Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Placenta Previa PathophysiologyDocument1 pagePlacenta Previa Pathophysiologykathy85% (20)
- Syndrome, (Exploratory Behavior and Hypersexuality) : Function of The Limbic CortexDocument2 pagesSyndrome, (Exploratory Behavior and Hypersexuality) : Function of The Limbic CortexFathy ElsheshtawyNo ratings yet
- "Reward" and "Punishment" Function of The Limbic SystemDocument2 pages"Reward" and "Punishment" Function of The Limbic SystemFathy ElsheshtawyNo ratings yet
- Functional Anatomy of The Limbic System Key Position of The HypothalamusDocument1 pageFunctional Anatomy of The Limbic System Key Position of The HypothalamusFathy ElsheshtawyNo ratings yet
- Name Age No - Admission Date Provisiona L DiagnosisDocument2 pagesName Age No - Admission Date Provisiona L DiagnosisFathy ElsheshtawyNo ratings yet
- Thelimb 1Document1 pageThelimb 1Fathy ElsheshtawyNo ratings yet
- Functional Anatomy ofDocument1 pageFunctional Anatomy ofFathy ElsheshtawyNo ratings yet
- Hypothalamus, A Major Control Headquarters For The Limbic SystemDocument2 pagesHypothalamus, A Major Control Headquarters For The Limbic SystemFathy ElsheshtawyNo ratings yet
- List of Neurologist Epileptologist EgyptDocument7 pagesList of Neurologist Epileptologist EgyptFathy ElsheshtawyNo ratings yet
- Medical Investigations PDFDocument136 pagesMedical Investigations PDFFathy ElsheshtawyNo ratings yet
- Index: Bacterial Viral TB Vs Polio CNS Meningitis PUO Immunization Parasitic InfestationDocument1 pageIndex: Bacterial Viral TB Vs Polio CNS Meningitis PUO Immunization Parasitic InfestationFathy ElsheshtawyNo ratings yet
- Placement TestDocument10 pagesPlacement TestFathy ElsheshtawyNo ratings yet
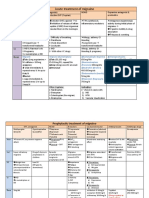
- Acute Treatment of Migraine: ActionDocument3 pagesAcute Treatment of Migraine: ActionFathy ElsheshtawyNo ratings yet
- Prophylactic: Factors Affecting TTTDocument14 pagesProphylactic: Factors Affecting TTTFathy ElsheshtawyNo ratings yet
- AUBDocument10 pagesAUBFathy ElsheshtawyNo ratings yet
- Abnormal Uterine Bleeding: Physiological Methods Barrier Methods Mechanical Methods Chemical MethodsDocument8 pagesAbnormal Uterine Bleeding: Physiological Methods Barrier Methods Mechanical Methods Chemical MethodsFathy ElsheshtawyNo ratings yet
- Contraception MCQ: B) No AndrogensDocument1 pageContraception MCQ: B) No AndrogensFathy ElsheshtawyNo ratings yet
- Urology (CTIN) V2Document45 pagesUrology (CTIN) V2Fathy ElsheshtawyNo ratings yet
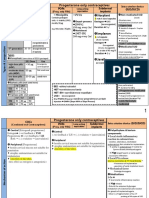
- Norplant: Progesterone Only ContraceptivesDocument9 pagesNorplant: Progesterone Only ContraceptivesFathy ElsheshtawyNo ratings yet
- VulvodyniaDocument5 pagesVulvodyniaTrapedNo ratings yet
- Endometriosis Case Presentation by Nkoro Edward-1Document27 pagesEndometriosis Case Presentation by Nkoro Edward-1Brie IpehNo ratings yet
- Science: The Menstrual CycleDocument4 pagesScience: The Menstrual CycleLena Beth Tapawan YapNo ratings yet
- Lesson 4 Biomedical Perspective in Gender Sexuality 2Document28 pagesLesson 4 Biomedical Perspective in Gender Sexuality 2Nikka GoenettNo ratings yet
- Obstetrics & MaternityDocument4 pagesObstetrics & MaternityBlue TechNo ratings yet
- 3rd Lecture On The Histology of Female Reproductive System by Dr. RoomiDocument19 pages3rd Lecture On The Histology of Female Reproductive System by Dr. RoomiMudassar RoomiNo ratings yet
- Ob ClinicsDocument13 pagesOb ClinicsLj chuaNo ratings yet
- Jurnal Kuda 1Document21 pagesJurnal Kuda 1Yulistia FadhilahNo ratings yet
- Laporan Instalasi Kamar Operasi Rsia Sitti Khadijah 1 Makassar Bulan 01 Tahun 2019 No Tanggal No - RM Nama Pasien DiagnosaDocument41 pagesLaporan Instalasi Kamar Operasi Rsia Sitti Khadijah 1 Makassar Bulan 01 Tahun 2019 No Tanggal No - RM Nama Pasien DiagnosaYuli AntiNo ratings yet
- Abnormal Uterine Bleeding in Reproductive-Age Patients: FIGO System 1 Terminology and Symptoms and SDocument2 pagesAbnormal Uterine Bleeding in Reproductive-Age Patients: FIGO System 1 Terminology and Symptoms and SMariana HernandezNo ratings yet
- Female GenitaliaDocument96 pagesFemale GenitaliaJopaii TanakaNo ratings yet
- SOX Science5 Q2 M2of7Document18 pagesSOX Science5 Q2 M2of7Neil Joy Felomino Basa-LepalemNo ratings yet
- Case Analaysis On infertility-BALLON-Karlo CDocument4 pagesCase Analaysis On infertility-BALLON-Karlo CMelinda Cariño BallonNo ratings yet
- Infeksi Organ Genital DR Alfaina - Id.enDocument45 pagesInfeksi Organ Genital DR Alfaina - Id.enJ KrystalNo ratings yet
- Septum Uterino Transverso Por HisterosDocument14 pagesSeptum Uterino Transverso Por HisterosmilifeerNo ratings yet
- GYNECOLOGY Chief ComplaintsDocument3 pagesGYNECOLOGY Chief ComplaintsJennifer HerediaNo ratings yet
- Amenorrhea UpdatedDocument30 pagesAmenorrhea UpdatedAbdi fatah ali1No ratings yet
- Endometrial BiopsyDocument72 pagesEndometrial BiopsySatish TatamiyaNo ratings yet
- Leiomyoma of The UterusDocument17 pagesLeiomyoma of The UterussanjivdasNo ratings yet
- Menstrual DisordersDocument45 pagesMenstrual DisordersMegat Mohd Azman Adzmi100% (1)
- Asherman Syndrome and Chronic Chlamydial Infection With Fitz-Hugh-Curtis Syndrome in Women With Secondary InfertilityDocument5 pagesAsherman Syndrome and Chronic Chlamydial Infection With Fitz-Hugh-Curtis Syndrome in Women With Secondary InfertilityPyuzz RemakeNo ratings yet
- An Activity On MenstruationDocument3 pagesAn Activity On Menstruationthabisojunior369No ratings yet
- Abnormal Uterine BleedingDocument36 pagesAbnormal Uterine BleedingPranshu Prajyot 67100% (1)
- Maternal and Child Health NursingDocument6 pagesMaternal and Child Health NursingRoanne DivinagraciaNo ratings yet
- 2009-10 Menstrual CalendarDocument1 page2009-10 Menstrual CalendarJeffersonLuvrNo ratings yet
- Hormonal CycleDocument20 pagesHormonal CycleGunaNo ratings yet
- Modified Manchester de BoerDocument7 pagesModified Manchester de BoerGustavo flores quispeNo ratings yet
- SGD Week 2 - Abnormal Uterine Bleeding Gr4Document39 pagesSGD Week 2 - Abnormal Uterine Bleeding Gr4Andrea GuarinNo ratings yet
- Adenomyosis Fact SheetDocument4 pagesAdenomyosis Fact SheetAnonymous AZ2Z4FhV9zNo ratings yet