Download as pdf or txt
You might also like
- PDF Bobcat s175 s185 Service Repair Manual SN 525011001 525111001 525211001 525311001 and AboveDocument933 pagesPDF Bobcat s175 s185 Service Repair Manual SN 525011001 525111001 525211001 525311001 and AboveChristian Cepeda86% (7)
- Lung AnatomyDocument19 pagesLung AnatomyScott Yee100% (2)
- Journal MataDocument6 pagesJournal MataRyad TabraniNo ratings yet
- Dietary Carotenoids, Vitamins C and E, and Risk of Cataract in WomenDocument8 pagesDietary Carotenoids, Vitamins C and E, and Risk of Cataract in WomenDiah RahmawatiNo ratings yet
- Clinical - Alimentary TractDocument8 pagesClinical - Alimentary TractFernando SousaNo ratings yet
- Evidence Supports Nutritional Support: EditorialDocument3 pagesEvidence Supports Nutritional Support: EditorialVitoria SilvaNo ratings yet
- Malnutrition in Older Adults: Screening and DeterminantsDocument8 pagesMalnutrition in Older Adults: Screening and DeterminantsDaniela Aguilar SánchezNo ratings yet
- JurnalDocument9 pagesJurnalSidika YuniaNo ratings yet
- SGNA NinosDocument7 pagesSGNA NinosjorgeNo ratings yet
- Risk Factors For Glaucoma Needing More Attention: Anne L. Coleman and Gergana KodjebachevaDocument5 pagesRisk Factors For Glaucoma Needing More Attention: Anne L. Coleman and Gergana KodjebachevaAngkat Prasetya Abdi NegaraNo ratings yet
- Nutrients 12 00878Document13 pagesNutrients 12 00878Ardian AshadiNo ratings yet
- Practiceguidelines: Received: 4 May 2017 Accepted: 22 May 2017 DOI: 10.1002/hed.24866Document7 pagesPracticeguidelines: Received: 4 May 2017 Accepted: 22 May 2017 DOI: 10.1002/hed.24866MdacNo ratings yet
- Prospective Study of Major Dietary Patterns and Risk of CoronaryDocument10 pagesProspective Study of Major Dietary Patterns and Risk of CoronaryJohn SammutNo ratings yet
- 2011 Corrigan - Nutrition in Stroke PatientsDocument11 pages2011 Corrigan - Nutrition in Stroke PatientsAmy100% (1)
- 13 SureDocument11 pages13 SureSamuel Kyei-BoatengNo ratings yet
- 1 s2.0 S2405457723001237 MainDocument7 pages1 s2.0 S2405457723001237 MainAfi FaturNo ratings yet
- Does Cow S Milk Protein Elimination Diet Have A Role On Induction and MaintenanceDocument6 pagesDoes Cow S Milk Protein Elimination Diet Have A Role On Induction and MaintenanceNejc KovačNo ratings yet
- Celiac DiseaseDocument19 pagesCeliac Disease35432No ratings yet
- Late Eating Is Associated With Cardiometabolic Risk Traits, Obesogenic Behaviors, and Impaired Weight LossDocument8 pagesLate Eating Is Associated With Cardiometabolic Risk Traits, Obesogenic Behaviors, and Impaired Weight LossSukma DewiNo ratings yet
- Commentary: Nutritional Assessment and Length of Hospital StayDocument2 pagesCommentary: Nutritional Assessment and Length of Hospital StayNjeodoNo ratings yet
- Temporal Eating Patterns: Associations With Nutrient Intakes, Diet Quality, and Measures of AdiposityDocument10 pagesTemporal Eating Patterns: Associations With Nutrient Intakes, Diet Quality, and Measures of Adipositywilly yashilvaNo ratings yet
- Nutrients 11 02123Document4 pagesNutrients 11 02123Pamela MierNo ratings yet
- Am J Clin Nutr 2015 Paddon Jones 1339S 45SDocument7 pagesAm J Clin Nutr 2015 Paddon Jones 1339S 45SevaNo ratings yet
- Subjective Global Nutrition Assessment ChildrenDocument7 pagesSubjective Global Nutrition Assessment Childrenmaricarmen IbarraNo ratings yet
- Developing and Validating A Renal Nutrition Screening Tool To Effectively Identify Undernutrition Risk Among Renal InpatientsDocument9 pagesDeveloping and Validating A Renal Nutrition Screening Tool To Effectively Identify Undernutrition Risk Among Renal Inpatientsluis Gomez VallejoNo ratings yet
- Early Enteral Versus Early Parenteral Nutrition in Critically Ill Patients With Respiratory Distress - A Case-Control StudyDocument9 pagesEarly Enteral Versus Early Parenteral Nutrition in Critically Ill Patients With Respiratory Distress - A Case-Control StudyNuralisaNo ratings yet
- Nutrients 15 03239 v2Document15 pagesNutrients 15 03239 v2arina fatharaniNo ratings yet
- TMP ABB8Document10 pagesTMP ABB8FrontiersNo ratings yet
- A Practical Approach To Nutritional Screening and Assessment in CirrhosisDocument14 pagesA Practical Approach To Nutritional Screening and Assessment in Cirrhosispamela Urrutia100% (1)
- Indicaciones NP Onc PedDocument7 pagesIndicaciones NP Onc PedSebastian MarinNo ratings yet
- Ultraprocessed Foods and Excess Heart Age Among Us AdultsDocument10 pagesUltraprocessed Foods and Excess Heart Age Among Us AdultsSaionara FranciscoNo ratings yet
- Journal of Clinical Gerontology & Geriatrics: Camilla Jing Hwa Chern, BS, Shyh-Dye Lee, MD, MPHDocument5 pagesJournal of Clinical Gerontology & Geriatrics: Camilla Jing Hwa Chern, BS, Shyh-Dye Lee, MD, MPHEdith Frederick LiemNo ratings yet
- Dietary Patterns Exhibit Sex-Specific 3Document9 pagesDietary Patterns Exhibit Sex-Specific 3Luiz Eduardo RodriguezNo ratings yet
- Aspectos Importantes de La Nutrición en Niños Con CáncerDocument11 pagesAspectos Importantes de La Nutrición en Niños Con CáncerNadia DonosoNo ratings yet
- Internasional PDFDocument7 pagesInternasional PDFseptianarifwandiniNo ratings yet
- Ophthalmology 2008 p822Document9 pagesOphthalmology 2008 p822Olvaria MisfaNo ratings yet
- Nutritional Assessment of Children With CHD CompareDocument9 pagesNutritional Assessment of Children With CHD CompareIntan Robi'ahNo ratings yet
- ESPEN Guideline On Clinical Nutrition in Inflammatory Bowel DiseaseDocument28 pagesESPEN Guideline On Clinical Nutrition in Inflammatory Bowel DiseaseAi NurfaiziyahNo ratings yet
- Nmaa 108Document20 pagesNmaa 108fidya ardinyNo ratings yet
- Anthropometry Assessment in Children With Disease Related MalnutritionDocument10 pagesAnthropometry Assessment in Children With Disease Related Malnutritionberlian29031992No ratings yet
- Nutrition in Critical Care: R. Chowdhury and S. LobazDocument6 pagesNutrition in Critical Care: R. Chowdhury and S. LobazVictoria PoNo ratings yet
- 1 s2.0 S0261561423000274 MainDocument15 pages1 s2.0 S0261561423000274 MainJulia KhaerunisaNo ratings yet
- Fnut 10 1149579Document8 pagesFnut 10 1149579juniartiyudhaNo ratings yet
- Associations of Fat and Carbohydrate Intake With Cardiovascular Disease and MortalityDocument11 pagesAssociations of Fat and Carbohydrate Intake With Cardiovascular Disease and MortalityMateo PeychauxNo ratings yet
- Cardenas 2021 Nday 2 JPEN Jpen.2085Document10 pagesCardenas 2021 Nday 2 JPEN Jpen.2085CamilaNo ratings yet
- The Antioxidants in Prevention of Cataracts Study: Effects of Antioxidant Supplements On Cataract Progression in South IndiaDocument5 pagesThe Antioxidants in Prevention of Cataracts Study: Effects of Antioxidant Supplements On Cataract Progression in South IndiaNeti WatiniNo ratings yet
- Nutritional Intake, Environmental Factors, and Their Impact On Myopia Prevalence in Korean Children Aged 5-12 YearsDocument13 pagesNutritional Intake, Environmental Factors, and Their Impact On Myopia Prevalence in Korean Children Aged 5-12 YearsOwais SaeedNo ratings yet
- J Parenter Enteral Nutr - 2022 - Gressies - Nutrition Issues in The General Medical Ward Patient From General Screening ToDocument8 pagesJ Parenter Enteral Nutr - 2022 - Gressies - Nutrition Issues in The General Medical Ward Patient From General Screening ToRaiden EiNo ratings yet
- Efficacy of Leptin and Adiponectin For Increased Insulin Resistance in Childhood ObesityDocument11 pagesEfficacy of Leptin and Adiponectin For Increased Insulin Resistance in Childhood ObesityDr. Ahmed Ghdhban Al-ZiaydiNo ratings yet
- Piis1036731421001144 PDFDocument7 pagesPiis1036731421001144 PDFvaloranthakam10No ratings yet
- Espen FQ NiñosDocument5 pagesEspen FQ NiñosCarla ANo ratings yet
- Nutritional Issues Faced by Patients With Intestinal Stoma. A Narrative Review. 2023Document14 pagesNutritional Issues Faced by Patients With Intestinal Stoma. A Narrative Review. 2023Oliver TateNo ratings yet
- Nutrition Therapy in Critically Ill Patients A Review of Current Evidence For CliniciansDocument7 pagesNutrition Therapy in Critically Ill Patients A Review of Current Evidence For CliniciansangiolikkiaNo ratings yet
- Proceedings 02 00573 v3Document186 pagesProceedings 02 00573 v3André SartorelliNo ratings yet
- Evaluation of Nutrition Status Using The Subjective Global Assessment: Malnutrition, Cachexia, and SarcopeniaDocument15 pagesEvaluation of Nutrition Status Using The Subjective Global Assessment: Malnutrition, Cachexia, and SarcopeniaLia. OktarinaNo ratings yet
- Children 09 01031Document12 pagesChildren 09 01031AIRA MARIE DOROTEONo ratings yet
- Diabetes & Metabolic Syndrome: Clinical Research & ReviewsDocument7 pagesDiabetes & Metabolic Syndrome: Clinical Research & ReviewsOdilia Rondang Mauli SimarmataNo ratings yet
- Nutrición Personalizada para Prevención de DemenciaDocument14 pagesNutrición Personalizada para Prevención de DemenciaMelisa RieloNo ratings yet
- Early Energy and Protein Intakes and AssociationsDocument7 pagesEarly Energy and Protein Intakes and Associationspaulo.freitas.machrentNo ratings yet
- SAM and Infections Technical Brief2 CMAM Forum May 2013Document52 pagesSAM and Infections Technical Brief2 CMAM Forum May 2013adan yareNo ratings yet
- Gastroparesis: A Comprehensive Approach to Evaluation and ManagementFrom EverandGastroparesis: A Comprehensive Approach to Evaluation and ManagementAnna IbeleNo ratings yet
- Botanical Orign: Peppermint OilDocument4 pagesBotanical Orign: Peppermint OilSidra TariqNo ratings yet
- 1000 English Collocations EbookDocument128 pages1000 English Collocations EbookHerdeiro DicaprioNo ratings yet
- Petroleum Refining Notes 1Document5 pagesPetroleum Refining Notes 1api-304149645No ratings yet
- Ch123 Exam II Practice Exam Spring2011Document7 pagesCh123 Exam II Practice Exam Spring2011christopher92530% (1)
- The Approach To Dysmorphic ChildDocument14 pagesThe Approach To Dysmorphic ChildBelinderjit KaurNo ratings yet
- Acids, Bases and Salt Preparations 1 QPDocument8 pagesAcids, Bases and Salt Preparations 1 QPAbdullah SheikhNo ratings yet
- Natural Remedies For Heart DiseaseDocument8 pagesNatural Remedies For Heart DiseaseNur HowladerNo ratings yet
- GENED 200 ItemsDocument235 pagesGENED 200 ItemsBRIAN100% (1)
- Shamanic HealingDocument41 pagesShamanic HealingMeraki Mary50% (2)
- LA Myxoma Case PresentationDocument34 pagesLA Myxoma Case PresentationWiwik Puji LestariNo ratings yet
- Diagnostic Fault Codes: Quick Reference GuideDocument2 pagesDiagnostic Fault Codes: Quick Reference GuideJavier VillelaNo ratings yet
- Top 10 Tips From ZOE Science and NutritionDocument5 pagesTop 10 Tips From ZOE Science and NutritionGabaNo ratings yet
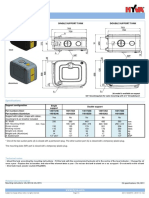
- Hyva Oil Tank: Single Support Tank Double Support TankDocument4 pagesHyva Oil Tank: Single Support Tank Double Support TankPutera Bumi NusantaraNo ratings yet
- Agrismart's Farm Water Solution An Alternative To Mains WaterDocument3 pagesAgrismart's Farm Water Solution An Alternative To Mains WaterPR.comNo ratings yet
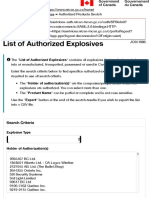
- NRCan's Explosives Eservices - Authorized Products SearchDocument5 pagesNRCan's Explosives Eservices - Authorized Products SearchDiego VilaNo ratings yet
- Offtake Oc035 Preparation Go No Go ChecklistDocument8 pagesOfftake Oc035 Preparation Go No Go ChecklistIhwan AsrulNo ratings yet
- F1.4 - Marine Sediment Treatment and ReuseDocument14 pagesF1.4 - Marine Sediment Treatment and ReuseKwan Chun SingNo ratings yet
- Indira Gandhi National Widow Pension SchemeDocument3 pagesIndira Gandhi National Widow Pension SchemeNavinkumar RohitNo ratings yet
- Tugas Rapid Silvia AplianiDocument11 pagesTugas Rapid Silvia AplianiSilvia AplianiNo ratings yet
- (II) Misadventure Is Mischance, Accident or Disaster. It Is of Three TypesDocument3 pages(II) Misadventure Is Mischance, Accident or Disaster. It Is of Three TypesSandeep BansalNo ratings yet
- Chapter 1 ThermochemistryDocument78 pagesChapter 1 Thermochemistrymikki11No ratings yet
- Pooja Sharma ThesisDocument66 pagesPooja Sharma ThesissknagarNo ratings yet
- RA For Assessment For Lifting OperationsDocument19 pagesRA For Assessment For Lifting OperationsMohamedSaidNo ratings yet
- Soy Source: Polarity TherapyDocument2 pagesSoy Source: Polarity TherapyrooNo ratings yet
- Hawthorne ExperimentsDocument14 pagesHawthorne ExperimentsShalini SharmaNo ratings yet
- Recruitment MSCDocument40 pagesRecruitment MSCViji MNo ratings yet
- Salvador Sanchez Complaint SignedDocument2 pagesSalvador Sanchez Complaint SignedStephen LoiaconiNo ratings yet
- HPV and Related Diseases Report HPV Informacion CentreDocument303 pagesHPV and Related Diseases Report HPV Informacion CentreRenée Elizade Martinez-PeñuelaNo ratings yet