtama Hadiputra SurbaktiNo ratings yet
- ArtigosDocument6 pagesArtigosIgor PiresNo ratings yet
- Type A Interrupted Aortic Arch With Taussig Bing Anomaly Case ReportDocument3 pagesType A Interrupted Aortic Arch With Taussig Bing Anomaly Case Reportchidiebere peter echiehNo ratings yet
- Nejmvcm 2004089Document7 pagesNejmvcm 2004089julian zuletaNo ratings yet
- Hybrid Repair of Aortic Arch AneurysmDocument8 pagesHybrid Repair of Aortic Arch AneurysmFrancesca MazzolaniNo ratings yet
- Reduction Aortoplasty and External Wrapping For Moderately Sized Tubular Ascending Aortic Aneurysm With Concomitant OperationsDocument4 pagesReduction Aortoplasty and External Wrapping For Moderately Sized Tubular Ascending Aortic Aneurysm With Concomitant OperationsRadioputro WicaksonoNo ratings yet
- Belhajsoulami 2018Document3 pagesBelhajsoulami 2018rédaNo ratings yet
- Resection of A Giant Mediastinal Teratoma: CommentDocument2 pagesResection of A Giant Mediastinal Teratoma: Commentflik_gantengNo ratings yet
- Cor Triatriatum With Persistent Levoatrial CardinaDocument4 pagesCor Triatriatum With Persistent Levoatrial CardinaAFJimenezONo ratings yet
- Severe Pelvic Fracture With Profound Hypotension: A Case Report and Treatment AlgorithmDocument3 pagesSevere Pelvic Fracture With Profound Hypotension: A Case Report and Treatment AlgorithmodyNo ratings yet
- 1 s2.0 S2210261223011938 MainDocument3 pages1 s2.0 S2210261223011938 Mainkalebberhane9No ratings yet
- MJMHS 1316Document3 pagesMJMHS 1316prima ningratNo ratings yet
- Omar 2014Document5 pagesOmar 2014Fede WeckesserNo ratings yet
- Kim2012Document5 pagesKim2012Stefanie MelisaNo ratings yet
- Jocs.15492 Articulo KozirevDocument7 pagesJocs.15492 Articulo KozirevCorazon MabelNo ratings yet
- CABG x4Document2 pagesCABG x4Indranil SinhaNo ratings yet
- Aaa RotoDocument11 pagesAaa RotoKarely TapiaNo ratings yet
- Alexandria Journal of Medicine: Rehab Abdel Rahman El BakryDocument5 pagesAlexandria Journal of Medicine: Rehab Abdel Rahman El BakrySatrio Budi WicaksonoNo ratings yet
- Journal of Cardiothoracic Surgery Journal of Cardiothoracic SurgeryDocument12 pagesJournal of Cardiothoracic Surgery Journal of Cardiothoracic SurgeryFendry KolondamNo ratings yet
- Chen 2018Document16 pagesChen 2018Jade GomitaNo ratings yet
- Modified Selective Aortic RootDocument7 pagesModified Selective Aortic RootDm LdNo ratings yet
- Transaortic Valve ReplacementDocument11 pagesTransaortic Valve ReplacementManuela CulicaNo ratings yet
- Criss-Cross Heart With Double-Outlet Right VentricleDocument4 pagesCriss-Cross Heart With Double-Outlet Right Ventriclejuana lopezNo ratings yet
- Congenital Absence of The Deep Inferior EpigastricDocument4 pagesCongenital Absence of The Deep Inferior EpigastricTanulNo ratings yet
- 1 s2.0 S0003497516304921 MainDocument8 pages1 s2.0 S0003497516304921 MainEnrique San NorbertoNo ratings yet
- Reoperative Aortic Valve Replacement After PreviousCoronary Artery Bypass Grafting or Aortic Valve ReplacementDocument18 pagesReoperative Aortic Valve Replacement After PreviousCoronary Artery Bypass Grafting or Aortic Valve Replacement.No ratings yet
- DeNino (2014)Document11 pagesDeNino (2014)Stefanie MelisaNo ratings yet
- KalangosDocument3 pagesKalangosCorazon MabelNo ratings yet
- A Modification of The Swenson Operation For Congenital MegacolonDocument8 pagesA Modification of The Swenson Operation For Congenital MegacolonGunduz AgaNo ratings yet
- Best Management in Isolated Right Ventricular Hypoplasia With Septal Defects in AdultsDocument7 pagesBest Management in Isolated Right Ventricular Hypoplasia With Septal Defects in AdultsReinaldi octaNo ratings yet
- Pi Is 0022522312015267Document9 pagesPi Is 0022522312015267Riani NazilaNo ratings yet
- Ailoaei Et Al 2021 Zero Fluoroscopy Ablation For Atrial Re Entry Via A Vein of Marshall Connection Using A VisibleDocument5 pagesAiloaei Et Al 2021 Zero Fluoroscopy Ablation For Atrial Re Entry Via A Vein of Marshall Connection Using A VisibleAndrés AllaucaNo ratings yet
- Pi Is 1522294218300734Document19 pagesPi Is 1522294218300734William MakdinataNo ratings yet
- Pedicle AutologousDocument3 pagesPedicle AutologousSoftwarebolivia EnriqueNo ratings yet
- Visual Diagnosis in Emergency Medicine: Hydropneumothorax and Trapped LungDocument2 pagesVisual Diagnosis in Emergency Medicine: Hydropneumothorax and Trapped LungJha BhoenkNo ratings yet
- Orthotopic Heart Trans-Plantation in A Patient With D-Transposition of The Great ArteriesDocument4 pagesOrthotopic Heart Trans-Plantation in A Patient With D-Transposition of The Great ArteriesLaura OrozcoNo ratings yet
- FormosJSurg51250-7751411 213154Document8 pagesFormosJSurg51250-7751411 213154Deddy WidjajaNo ratings yet
- 1 Thoracic and Abdominal AneurysmDocument37 pages1 Thoracic and Abdominal AneurysmErneslito LucasNo ratings yet
- A Complete LBBB Revealing Non Specific Venous Metastasis Into The Right Atrium: A Case Report and Review of LiteratureDocument7 pagesA Complete LBBB Revealing Non Specific Venous Metastasis Into The Right Atrium: A Case Report and Review of LiteratureIJAR JOURNALNo ratings yet
- ChiesaDocument9 pagesChiesaserena7205No ratings yet
- Surgical Management of Tracheal Compression Caused by Mediastinal Goiter: Is Extracorporeal Circulation Requisite钥Document3 pagesSurgical Management of Tracheal Compression Caused by Mediastinal Goiter: Is Extracorporeal Circulation Requisite钥Indra W SaputraNo ratings yet
- Long-Term Outcomes After Valve-Sparing Anatomical Aortic Root Reconstruction in Acute Dissection Involving The RootDocument10 pagesLong-Term Outcomes After Valve-Sparing Anatomical Aortic Root Reconstruction in Acute Dissection Involving The RootMaghfirah MahmuddinNo ratings yet
- Letters To The Editor: Pulmonary Atresia With Intact Ventricular SeptumDocument2 pagesLetters To The Editor: Pulmonary Atresia With Intact Ventricular SeptumanindiawNo ratings yet
- Anastasiadou Trombose Aneurisma2017Document4 pagesAnastasiadou Trombose Aneurisma2017Margarita AucejoNo ratings yet
- Medical Devices of The ChestDocument22 pagesMedical Devices of The ChestJose David Flores PérezNo ratings yet
- Vargas 1985Document4 pagesVargas 1985Jose YoveraNo ratings yet
- Central Venous Catheterization: To The EditorDocument3 pagesCentral Venous Catheterization: To The Editordrpiratheepan4274No ratings yet
- Suh 2016Document4 pagesSuh 2016wahyuningsihNo ratings yet
- A Case Report On Middle Cerebral Artery Aneurysm.44Document5 pagesA Case Report On Middle Cerebral Artery Aneurysm.44SuNil AdhiKariNo ratings yet
- An Unusual Source of Tension - ChestDocument5 pagesAn Unusual Source of Tension - ChestKaran KalraNo ratings yet
- Cavotricuspid Isthmus: Anatomy, Electrophysiology, and Long-Term OutcomeDocument5 pagesCavotricuspid Isthmus: Anatomy, Electrophysiology, and Long-Term Outcomeapi-26166949No ratings yet
- F 6 Faa 026 Fca 60 C 4 F 4 C 89Document18 pagesF 6 Faa 026 Fca 60 C 4 F 4 C 89api-684047665No ratings yet
- Apm 12 151 PDFDocument4 pagesApm 12 151 PDFFityan Aulia RahmanNo ratings yet
- Sudden Hypotension Occurring After 4 Days of Left-Sided Central Catheter PlacementDocument3 pagesSudden Hypotension Occurring After 4 Days of Left-Sided Central Catheter PlacementFaqih SultonfaqNo ratings yet
- Case Report Missed Connections: Identification of Atrial Septal Defect by MRIDocument4 pagesCase Report Missed Connections: Identification of Atrial Septal Defect by MRIMuhammad Nur Ardhi LahabuNo ratings yet
- J HLC 2020 09 872Document2 pagesJ HLC 2020 09 872aswedi nersNo ratings yet
- Cardiac Surgical Operative AtlasFrom EverandCardiac Surgical Operative AtlasThorsten WahlersNo ratings yet
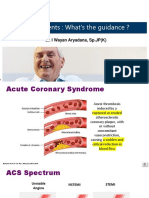
- Slide WS ACS Dr. Wayan Aryadana SP - JP (K) - WS 1Document26 pagesSlide WS ACS Dr. Wayan Aryadana SP - JP (K) - WS 1Luh Leni AriniNo ratings yet
- Atrial FibrillationDocument21 pagesAtrial FibrillationAndrea LombiNo ratings yet
- RUMUSDocument1 pageRUMUSdevinaNo ratings yet
- RHEUMATIC HEART DISEASE PPT (Autosaved)Document44 pagesRHEUMATIC HEART DISEASE PPT (Autosaved)abid AliNo ratings yet
- 30th ASMIHA Abstract AnnouncementDocument31 pages30th ASMIHA Abstract AnnouncementMora LubisNo ratings yet
- Journal Reading CKDDocument19 pagesJournal Reading CKDSyah Muhammad RezaNo ratings yet
- The ADEMEX Study Make Haste Slowly.35Document4 pagesThe ADEMEX Study Make Haste Slowly.35Arista RachmaNo ratings yet
- Li (2021) - Human RyR2 (Ryanodine Receptor 2) Loss-of-Function MutationsDocument12 pagesLi (2021) - Human RyR2 (Ryanodine Receptor 2) Loss-of-Function MutationsbalounovaNo ratings yet
- Renal - Goljan SlidesDocument29 pagesRenal - Goljan SlidesJoan ChoiNo ratings yet
- Poster 10 PALS 01 01 ENG V20100927 PDFDocument1 pagePoster 10 PALS 01 01 ENG V20100927 PDFAndy XiaoNo ratings yet
- Aortic RegurgitationDocument18 pagesAortic RegurgitationPukar GhimireNo ratings yet
- Chapter 28: Management of Patients With Structural, Infectious, and Inflammatory Cardiac DisordersDocument19 pagesChapter 28: Management of Patients With Structural, Infectious, and Inflammatory Cardiac DisordersBrian BileckyNo ratings yet
- The Dandenong Dossier 2010Document243 pagesThe Dandenong Dossier 2010reshminNo ratings yet
- Metkus Et Al 2023 Presentation and Outcomes of Patients With Preoperative Critical Illness Undergoing Cardiac SurgeryDocument8 pagesMetkus Et Al 2023 Presentation and Outcomes of Patients With Preoperative Critical Illness Undergoing Cardiac Surgerytegar ksatriaNo ratings yet
- Kelompok 2 - CICU - LITREV - PENANGANAN ARRHYTHMOGENIC RIGHT VENTRICULARDocument14 pagesKelompok 2 - CICU - LITREV - PENANGANAN ARRHYTHMOGENIC RIGHT VENTRICULARasep idoyNo ratings yet
- Cardiac Stress TestingDocument90 pagesCardiac Stress TestingFrancesca Isabel BunyiNo ratings yet
- Nephrotic Syndrome (Nephrosis)Document9 pagesNephrotic Syndrome (Nephrosis)Radit Radovzky MayangkaraNo ratings yet
- 28-Article Text-165-1-10-20200818Document11 pages28-Article Text-165-1-10-20200818Edriyan SyaputraNo ratings yet
- MTI Interview - FAQs For Candidates - Final - 0Document9 pagesMTI Interview - FAQs For Candidates - Final - 0MariajanNo ratings yet
- Advanced Cardiac Life Support (ACLS) : Dr. Martha Regisna Silalahi RSUD BintanDocument19 pagesAdvanced Cardiac Life Support (ACLS) : Dr. Martha Regisna Silalahi RSUD BintangisnamarthaNo ratings yet
- Journal Heptojugular RefluxDocument5 pagesJournal Heptojugular RefluxFarhan RezaNo ratings yet
- Nephrology Curriculum - الزمالة المصرية للكليDocument60 pagesNephrology Curriculum - الزمالة المصرية للكليbook1man100% (1)
- Activity 11 Cardiac Tamponade NCPDocument3 pagesActivity 11 Cardiac Tamponade NCPCloe CorpuzNo ratings yet
- 53 Coronary Artery AnomaliesDocument5 pages53 Coronary Artery AnomaliesVictor PazNo ratings yet
- Heart Diseases in PregnancyDocument19 pagesHeart Diseases in PregnancyKirubah Sai PatnaikNo ratings yet
- Cardiology - Corrected AhmedDocument23 pagesCardiology - Corrected AhmedHanadi UmhanayNo ratings yet
- Electrical Diseases of The Heart PDFDocument982 pagesElectrical Diseases of The Heart PDFJavierPiñeiroAndradeNo ratings yet
- Claria Mri QQDocument60 pagesClaria Mri QQbobo samNo ratings yet
- Left Sided Heart FailureDocument25 pagesLeft Sided Heart FailurePaulNo ratings yet