Download as pdf or txt
You might also like
- ASTA Membership Directory 2022Document18 pagesASTA Membership Directory 2022Vasanthi Muthayan100% (1)
- Written Quiz SITHCCC006Document15 pagesWritten Quiz SITHCCC006ajay67% (3)
- Expression of Interest - Elective Placement For Medical StudentsDocument2 pagesExpression of Interest - Elective Placement For Medical Studentsfsdfs100% (1)
- Intrapartum 111: 1. Examine The Woman For Emergency SignsDocument7 pagesIntrapartum 111: 1. Examine The Woman For Emergency SignsJane MartinNo ratings yet
- Management of Normal LaborDocument10 pagesManagement of Normal Labortsegay169No ratings yet
- Fetal Well BeingDocument5 pagesFetal Well BeingCARL JOHN MANALONo ratings yet
- Stages of Labor Nursing Intervention: First StageDocument3 pagesStages of Labor Nursing Intervention: First StageJhanniel IreneaNo ratings yet
- First Stage of LabourDocument22 pagesFirst Stage of LabourdodoNo ratings yet
- Essential Intrapartum and Newborn CareDocument23 pagesEssential Intrapartum and Newborn CareEarl ReyesNo ratings yet
- Handout Steps To Follow in INTRAPARTAL CAREDocument13 pagesHandout Steps To Follow in INTRAPARTAL CAREalyssa marie salcedoNo ratings yet
- Explain 4Document21 pagesExplain 4CHACHACHACHAAAAANo ratings yet
- 15 EmOC Labour & P'gram 2016 FINALDocument45 pages15 EmOC Labour & P'gram 2016 FINALDavina DakapNo ratings yet
- Low Risk Labour CareDocument11 pagesLow Risk Labour CareYwagar YwagarNo ratings yet
- NFDN 2004 - Unit 4.3 - JLB StudentDocument43 pagesNFDN 2004 - Unit 4.3 - JLB StudentkendrabooboooNo ratings yet
- Post-Term Labor - NCPDocument8 pagesPost-Term Labor - NCPCameron De GuzmanNo ratings yet
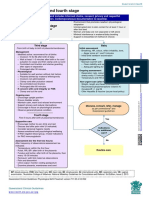
- F NB ThirdfourthstageDocument1 pageF NB ThirdfourthstageManisha ThakurNo ratings yet
- Labor & DeliveryDocument9 pagesLabor & DeliveryfriaslenemoNo ratings yet
- Chapter 14Document5 pagesChapter 14Kelly HeartsillNo ratings yet
- Cmca Trans AntenatalDocument4 pagesCmca Trans Antenatal2xy79knkmyNo ratings yet
- A Multidisciplinary Care Map For A Woman in Preterm Labor LazaletaDocument3 pagesA Multidisciplinary Care Map For A Woman in Preterm Labor Lazaletablythe RiveroNo ratings yet
- Preterm Labor: Group 6Document13 pagesPreterm Labor: Group 6Evelyn MedinaNo ratings yet
- Care of Mother, Child, and Adolescent NCM 107Document24 pagesCare of Mother, Child, and Adolescent NCM 107Gizzi Asbelle EspirituNo ratings yet
- Care During First Stage of LabourDocument6 pagesCare During First Stage of LabourSabita PaudelNo ratings yet
- Antepartum AssessmentDocument14 pagesAntepartum Assessmentamena mahmoudNo ratings yet
- Normal Labour: PRESENTED BY DR Tsitsi Vimbayi ChatoraDocument13 pagesNormal Labour: PRESENTED BY DR Tsitsi Vimbayi ChatoraChatora Tsitsi VimbayiNo ratings yet
- Poster 17Document2 pagesPoster 17Abhi DasNo ratings yet
- Antenatal Care AduanaDocument36 pagesAntenatal Care AduanalaarnieNo ratings yet
- Stages of LabourDocument43 pagesStages of LabourhaisureshNo ratings yet
- Learn Mat 6Document14 pagesLearn Mat 6Shyla ManguiatNo ratings yet
- Nursing Management of During Stages of Labor and Delivery UpdatedDocument60 pagesNursing Management of During Stages of Labor and Delivery UpdatedSherlyn Miranda GarcesNo ratings yet
- DR NotesDocument6 pagesDR NotesMina ByunNo ratings yet
- Problem With The PowersDocument9 pagesProblem With The PowersNicole Claire LegaspiNo ratings yet
- Labor Delivery 1Document29 pagesLabor Delivery 1Elmer DaquilañeaNo ratings yet
- Process Flow of Clinical Service Antenatal Care: Information AreaDocument4 pagesProcess Flow of Clinical Service Antenatal Care: Information ArearonronNo ratings yet
- Normal Spontaneous Vaginal DeliveryDocument6 pagesNormal Spontaneous Vaginal DeliveryQuennie AlamNo ratings yet
- Chapter 9 (Assessing The Fetal Well-Being) : The Care of Mother, Child and AdolescenceDocument22 pagesChapter 9 (Assessing The Fetal Well-Being) : The Care of Mother, Child and AdolescenceMARIA PEARLITA TANNo ratings yet
- EINC Handout by Nicole Honrado BSN 2ADocument7 pagesEINC Handout by Nicole Honrado BSN 2A2A - Nicole Marrie HonradoNo ratings yet
- Intrapartum Complication: N420 Childbearing Family Nursing Week 13 April 13, 2000Document37 pagesIntrapartum Complication: N420 Childbearing Family Nursing Week 13 April 13, 2000Mikylla Huertas0% (1)
- JINGCO - BSN 2-D - Module-6-Storified-Case-ScenarioDocument13 pagesJINGCO - BSN 2-D - Module-6-Storified-Case-ScenarioJashtine JingcoNo ratings yet
- Labour - 1st Stage - ManagementDocument29 pagesLabour - 1st Stage - ManagementJeevitha .BNo ratings yet
- Labour Second StageDocument8 pagesLabour Second StageakankshaNo ratings yet
- C SectionDocument8 pagesC SectionJenny Agustin FabrosNo ratings yet
- Care During Labor and Delivery: SBA - Presentation 4Document29 pagesCare During Labor and Delivery: SBA - Presentation 4HemamaliniNo ratings yet
- Book Reading 2 REF SalinanDocument40 pagesBook Reading 2 REF SalinanNahrisyah Ulfa SafnaNo ratings yet
- Dysfunctional Labor DystociaDocument8 pagesDysfunctional Labor Dystociamardsz100% (2)
- POST PARTUM CARE 5thDocument25 pagesPOST PARTUM CARE 5thAnthony Joseph ReyesNo ratings yet
- Labor Part 2: Maternal and Child Health - Trina Domanais - BSN 2P Iii. Power A. Uterine Contraction First Stage of LaborDocument3 pagesLabor Part 2: Maternal and Child Health - Trina Domanais - BSN 2P Iii. Power A. Uterine Contraction First Stage of LaborRANDY ERNEST GESTOSANINo ratings yet
- Nursing Management During Stages of Labor and Delivery UpdatedDocument40 pagesNursing Management During Stages of Labor and Delivery UpdatedCharlmagne LinnamNo ratings yet
- Fetal AssessmentDocument28 pagesFetal Assessmentgayon09No ratings yet
- Antepartum SurveilDocument3 pagesAntepartum Surveilapi-3712326No ratings yet
- Emergency Cases (Document (A4 Portrait) )Document14 pagesEmergency Cases (Document (A4 Portrait) )Joelyn DulayNo ratings yet
- Case Study AnswersDocument4 pagesCase Study AnswersGenevieve VillaflorNo ratings yet
- Labour Presentation ObsDocument48 pagesLabour Presentation ObsVera BannorNo ratings yet
- #15 - NCM 109 (Rle) - TransesDocument9 pages#15 - NCM 109 (Rle) - TransesJaimie BanaagNo ratings yet
- EINCDocument69 pagesEINCNicole GadrinabNo ratings yet
- 6 ExamDocument9 pages6 Examjacynda linsanganNo ratings yet
- Labour and Delivery: Dr. Amani ShamanDocument56 pagesLabour and Delivery: Dr. Amani ShamanKholoud KholoudNo ratings yet
- Management of First Stage of Labour: Prepared By: Nirsuba Gurung Assistant Lecturer MsonDocument55 pagesManagement of First Stage of Labour: Prepared By: Nirsuba Gurung Assistant Lecturer MsonBharat ThapaNo ratings yet
- CH 10 Test 3 NotesDocument10 pagesCH 10 Test 3 NotesJulx0No ratings yet
- Pre-Clinical Assignment: Labor and Delivery Management PlanDocument7 pagesPre-Clinical Assignment: Labor and Delivery Management PlanSaharish HoodaNo ratings yet
- Nursing Care During Labor and BirthDocument7 pagesNursing Care During Labor and BirthRegine VillanuevaNo ratings yet
- CertificationDocument35 pagesCertificationRobin ThingomNo ratings yet
- Module 2Document40 pagesModule 2Romel CuregNo ratings yet
- Rev Implementasi UC Poli GigiDocument150 pagesRev Implementasi UC Poli GiginikeNo ratings yet
- Technical Data Sheet: Tire Lube and SealDocument1 pageTechnical Data Sheet: Tire Lube and SealDon HowardNo ratings yet
- (Download PDF) The Monstrous Feminine in Contemporary Japanese Popular Culture Raechel Dumas Online Ebook All Chapter PDFDocument42 pages(Download PDF) The Monstrous Feminine in Contemporary Japanese Popular Culture Raechel Dumas Online Ebook All Chapter PDFdavid.messer693100% (15)
- Rock Mechanics Fundamentals: Foot) - What Is Its Specific Gravity?Document18 pagesRock Mechanics Fundamentals: Foot) - What Is Its Specific Gravity?Ghulam Mohyuddin SohailNo ratings yet
- TM 9-1783a A-C HD-7W Diesel EngineDocument173 pagesTM 9-1783a A-C HD-7W Diesel EngineAdvocate100% (1)
- Aiaa 2003 0696 PDFDocument11 pagesAiaa 2003 0696 PDFSyed Ñąveed HąįdeŕNo ratings yet
- Japanese Industrial StandardsDocument10 pagesJapanese Industrial StandardsKen SelorioNo ratings yet
- Aluminium GMAW GuideDocument32 pagesAluminium GMAW GuideDaniel Salinas100% (2)
- Moonbase Blues BW v1Document2 pagesMoonbase Blues BW v1Станіслав Польськой100% (3)
- Technical Specification 1 No: Unit QtyDocument3 pagesTechnical Specification 1 No: Unit QtySuraj KhopeNo ratings yet
- ĐỀ 51Document9 pagesĐỀ 51bichngocvonagiNo ratings yet
- Drying Bed Design PDFDocument29 pagesDrying Bed Design PDFAshokNo ratings yet
- Homemade Parallettes: What Is A Parallette?Document58 pagesHomemade Parallettes: What Is A Parallette?Athos VianaNo ratings yet
- 12 Production and Purification of Recombinant Glargine Insulin From Escherichia Coli BL-21 StrainDocument12 pages12 Production and Purification of Recombinant Glargine Insulin From Escherichia Coli BL-21 StrainAnand KumarNo ratings yet
- Sunlight Dishwashing Liquid-All-updated 09 PDFDocument4 pagesSunlight Dishwashing Liquid-All-updated 09 PDFcontrax8No ratings yet
- Code On Wages 2019 - NotesDocument3 pagesCode On Wages 2019 - NotesAnand ReddyNo ratings yet
- RPZ Testing Form 215bDocument2 pagesRPZ Testing Form 215bSam ChoiNo ratings yet
- SFDA Requirement For DEXADocument9 pagesSFDA Requirement For DEXAEhsan alwafaaNo ratings yet
- CASE STUDY CAKE BATIK Proximate AnalysisDocument25 pagesCASE STUDY CAKE BATIK Proximate AnalysisNur Azhani100% (1)
- Dettol Liquid Hand Wash SDSDocument10 pagesDettol Liquid Hand Wash SDSaskdfhaosljudgnNo ratings yet
- H. P. Lovecraft - PolarisDocument3 pagesH. P. Lovecraft - PolarisBárbara AlvesNo ratings yet
- Apr 78Document147 pagesApr 78Quality AssuranceNo ratings yet
- What Would You Be If You Were?Document2 pagesWhat Would You Be If You Were?oantaNo ratings yet
- Tugas English Afwa Jurnal 1910811011 GanjilDocument4 pagesTugas English Afwa Jurnal 1910811011 Ganjilsakna afwaNo ratings yet
- Unit IG2: Risk AssessmentDocument16 pagesUnit IG2: Risk AssessmentRizwan Hameed100% (2)