Download as pdf or txt
You might also like
- QBANK PasTest SAQs For DentistryDocument651 pagesQBANK PasTest SAQs For DentistrybassamNo ratings yet
- 1949 Neff TAILORED OCCLUSION WITH THE ANTERIOR COEFFICIDocument5 pages1949 Neff TAILORED OCCLUSION WITH THE ANTERIOR COEFFICIRockey ShrivastavaNo ratings yet
- Clase II Extraccion o NoDocument17 pagesClase II Extraccion o NoDiego PinedaNo ratings yet
- The Profile Analysis of A.M. SchwarzDocument5 pagesThe Profile Analysis of A.M. SchwarzMariyam100% (4)
- Openbite CamouflageDocument8 pagesOpenbite CamouflageRakesh RaveendranNo ratings yet
- Maxillary Arch Distalization Using Interradicular Miniscrews and The Lever-Arm ApplianceDocument8 pagesMaxillary Arch Distalization Using Interradicular Miniscrews and The Lever-Arm ApplianceJuan Carlos CárcamoNo ratings yet
- Jioh 7 65Document3 pagesJioh 7 65Athira JithendranathNo ratings yet
- Jurnal 3Document5 pagesJurnal 3Ef AzhariNo ratings yet
- Nonsurgical Correction of A Class III Malocclusion in An Adult by Miniscrew-Assisted Mandibular Dentition DistalizationDocument11 pagesNonsurgical Correction of A Class III Malocclusion in An Adult by Miniscrew-Assisted Mandibular Dentition DistalizationNeycer Catpo NuncevayNo ratings yet
- Bong 2011 PDFDocument14 pagesBong 2011 PDFkarenchavezalvanNo ratings yet
- Severe Anterior Open Bite With Mandibular Retrusion Treated With Multiloop Edgewise Archwires and Microimplant Anchorage ComplementedDocument10 pagesSevere Anterior Open Bite With Mandibular Retrusion Treated With Multiloop Edgewise Archwires and Microimplant Anchorage ComplementedLedir Luciana Henley de AndradeNo ratings yet
- TRATRAMIENTO DE CLASE II DIVISION 2 CON ExTREMA PROFUNDIDADDocument13 pagesTRATRAMIENTO DE CLASE II DIVISION 2 CON ExTREMA PROFUNDIDADMelisa GuerraNo ratings yet
- Twin-Occlusion Prosthesis in A Class IIIDocument47 pagesTwin-Occlusion Prosthesis in A Class IIINishu PriyaNo ratings yet
- Correction of Sever Rotation of Central Maxillary Incisor With Fixed-Removable Appliance in The Mixed Dentition Stage: A Case ReportDocument5 pagesCorrection of Sever Rotation of Central Maxillary Incisor With Fixed-Removable Appliance in The Mixed Dentition Stage: A Case ReportJavier Farias VeraNo ratings yet
- 1 s2.0 S2666430522000036 MainDocument12 pages1 s2.0 S2666430522000036 MainDANTE DELEGUERYNo ratings yet
- AJO DO Revista ArticuloDocument10 pagesAJO DO Revista ArticuloAngélicaLujánNo ratings yet
- Open Bite: Diagnosis, Treatment and StabilityDocument12 pagesOpen Bite: Diagnosis, Treatment and Stabilityjavi222222No ratings yet
- Case Report Lateral Open Bite Treatment Stability OMT Essential Cabrera USP Brazil AJO DO 2011Document11 pagesCase Report Lateral Open Bite Treatment Stability OMT Essential Cabrera USP Brazil AJO DO 2011AndreaVanoyMartinNo ratings yet
- Open Bite: Diagnosis, Treatment and StabilityDocument11 pagesOpen Bite: Diagnosis, Treatment and StabilityJavier Farias VeraNo ratings yet
- Sefalo 3Document6 pagesSefalo 3Aisha DewiNo ratings yet
- Rehabilitation of Hemimandibulectomy PatientDocument3 pagesRehabilitation of Hemimandibulectomy PatientAB MISHRANo ratings yet
- Multiloop PDFDocument10 pagesMultiloop PDFAstrid Carolina HerreraNo ratings yet
- JOrthodRes3157-5423691 150356 PDFDocument4 pagesJOrthodRes3157-5423691 150356 PDFCatarina RochaNo ratings yet
- Chin Remodeling in A Patient With Bimaxillary P 2018 American Journal of OrtDocument9 pagesChin Remodeling in A Patient With Bimaxillary P 2018 American Journal of Ortchristian roblesNo ratings yet
- Severe Class II Division 1 MalocclusionDocument14 pagesSevere Class II Division 1 MalocclusionCARMEN ROSA AREVALO ROLDANNo ratings yet
- OrthoDocument3 pagesOrthohegarNo ratings yet
- Journal of The World Federation of OrthodontistsDocument8 pagesJournal of The World Federation of OrthodontistsJuan Carlos MeloNo ratings yet
- Artículo DentalDocument6 pagesArtículo DentalAngélicaLujánNo ratings yet
- Artículo OrtodonciaDocument5 pagesArtículo OrtodonciaReyalejandro's huntingNo ratings yet
- Ojsadmin, 388Document10 pagesOjsadmin, 388Srishti Jain MalooNo ratings yet
- Multiloop Edgewise Archwire in The Treatment of A Patient With An Anterior Open Bite and A Long FaceDocument7 pagesMultiloop Edgewise Archwire in The Treatment of A Patient With An Anterior Open Bite and A Long FaceKanchit SuwanswadNo ratings yet
- 10.0000@Www - Jco Online - Com@1999@04@236 The 018 Nickel Titanium Stop For Prevention of Archwire CrawlDocument5 pages10.0000@Www - Jco Online - Com@1999@04@236 The 018 Nickel Titanium Stop For Prevention of Archwire Crawlhassankhan9849No ratings yet
- Journal of The World Federation of OrthodontistsDocument6 pagesJournal of The World Federation of OrthodontistsJuan Carlos MeloNo ratings yet
- Ajodo Clase II-2 2018Document9 pagesAjodo Clase II-2 2018Luis HerreraNo ratings yet
- Dramit007, Journal Manager, 13Document3 pagesDramit007, Journal Manager, 13KAREN VIVIANA ALVARADO HERNANDEZNo ratings yet
- Class I Malocclusion Article JD-4Document8 pagesClass I Malocclusion Article JD-4panimalar madhaNo ratings yet
- Jurnal Ortho 6Document5 pagesJurnal Ortho 6Santika IndahsariNo ratings yet
- Awais AssignmentDocument3 pagesAwais AssignmentMuhammad AwaisNo ratings yet
- Orthodontic Treatment of A Patient With Bilateral Congenitally Missing Maxillary Canines: The Effects of First Premolar Substitution On The Functional OutcomeDocument6 pagesOrthodontic Treatment of A Patient With Bilateral Congenitally Missing Maxillary Canines: The Effects of First Premolar Substitution On The Functional OutcomesauriuaNo ratings yet
- Mandibular Premolar Transplantation To Replace Missing Maxillary Anterior Teeth: A Multidisciplinary ApproachDocument14 pagesMandibular Premolar Transplantation To Replace Missing Maxillary Anterior Teeth: A Multidisciplinary ApproachRicha AhlawatNo ratings yet
- Pendulum Appliance in Two Phases OrthodoDocument6 pagesPendulum Appliance in Two Phases OrthodoAndra Andra ENo ratings yet
- Disatalización Clase IIDocument13 pagesDisatalización Clase IIchristian roblesNo ratings yet
- Edgewise in cl2Document4 pagesEdgewise in cl2MariaBoicuNo ratings yet
- Arvystas 1998Document4 pagesArvystas 1998Саша АптреевNo ratings yet
- Class III Malocclusion SurgicaDocument9 pagesClass III Malocclusion Surgicaortodoncia 2022No ratings yet
- Non Extraction Orthodontic Management of Class I Malocclusion With Ectopically Placed Canine: A CaseDocument4 pagesNon Extraction Orthodontic Management of Class I Malocclusion With Ectopically Placed Canine: A CaseDr ZarniNo ratings yet
- Gummy Smile Case ReportDocument13 pagesGummy Smile Case ReportAli ChaconNo ratings yet
- Vertical-Dimension Control During En-MasseDocument13 pagesVertical-Dimension Control During En-MasseLisbethNo ratings yet
- TwinblockpaperDocument6 pagesTwinblockpaperelvin peraltaNo ratings yet
- Atypical Extraction Treatment For Failing Replante - 2020 - American Journal ofDocument11 pagesAtypical Extraction Treatment For Failing Replante - 2020 - American Journal ofAlejandro Aranzábal NavarreteNo ratings yet
- AJODO-mechanism-case ReportDocument10 pagesAJODO-mechanism-case ReportAthira JithendranathNo ratings yet
- Journal of The World Federation of OrthodontistsDocument7 pagesJournal of The World Federation of OrthodontistsCastillon SamNo ratings yet
- Management Class Ii Division 1 Malocclusion: Prepared byDocument41 pagesManagement Class Ii Division 1 Malocclusion: Prepared byNur AwanisNo ratings yet
- Jurnal OrthoDocument5 pagesJurnal OrthoBatman KANo ratings yet
- Two-Stage Treatment of Skeletal Class III Malocclusion During The Early Permanent DentitionDocument8 pagesTwo-Stage Treatment of Skeletal Class III Malocclusion During The Early Permanent DentitionkarenchavezalvanNo ratings yet
- Maxillary Molar Distalization With Modified Trans Palatal Arch and Mini Implants PDFDocument6 pagesMaxillary Molar Distalization With Modified Trans Palatal Arch and Mini Implants PDFSoe San KyawNo ratings yet
- A Pair For The Impaired - Orthodontic and Surgical Combination Treatment of Skeletal Class III Malocclusion: A Two Year Follow UpDocument9 pagesA Pair For The Impaired - Orthodontic and Surgical Combination Treatment of Skeletal Class III Malocclusion: A Two Year Follow UprohitNo ratings yet
- AlineadoresDocument5 pagesAlineadoresAlfredo RamzNo ratings yet
- Management of A Palatal Gingival Groove in A Maxillary Lateral Incisor: A Case ReportDocument4 pagesManagement of A Palatal Gingival Groove in A Maxillary Lateral Incisor: A Case ReporthappykglayNo ratings yet
- Rescue Therapy With Orthodontic Traction To Manage Severely Impacted Mandibular Second Molars and To Restore An Alveolar Bone DefectDocument12 pagesRescue Therapy With Orthodontic Traction To Manage Severely Impacted Mandibular Second Molars and To Restore An Alveolar Bone DefectNathália LopesNo ratings yet
- Endodontic Treatment of Mandibular Premolars With Complex Anatomy Case SeriesDocument5 pagesEndodontic Treatment of Mandibular Premolars With Complex Anatomy Case SeriesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Controlled Tooth Movement To Correct An Iatrogenic Problem: Case ReportDocument8 pagesControlled Tooth Movement To Correct An Iatrogenic Problem: Case ReportElla GolikNo ratings yet
- Implant Therapy: Clinical Approaches and Evidence of Success, Second EditionFrom EverandImplant Therapy: Clinical Approaches and Evidence of Success, Second EditionNo ratings yet
- Epiphora Drainage by DCR - Long-Term Results: Original ResearchDocument5 pagesEpiphora Drainage by DCR - Long-Term Results: Original ResearchSaatvik AtriNo ratings yet
- Accuracy of Demirjian's and Indian Specific Formulae in Age Estimation Using Eight-Teeth Method in Kanyakumari PopulationDocument6 pagesAccuracy of Demirjian's and Indian Specific Formulae in Age Estimation Using Eight-Teeth Method in Kanyakumari PopulationSaatvik AtriNo ratings yet
- Determination of Fluoride Release and Strength of A Fluoride Treated Heat Cured Acrylic ResinDocument5 pagesDetermination of Fluoride Release and Strength of A Fluoride Treated Heat Cured Acrylic ResinSaatvik AtriNo ratings yet
- IndianJDentRes303332-306504 083050Document5 pagesIndianJDentRes303332-306504 083050Saatvik AtriNo ratings yet
- East Java Extract Propolis As Potential Intracanal Medicament in Experimentally Induced Chronic Apical PeriodontitisDocument5 pagesEast Java Extract Propolis As Potential Intracanal Medicament in Experimentally Induced Chronic Apical PeriodontitisSaatvik AtriNo ratings yet
- Oral Microbes and NCDS: EditorialDocument1 pageOral Microbes and NCDS: EditorialSaatvik AtriNo ratings yet
- IDJ Vol 7 1Document6 pagesIDJ Vol 7 1Saatvik AtriNo ratings yet
- Esthetic Depigmentation of Anterior Gingiva: A Case: Indian Dental JournalDocument3 pagesEsthetic Depigmentation of Anterior Gingiva: A Case: Indian Dental JournalSaatvik AtriNo ratings yet
- Indian Dental Journal: Zirconia As An Implant BiomaterialDocument6 pagesIndian Dental Journal: Zirconia As An Implant BiomaterialSaatvik AtriNo ratings yet
- IndianJDentRes303329-3001241 082012Document2 pagesIndianJDentRes303329-3001241 082012Saatvik AtriNo ratings yet
- IDJ Vol 5 2 PDFDocument6 pagesIDJ Vol 5 2 PDFSaatvik AtriNo ratings yet
- Oral Health Behaviour of Children and Adults in Urban and Rural Areas of Burkina Faso, AfricaDocument10 pagesOral Health Behaviour of Children and Adults in Urban and Rural Areas of Burkina Faso, AfricaSaatvik AtriNo ratings yet
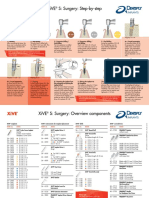
- XiVE Surgery Step-By-stepDocument2 pagesXiVE Surgery Step-By-stepSaatvik AtriNo ratings yet
- Operation Manual: Surgic ProDocument24 pagesOperation Manual: Surgic ProSaatvik AtriNo ratings yet
- Familial Infantile Osteopetrosis: A Case Report: Indian Dental JournalDocument6 pagesFamilial Infantile Osteopetrosis: A Case Report: Indian Dental JournalSaatvik AtriNo ratings yet
- Surface Modifications For Dental ImplantsDocument5 pagesSurface Modifications For Dental ImplantsSaatvik AtriNo ratings yet
- Age Estimation Methods in Forensic Odontology: Indian Dental JournalDocument5 pagesAge Estimation Methods in Forensic Odontology: Indian Dental JournalSaatvik AtriNo ratings yet
- IDJ Vol 5 3 PDFDocument5 pagesIDJ Vol 5 3 PDFSaatvik AtriNo ratings yet
- Inter Occlusal Record Materials Used For Patients Under Going Prosthodontic RehabilitationDocument6 pagesInter Occlusal Record Materials Used For Patients Under Going Prosthodontic RehabilitationSaatvik AtriNo ratings yet
- Relationship Between Gutkha Chewing People and Their Saliva Composition Including Bacterial MicrofloraDocument3 pagesRelationship Between Gutkha Chewing People and Their Saliva Composition Including Bacterial MicrofloraSaatvik AtriNo ratings yet
- Indian Dental Journal: Endodontic Irrigation: An UpdateDocument6 pagesIndian Dental Journal: Endodontic Irrigation: An UpdateSaatvik AtriNo ratings yet
- 1801cei PaceImpressions WebDocument7 pages1801cei PaceImpressions WebSaatvik AtriNo ratings yet
- IDJ Vol 4 7Document5 pagesIDJ Vol 4 7Saatvik AtriNo ratings yet
- Indian Dental Journal: Nutrition and Prosthodontic PatientDocument2 pagesIndian Dental Journal: Nutrition and Prosthodontic PatientSaatvik AtriNo ratings yet
- IDJ Vol 4 7 PDFDocument5 pagesIDJ Vol 4 7 PDFSaatvik AtriNo ratings yet
- Age Estimation Methods in Forensic Odontology: Indian Dental JournalDocument5 pagesAge Estimation Methods in Forensic Odontology: Indian Dental JournalSaatvik AtriNo ratings yet
- Rehabilitation of Edentulous Maxillectomy Patient With Lightweight, Top Open Obturator: A Clinical ReportDocument3 pagesRehabilitation of Edentulous Maxillectomy Patient With Lightweight, Top Open Obturator: A Clinical ReportSaatvik AtriNo ratings yet
- 3580/PDF/1807cei Boynes WebDocument12 pages3580/PDF/1807cei Boynes WebSaatvik AtriNo ratings yet
- IDJ Vol 4 6Document6 pagesIDJ Vol 4 6Saatvik AtriNo ratings yet
- Jop.2008.080086.lowlink - PDF v03 PDFDocument14 pagesJop.2008.080086.lowlink - PDF v03 PDFSaatvik AtriNo ratings yet
- FacemaskDocument30 pagesFacemaskAnushree RathiNo ratings yet
- Occlusal Schemes and How To Achieve ThemDocument3 pagesOcclusal Schemes and How To Achieve ThemCostin SilviuNo ratings yet
- Herbst Appliance: Dr. Rajshekhar BanerjeeDocument161 pagesHerbst Appliance: Dr. Rajshekhar BanerjeeRajshekhar Banerjee100% (3)
- Class III Twin Blocks: A Case Series: Clinical SectionDocument6 pagesClass III Twin Blocks: A Case Series: Clinical Sectionortodoncia 2018No ratings yet
- Treatment of Brodie SyndromeDocument25 pagesTreatment of Brodie SyndromeAdina Serban100% (1)
- Cherry Loop - A New Loop To Move Mandibular Molar MesialyDocument6 pagesCherry Loop - A New Loop To Move Mandibular Molar MesialyCristian CarlosNo ratings yet
- Case 2Document18 pagesCase 2atikaNo ratings yet
- Quiz Pharma and OrthoDocument5 pagesQuiz Pharma and OrthoMonaNo ratings yet
- Reliability and Validity of T-Scan and 3D Intraoral Scanning For Measuring The Occlusal Contact AreaDocument7 pagesReliability and Validity of T-Scan and 3D Intraoral Scanning For Measuring The Occlusal Contact AreaananthNo ratings yet
- Prediction in An Ortho Surgical Case: A ReportDocument7 pagesPrediction in An Ortho Surgical Case: A ReportMuhammad AleemNo ratings yet
- Implant OcclusionDocument43 pagesImplant OcclusionMuaiyed Buzayan Akremy100% (3)
- Via Zis 1991Document2 pagesVia Zis 1991drvivek reddyNo ratings yet
- Mascara Facial 2Document7 pagesMascara Facial 2afperdomo8403No ratings yet
- MEAW-Kim Jeong Il Đã ConvertDocument659 pagesMEAW-Kim Jeong Il Đã ConvertNguyen Hong AnNo ratings yet
- ClearCorrect Case Examples BookletDocument64 pagesClearCorrect Case Examples BookletkirthikakumarNo ratings yet
- Classification of Malocclusion Jai - Pptsaurabh / Orthodontic Courses by Indian Dental AcademyDocument136 pagesClassification of Malocclusion Jai - Pptsaurabh / Orthodontic Courses by Indian Dental Academyindian dental academy100% (2)
- Class II MEAWDocument27 pagesClass II MEAWNhock LamentosNo ratings yet
- Effects On The Periodontium Following Corticotomy Facilitated Orthodontics. Case ReportsDocument5 pagesEffects On The Periodontium Following Corticotomy Facilitated Orthodontics. Case Reportschristian roblesNo ratings yet
- Unusual Orthodontic Correction of Bilateral Maxillary Canine-First Premolar TranspositionDocument11 pagesUnusual Orthodontic Correction of Bilateral Maxillary Canine-First Premolar TranspositionAstrid DindaNo ratings yet
- 7orthodoenticsvol6issue1pp23-26 20190307020613Document4 pages7orthodoenticsvol6issue1pp23-26 20190307020613Diba Eka DiputriNo ratings yet
- 2010niko Christian BockDocument6 pages2010niko Christian BockNeeraj AroraNo ratings yet
- Modified Beggs / Orthodontic Courses by Indian Dental AcademyDocument202 pagesModified Beggs / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- PAR Scoring Sheet - 2017Document1 pagePAR Scoring Sheet - 2017Assem AbdejawwadNo ratings yet
- Class II Correction....Document7 pagesClass II Correction....Yudia PangestiNo ratings yet
- T-Loop Force System With and Without Vertical Step Using Finite Element AnalysisDocument8 pagesT-Loop Force System With and Without Vertical Step Using Finite Element AnalysisHabeeb AL-AbsiNo ratings yet
- Introduction, Definition, Need For Orthodontic Care and Aims &objectives of Orthodontics Bds 3 YearDocument28 pagesIntroduction, Definition, Need For Orthodontic Care and Aims &objectives of Orthodontics Bds 3 YearJude Daniel AquinoNo ratings yet
- Pedo QuestionsDocument11 pagesPedo QuestionsSaleh Al-naimi83% (6)