Download as docx, pdf, or txt
You might also like
- Hypertension: Rojina Bhurtel Lecturer MmihsDocument36 pagesHypertension: Rojina Bhurtel Lecturer MmihsRojina Bhurtel100% (2)
- Input Process OutputDocument1 pageInput Process OutputJheanAlphonsineT.MeansNo ratings yet
- COURSE TASK 2 Mrs. Clot's and Alexa's Case - POLICIOS, SHARMAINE ANNE M. BSN 3Y2 - 3ADocument10 pagesCOURSE TASK 2 Mrs. Clot's and Alexa's Case - POLICIOS, SHARMAINE ANNE M. BSN 3Y2 - 3ASHARMAINE ANNE POLICIOSNo ratings yet
- Medication CardsDocument65 pagesMedication CardsMovaliya Ghanshyam80% (5)
- Measles Differential DiagnosisDocument1 pageMeasles Differential Diagnosistobechi86No ratings yet
- Hypertension Written ReportDocument5 pagesHypertension Written ReportKate Felongco CambelNo ratings yet
- Hypertension: Edet Unyime Treasure 019/0102/0077Document11 pagesHypertension: Edet Unyime Treasure 019/0102/0077Akinsoun MotunrayoNo ratings yet
- Hypertension OutlineDocument6 pagesHypertension OutlineZJ GarcianoNo ratings yet
- Classification: HypertensionDocument13 pagesClassification: HypertensiontermskipopNo ratings yet
- Hypertension: Prepared By: Eden Marie D. Francisco Lorraine Nicolne B. CortejoDocument27 pagesHypertension: Prepared By: Eden Marie D. Francisco Lorraine Nicolne B. CortejoAlecNo ratings yet
- HypertensionDocument21 pagesHypertensionM RaisNo ratings yet
- Hypertension OutlineDocument14 pagesHypertension OutlineMaria CayacoNo ratings yet
- Kuliah Hipertensi KMB1 2018Document43 pagesKuliah Hipertensi KMB1 2018Ainu RamadhaniNo ratings yet
- Health Teaching PlanDocument10 pagesHealth Teaching PlanMariel Colminas100% (2)
- DBP: Diastolic Blood Pressure SBP: Systolic Blood PressureDocument7 pagesDBP: Diastolic Blood Pressure SBP: Systolic Blood PressureM. JoyceNo ratings yet
- Hypertension: Medlineplus TopicsDocument31 pagesHypertension: Medlineplus TopicsMcNover Catlin OsamNo ratings yet
- HypertensionDocument55 pagesHypertensionSr.Jyothy SABSNo ratings yet
- Hypertension and Antihypertensives (Iniaghe) Physiotherapy Students Oct 2021Document15 pagesHypertension and Antihypertensives (Iniaghe) Physiotherapy Students Oct 2021s9hdy4gsqrNo ratings yet
- Presented by Asmaa Abdelhameed AhmedDocument24 pagesPresented by Asmaa Abdelhameed AhmedSoma Al-mutairiNo ratings yet
- HYPERTENSIONDocument10 pagesHYPERTENSIONChelsea Faith SarandiNo ratings yet
- HypertensionDocument10 pagesHypertensionRima HannaniNo ratings yet
- Isyncope: Partial or Complete Loss of Consciousness With Interruption of Awareness of Oneself and OnesDocument4 pagesIsyncope: Partial or Complete Loss of Consciousness With Interruption of Awareness of Oneself and OnesLimLichynNo ratings yet
- LAS 4 Drugs For HypertensionDocument28 pagesLAS 4 Drugs For HypertensionMuhammad Haroon RazaNo ratings yet
- 5 Nutrition Therapy For Cardiovascular DiseasesDocument74 pages5 Nutrition Therapy For Cardiovascular Diseaseskarinablanca adranedaNo ratings yet
- Allied Health-Blood Pressure Class AssignmentDocument4 pagesAllied Health-Blood Pressure Class Assignmentapi-385125344No ratings yet
- Hypertension LectureDocument10 pagesHypertension LectureHarold CapidosNo ratings yet
- Emediong SeminarDocument33 pagesEmediong SeminarItoro UdohNo ratings yet
- HypertensionDocument36 pagesHypertensionmohamedahmedf12345678No ratings yet
- Drug Presentation On Anti-Hypertensive: All India Institute of Medical and Science New Delhi 2021-2022Document12 pagesDrug Presentation On Anti-Hypertensive: All India Institute of Medical and Science New Delhi 2021-2022Priya SinghNo ratings yet
- Case Study 4Document10 pagesCase Study 4api-440408997No ratings yet
- Unit 3: Diet in Health and Disease: IIDocument69 pagesUnit 3: Diet in Health and Disease: IItestNo ratings yet
- HYPERTENSION, Also Known As High Blood Pressure Affects MillionsDocument7 pagesHYPERTENSION, Also Known As High Blood Pressure Affects MillionsPrince KarikariNo ratings yet
- Hypertension: High Blood PressureDocument6 pagesHypertension: High Blood PressureAnne BattulayanNo ratings yet
- Hypertension (High Blood Pressure) Is A Disease of Vascular Regulation Resulting From Malfunction ofDocument4 pagesHypertension (High Blood Pressure) Is A Disease of Vascular Regulation Resulting From Malfunction ofkewpietheresaNo ratings yet
- Vasucular DiseasesDocument43 pagesVasucular DiseasesSufiyan AbduramanNo ratings yet
- Report About HypertensionDocument11 pagesReport About HypertensionZA IDNo ratings yet
- Pharmacology: Unit VIIIDocument92 pagesPharmacology: Unit VIIIChristian Laraya AlayonNo ratings yet
- Hypertension KLP 10Document16 pagesHypertension KLP 10Tri ArdiyaniNo ratings yet
- GeronDocument54 pagesGeronL Rean Carmelle MAGALLONESNo ratings yet
- Hypertension: Margaret Xaira R. Mercado RNDocument36 pagesHypertension: Margaret Xaira R. Mercado RNMargaret Xaira Rubio MercadoNo ratings yet
- Nutrition Therapy For Cardiovascular DiseasesDocument43 pagesNutrition Therapy For Cardiovascular DiseasesChelo Jan GeronimoNo ratings yet
- Presented To: Dr. Lakshmi Dodda Presented By: Nicolas Abdel NourDocument33 pagesPresented To: Dr. Lakshmi Dodda Presented By: Nicolas Abdel NourNicolas Abdel NourNo ratings yet
- Hypertension Definition:: Nitric OxideDocument5 pagesHypertension Definition:: Nitric OxideAnonymous bbeAZHxZNo ratings yet
- Cardiovascular FunctionDocument157 pagesCardiovascular FunctionJonnabelle PadillaNo ratings yet
- What Is High Blood PressureDocument4 pagesWhat Is High Blood PressureBudhi AstawaNo ratings yet
- Gerontic Nursing: Elderly With Hypertension: Arranged Group 11: Suci Aulia (1714201042)Document15 pagesGerontic Nursing: Elderly With Hypertension: Arranged Group 11: Suci Aulia (1714201042)anisaNo ratings yet
- Pulmonary HypertensionDocument3 pagesPulmonary HypertensionJiezl Abellano AfinidadNo ratings yet
- Hypertension: Dosen PengampuDocument9 pagesHypertension: Dosen Pengampulilis wulandariNo ratings yet
- Primary AldosteronismDocument31 pagesPrimary AldosteronismSteph100% (1)
- Understanding Low Blood Pressure - The BasicsDocument6 pagesUnderstanding Low Blood Pressure - The BasicsRajeev Nechiyil100% (1)
- HypertensionDocument12 pagesHypertensionDr. PARMINDER NAINNo ratings yet
- Hypertension: Jumarang, Kim Enrico M. BSN401 STI - Global CityDocument6 pagesHypertension: Jumarang, Kim Enrico M. BSN401 STI - Global CityKim Enrico JumarangNo ratings yet
- HypertensionDocument10 pagesHypertensionaa zzNo ratings yet
- AntihypertensiveDocument7 pagesAntihypertensiveAKASH BISWASNo ratings yet
- Antihypertensive Drugs Lecture-1Document94 pagesAntihypertensive Drugs Lecture-1onyeukwudaniel12No ratings yet
- Lesson 5 Hypertension Notes White BGDocument15 pagesLesson 5 Hypertension Notes White BGWaliid Khan 5SNo ratings yet
- Ingles HTADocument8 pagesIngles HTAlizalfonso02No ratings yet
- Final Intro HTNDocument28 pagesFinal Intro HTNHanwell Keith SantosNo ratings yet
- Hypertensive Cardiovascular Disease Also Known As Hypertensive Heart Disease Occurs Due To The Complication of Hypertension or High Blood PressureDocument3 pagesHypertensive Cardiovascular Disease Also Known As Hypertensive Heart Disease Occurs Due To The Complication of Hypertension or High Blood Pressurejoanneceline16No ratings yet
- Chapter 31 HypertensionDocument3 pagesChapter 31 HypertensionVen SemillaNo ratings yet
- HTNDocument35 pagesHTNnathanielNo ratings yet
- Hyper TentionDocument19 pagesHyper TentionAnthony MarkNo ratings yet
- Hypertension Mini Case StudyDocument5 pagesHypertension Mini Case Studymaeca101100% (1)
- Health Teaching PlanDocument3 pagesHealth Teaching PlanJheanAlphonsineT.MeansNo ratings yet
- Nursing Prioritization, Delegation and Assignment, INFECTION CONTROLDocument7 pagesNursing Prioritization, Delegation and Assignment, INFECTION CONTROLJheanAlphonsineT.Means100% (1)
- Pediatric Nursing Review BulletsDocument3 pagesPediatric Nursing Review BulletsJheanAlphonsineT.MeansNo ratings yet
- Major Depressive DisorderDocument11 pagesMajor Depressive DisorderJheanAlphonsineT.MeansNo ratings yet
- UROLITHIASISDocument84 pagesUROLITHIASISJheanAlphonsineT.MeansNo ratings yet
- Bulimia NervosaDocument17 pagesBulimia NervosaJheanAlphonsineT.Means100% (1)
- Grad Ball Program FlowDocument1 pageGrad Ball Program FlowJheanAlphonsineT.MeansNo ratings yet
- Case 2Document5 pagesCase 2JheanAlphonsineT.MeansNo ratings yet
- CA Risk For Infection NCPDocument2 pagesCA Risk For Infection NCPJheanAlphonsineT.MeansNo ratings yet
- NCP #1 Acute PainDocument3 pagesNCP #1 Acute PainJheanAlphonsineT.MeansNo ratings yet
- Ca Semi FiDocument23 pagesCa Semi FiJheanAlphonsineT.MeansNo ratings yet
- Nclex ExamDocument24 pagesNclex ExamJheanAlphonsineT.MeansNo ratings yet
- Pathophysiology of Transitional Cell CarcinomaDocument10 pagesPathophysiology of Transitional Cell CarcinomaJheanAlphonsineT.MeansNo ratings yet
- The Bishop ScoreDocument3 pagesThe Bishop ScoreJheanAlphonsineT.MeansNo ratings yet
- Ursing ARE LAN: Nursing DiagnosisDocument2 pagesUrsing ARE LAN: Nursing DiagnosisJheanAlphonsineT.MeansNo ratings yet
- Types of BurnsDocument5 pagesTypes of BurnsJheanAlphonsineT.Means100% (2)
- Care of Clients in Emergent ConditionsDocument19 pagesCare of Clients in Emergent ConditionsJheanAlphonsineT.MeansNo ratings yet
- A Study On Prevalence of Bacteria in The Hands ofDocument5 pagesA Study On Prevalence of Bacteria in The Hands ofhudaNo ratings yet
- Modules Pe 1 (Lesson 5)Document12 pagesModules Pe 1 (Lesson 5)Jose Emmanuel CalagNo ratings yet
- Comparative Study of Using Ddfao Esg SystemDocument18 pagesComparative Study of Using Ddfao Esg SystemCao Minh Trí100% (1)
- Photophobia: Light Sensitivity and Migraines - Webmd: Web ResultsDocument3 pagesPhotophobia: Light Sensitivity and Migraines - Webmd: Web ResultsRheaniesse TreveriaNo ratings yet
- Healthcare Associated Infections in The Nicu PowerpointDocument21 pagesHealthcare Associated Infections in The Nicu Powerpointapi-489132887No ratings yet
- ORAL CANCER ADOD-2-110 Annals of Dentistry and Oral Disorders Ambarkova Oral CancerDocument2 pagesORAL CANCER ADOD-2-110 Annals of Dentistry and Oral Disorders Ambarkova Oral CancerVesna AmbarkovaNo ratings yet
- Sample NURSING PROCESS IN PHARMACOLOGY PDFDocument7 pagesSample NURSING PROCESS IN PHARMACOLOGY PDFVic Intia PaaNo ratings yet
- Factors Contributing To Kidney Allograft Loss and Associated Consequences Among Post Kidney Transplantation PatientsDocument11 pagesFactors Contributing To Kidney Allograft Loss and Associated Consequences Among Post Kidney Transplantation PatientsRafela Agatha ChristyNo ratings yet
- Point-of-Care Testing Millennium Technology For CRDocument7 pagesPoint-of-Care Testing Millennium Technology For CRBrendaCelina MejíaAguayoNo ratings yet
- iTEC and VTCT Qualifications For Remote Delivery V 3Document7 pagesiTEC and VTCT Qualifications For Remote Delivery V 3Alexis O'SullivanNo ratings yet
- 10 1016@j Wneu 2019 01 093 PDFDocument16 pages10 1016@j Wneu 2019 01 093 PDFfira rifaNo ratings yet
- Systematic Review - Cardiac LipomaDocument7 pagesSystematic Review - Cardiac LipomaEspecialização EcocardiografiaNo ratings yet
- PCL's Avulsion FractureDocument22 pagesPCL's Avulsion FractureNey da OnneyNo ratings yet
- Stefania Boccia, Paolo Villari, Walter Ricciardi (Eds.) - A Systematic Review of Key Issues in Public Health (2015, Springer International Publishing)Document294 pagesStefania Boccia, Paolo Villari, Walter Ricciardi (Eds.) - A Systematic Review of Key Issues in Public Health (2015, Springer International Publishing)Agus GunadiNo ratings yet
- Sensitivity: The Ability of A Test ToDocument133 pagesSensitivity: The Ability of A Test ToKim DeeNo ratings yet
- Borderline Personality Disorder - 0Document8 pagesBorderline Personality Disorder - 0Vanshla GuptaNo ratings yet
- Huntington's Disease Comment PieceDocument1 pageHuntington's Disease Comment PieceJuze DowdeeNo ratings yet
- Andrew Idoko Group 332 Variant 14 Explain The Pathogenesis of Clinical Signs and Symptoms of Fanconi AnemiaDocument2 pagesAndrew Idoko Group 332 Variant 14 Explain The Pathogenesis of Clinical Signs and Symptoms of Fanconi AnemiadreNo ratings yet
- Pil 6542Document7 pagesPil 6542GodlyNoobNo ratings yet
- Band 5 QuestionsDocument9 pagesBand 5 Questionsdan iacobNo ratings yet
- Substance UseDocument3 pagesSubstance UseAlbert SamanteNo ratings yet
- Sociology Research PaperDocument11 pagesSociology Research PaperElsa ShaikhNo ratings yet
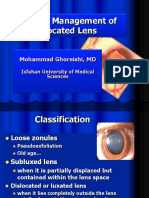
- Surgical Management of Dilocated Lens: Mohammad Ghoreishi, MDDocument15 pagesSurgical Management of Dilocated Lens: Mohammad Ghoreishi, MDwawan 88No ratings yet
- Moisture-Associated Skin Damage (MASD) - Tear CollectionDocument14 pagesMoisture-Associated Skin Damage (MASD) - Tear CollectionIchigo RukiaNo ratings yet
- Case 1 Pedia Henoch Schonlein PurpuraDocument45 pagesCase 1 Pedia Henoch Schonlein PurpuraJefferson Gumiran100% (1)
- NNF Guidelines 2011Document344 pagesNNF Guidelines 2011Vijay Dihora0% (1)
- Activity Exercise PatternDocument4 pagesActivity Exercise PatternButchay LumbabNo ratings yet