Download as pdf or txt
You might also like
- PostGraduate Vascular SurgeryDocument339 pagesPostGraduate Vascular SurgeryAmyand100% (1)
- Balneo 305Document6 pagesBalneo 305Nicoleta TudorachiNo ratings yet
- Journal EadiologiDocument5 pagesJournal EadiologiAhmad IsmatullahNo ratings yet
- Complications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFDocument19 pagesComplications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFSergio Tomas Cortés MoralesNo ratings yet
- Chronic Knee Pain Is The Paramount Presentation in Patients With Nail Patella SyndromeDocument7 pagesChronic Knee Pain Is The Paramount Presentation in Patients With Nail Patella SyndromeAthenaeum Scientific PublishersNo ratings yet
- West Indian Medical Journal: A Case of Pathological Rib Fractures: Focal Osteolysis or Osteoporosis?Document10 pagesWest Indian Medical Journal: A Case of Pathological Rib Fractures: Focal Osteolysis or Osteoporosis?IstianahNo ratings yet
- Laprade 2012Document11 pagesLaprade 2012Aaron BNo ratings yet
- Evaluating Lumbar Spine 582-589Document8 pagesEvaluating Lumbar Spine 582-589Mansour ZamaniNo ratings yet
- Painful Knee 2024 International Journal of Surgery Case ReportsDocument6 pagesPainful Knee 2024 International Journal of Surgery Case ReportsRonald QuezadaNo ratings yet
- Case Report - 14 Years-Old Boy With Paraplegia and Aneurysmal Bone Cysts of Neck Who Responded To Anti-Tuberculosis TreatmentDocument3 pagesCase Report - 14 Years-Old Boy With Paraplegia and Aneurysmal Bone Cysts of Neck Who Responded To Anti-Tuberculosis TreatmentMadya WicaksonoNo ratings yet
- Endoscopic Release of The Piriformis TendonDocument6 pagesEndoscopic Release of The Piriformis TendonKinjal SharmaNo ratings yet
- Management of Incarcerating Pincer-Type Femoroacetabular Impingement With Hip Arthroscopy - Arthroscopy TechniquesDocument1 pageManagement of Incarcerating Pincer-Type Femoroacetabular Impingement With Hip Arthroscopy - Arthroscopy TechniquesNica ReyesNo ratings yet
- Postoperative Radiograph of The Hip Arthroplasty: What The Radiologist Should KnowDocument11 pagesPostoperative Radiograph of The Hip Arthroplasty: What The Radiologist Should KnowSurya AbigamikaNo ratings yet
- P ('t':'3', 'I':'669333659') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Document6 pagesP ('t':'3', 'I':'669333659') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)deadcorpsesNo ratings yet
- Pathological Gait Patterns in Coxa Retrotorta in Pediatric Population-Supplementary Examination For Preoperative Planning?Document2 pagesPathological Gait Patterns in Coxa Retrotorta in Pediatric Population-Supplementary Examination For Preoperative Planning?Gabriela Istrati-StanciugelNo ratings yet
- Effects Er Vics Pondy LozDocument7 pagesEffects Er Vics Pondy Lozokan karabulutNo ratings yet
- Nice 1stDocument6 pagesNice 1staldiNo ratings yet
- Wakefield - 2008Document6 pagesWakefield - 2008TurboNo ratings yet
- Arthroscopic Debridement and Drilling of Osteochondral Lesions of The TalusDocument15 pagesArthroscopic Debridement and Drilling of Osteochondral Lesions of The TalusAnonymous kdBDppigENo ratings yet
- The Modified Brostr M Gould Procedure - Early Results Usi - 2014 - Foot and AnklDocument5 pagesThe Modified Brostr M Gould Procedure - Early Results Usi - 2014 - Foot and AnklFyodorovich Makarov NikolaiNo ratings yet
- Shital N Parikh 4 in 1 Quadricepsplasty For HabitualDocument9 pagesShital N Parikh 4 in 1 Quadricepsplasty For HabitualDrSheenam BansalNo ratings yet
- Effects On Inadvertent Endplate Fracture Following Lateral Cage Placement On Range of Motion and Indirect Spine Decompression in Lumbar Spine Fusion Constructs: A Cadaveric StudyDocument8 pagesEffects On Inadvertent Endplate Fracture Following Lateral Cage Placement On Range of Motion and Indirect Spine Decompression in Lumbar Spine Fusion Constructs: A Cadaveric Studysiti hanifahNo ratings yet
- Fagan 2004Document11 pagesFagan 2004Hari25885No ratings yet
- So Sang Sieu Am Va MriDocument12 pagesSo Sang Sieu Am Va Mrithu hangNo ratings yet
- Posterior Lumbar Interbody Fusion (PLIF) With Cages and Local Bone Graft in The Treatment of Spinal StenosisDocument7 pagesPosterior Lumbar Interbody Fusion (PLIF) With Cages and Local Bone Graft in The Treatment of Spinal StenosisMd.Shafiul EzazNo ratings yet
- Spinous Process Fractures in Osteoporotic Thoracolumbar Vertebral FracturesDocument4 pagesSpinous Process Fractures in Osteoporotic Thoracolumbar Vertebral FracturesAditya Arya PutraNo ratings yet
- Femoral Head Osteonecrosis Why Choose FreeDocument6 pagesFemoral Head Osteonecrosis Why Choose FreeFreestanding identificationNo ratings yet
- Overuse Ankle Injuries in Professional Irish DancersDocument5 pagesOveruse Ankle Injuries in Professional Irish DancersPookcey IdsariyaNo ratings yet
- Tatalaksana OsteonekrosisDocument78 pagesTatalaksana OsteonekrosisRama MahendraNo ratings yet
- A Literature Review of Total Hip Arthroplasty in Patients With Ankylosing Spondylitis: Perioperative Considerations and OutcomeDocument7 pagesA Literature Review of Total Hip Arthroplasty in Patients With Ankylosing Spondylitis: Perioperative Considerations and OutcomeSivabharathi SivanandamNo ratings yet
- Journal of Equine Veterinary Science: Wade T. Walker DVM, Natasha M. Werpy DVM, Dacvr, Laurie R. Goodrich DVM, PHD, DacvsDocument9 pagesJournal of Equine Veterinary Science: Wade T. Walker DVM, Natasha M. Werpy DVM, Dacvr, Laurie R. Goodrich DVM, PHD, DacvsMaria Paz MorenoNo ratings yet
- Rodilla Inervación Tran2018 PDFDocument8 pagesRodilla Inervación Tran2018 PDFLore BarreraNo ratings yet
- Isolated Calcaneocuboid Instability - A Unique DiagDocument18 pagesIsolated Calcaneocuboid Instability - A Unique Diagvijaypatel4282No ratings yet
- 460 FullDocument7 pages460 FullNasrull BinHzNo ratings yet
- Assessment of Pelvic Floor Dysfunctions Using Dynamic Magnetic Resonance ImagingDocument11 pagesAssessment of Pelvic Floor Dysfunctions Using Dynamic Magnetic Resonance ImagingsalahzotoNo ratings yet
- Morbidity and Total Knee Arthroplasty As A Long Term Sequela of Tibial Plateau FracturesDocument8 pagesMorbidity and Total Knee Arthroplasty As A Long Term Sequela of Tibial Plateau FracturesAthenaeum Scientific PublishersNo ratings yet
- Surgically Relevant Bony and Soft Tissue Anatomy of The Proximal FemurDocument9 pagesSurgically Relevant Bony and Soft Tissue Anatomy of The Proximal Femurfahaxa7201No ratings yet
- 35 Daksh EtalDocument4 pages35 Daksh EtaleditorijmrhsNo ratings yet
- Double Pelvic Osteotomy For The Treatmen of Hip Dysplasi in Ypung DogsDocument9 pagesDouble Pelvic Osteotomy For The Treatmen of Hip Dysplasi in Ypung DogsJuan C. VasquezNo ratings yet
- Cervical Facet ArthrosisDocument4 pagesCervical Facet ArthrosisMarco PeroliNo ratings yet
- Rajiv Gandhi University of Health Sciences Bengaluru, Karnataka Proforma For Registration of Subjects For DissertationDocument10 pagesRajiv Gandhi University of Health Sciences Bengaluru, Karnataka Proforma For Registration of Subjects For DissertationRachnaNo ratings yet
- The Prevalence of in The Knee Osteoarthritis ElderlyDocument5 pagesThe Prevalence of in The Knee Osteoarthritis Elderlyqurrat ul ann haiderNo ratings yet
- What Should We Be Careful of Ankle Arthroscopy?: or Thopaedic Surger yDocument9 pagesWhat Should We Be Careful of Ankle Arthroscopy?: or Thopaedic Surger yJaysellePuguonTabijeNo ratings yet
- Volume 1 Issue 1 Page 1-5 Morphometric Study of The Pedicles of Dried Adult Human Lumbar VertebraeDocument5 pagesVolume 1 Issue 1 Page 1-5 Morphometric Study of The Pedicles of Dried Adult Human Lumbar VertebraeEditorsNo ratings yet
- Assessment of The Anterior Talofibular Ligament Thickness 2017 Journal of MeDocument5 pagesAssessment of The Anterior Talofibular Ligament Thickness 2017 Journal of MeRyana Fitriana IINo ratings yet
- Quantitative and Qualitative Assessment of Posterolateral Meniscal AnatomyDocument7 pagesQuantitative and Qualitative Assessment of Posterolateral Meniscal AnatomyNuno AlimanNo ratings yet
- Imaging in Osteoarthritis 2021 YjocaDocument22 pagesImaging in Osteoarthritis 2021 Yjocaal malikNo ratings yet
- Reichenbach 2010Document6 pagesReichenbach 2010EriC. ChaN.No ratings yet
- Patellofemoral Pain: Jennifer E. Earl, PHD, Atc, Carole S. Vetter, MD, AtcDocument20 pagesPatellofemoral Pain: Jennifer E. Earl, PHD, Atc, Carole S. Vetter, MD, AtcGabriela Soto CoñuecarNo ratings yet
- Distinctive Skeletal Phenotype in Patients With Kniest DysplasiaDocument10 pagesDistinctive Skeletal Phenotype in Patients With Kniest DysplasiaAthenaeum Scientific PublishersNo ratings yet
- Bilateral Simultaneous Anterior Shoulder DislocationDocument2 pagesBilateral Simultaneous Anterior Shoulder DislocationIOSRjournalNo ratings yet
- Tendinopatia RotulianaDocument12 pagesTendinopatia RotulianaPablo GFNo ratings yet
- Exploring The Feasibility of The Use of Sphygmomanometer For Assessing Hip Abductor Muscle Strength in Avascular Necrosis Patients - A Pilot StudyDocument3 pagesExploring The Feasibility of The Use of Sphygmomanometer For Assessing Hip Abductor Muscle Strength in Avascular Necrosis Patients - A Pilot StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Bru10319 FM PDFDocument6 pagesBru10319 FM PDFR HariNo ratings yet
- Tare de TotDocument25 pagesTare de TotantohebogdanalexNo ratings yet
- 2014 RNM en Tobillo AsintomáticoDocument5 pages2014 RNM en Tobillo AsintomáticoAnyela Gineth Chisaca NieblesNo ratings yet
- Cervical Spondylotic Myelopathy Pathophysiology CLDocument10 pagesCervical Spondylotic Myelopathy Pathophysiology CLMayNo ratings yet
- Agricola RintjeDocument282 pagesAgricola RintjeBramwel MendozaNo ratings yet
- Incidental Findings of The Lumbar Spine at MRI During Herniated Intervertebral Disk Disease EvaluationDocument5 pagesIncidental Findings of The Lumbar Spine at MRI During Herniated Intervertebral Disk Disease EvaluationDyah Gaby KesumaNo ratings yet
- Kelly 2003Document18 pagesKelly 2003leidy-riverosNo ratings yet
- Case Study 3 - Knee PainDocument12 pagesCase Study 3 - Knee PainElizabeth Ho100% (9)
- What Causes Pain Behind The KneeDocument7 pagesWhat Causes Pain Behind The KneeRatnaPrasadNalamNo ratings yet
- BursitisDocument23 pagesBursitisAngie Paola RodriguezNo ratings yet
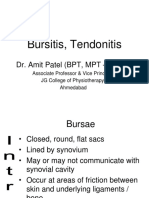
- Bursitis-Tendonitis-Dr - Amit PatelDocument52 pagesBursitis-Tendonitis-Dr - Amit PatelAmitNo ratings yet
- Writing OET Mastery 2 Scored 450Document5 pagesWriting OET Mastery 2 Scored 450Sabina Maya PantaNo ratings yet
- DVT Ultrasound Made Easy Step-By-Step GuideDocument37 pagesDVT Ultrasound Made Easy Step-By-Step GuideEL SHITANo ratings yet
- Screening Checklist: The Musculoskeletal Screening ExaminationDocument36 pagesScreening Checklist: The Musculoskeletal Screening ExaminationArden GabrielNo ratings yet
- BURSITISDocument18 pagesBURSITISmonapurwitasariNo ratings yet
- Poster Case Report Jecky Edited 2 (Final)Document1 pagePoster Case Report Jecky Edited 2 (Final)Johannes CordeNo ratings yet
- The Popliteal Fossa - Borders - Contents - TeachMeAnatomyDocument3 pagesThe Popliteal Fossa - Borders - Contents - TeachMeAnatomy147 -Ashfia HashmiNo ratings yet
- Clinical Examination of The Knee: DR John EbnezarDocument95 pagesClinical Examination of The Knee: DR John EbnezarsandeepNo ratings yet
- Pes Bursitis PubDocument9 pagesPes Bursitis PubHida IhsaniNo ratings yet
- Meniscus Root Repair RehabDocument6 pagesMeniscus Root Repair RehablangolierNo ratings yet
- Care of Orthopedic Patients With Baker CystsDocument27 pagesCare of Orthopedic Patients With Baker CystsLuayon FrancisNo ratings yet
- Radiology Ordering GuideDocument27 pagesRadiology Ordering GuideRahim Rajab AliNo ratings yet
- Achilles Tendon Injuries: Signs and SymptomsDocument23 pagesAchilles Tendon Injuries: Signs and SymptomsahmadNo ratings yet
- Emergency Ultrasound教學 (8) 急診超音波在深部靜脈栓塞之應用Document40 pagesEmergency Ultrasound教學 (8) 急診超音波在深部靜脈栓塞之應用juice119No ratings yet
- Surgical Treatment of Popliteal Cyst A SystematicDocument9 pagesSurgical Treatment of Popliteal Cyst A SystematicSri KarunNo ratings yet
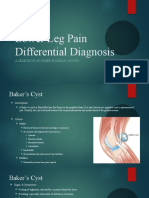
- Lower Leg Pain Differential Diagnosis - OtherDocument13 pagesLower Leg Pain Differential Diagnosis - Otherapi-619359087No ratings yet
- Bakers CystDocument1 pageBakers CystLovadi Emese IldikóNo ratings yet
- Knee OsteoarthritisDocument21 pagesKnee OsteoarthritisSEAN JERIMIAH AGBAYANINo ratings yet
- Case Scenario Osteoarthritis Week 16 GerontologDocument5 pagesCase Scenario Osteoarthritis Week 16 GerontologMary Josette NavarraNo ratings yet
- Arthritis: by DR Samra Tahseen Registrar, Radiology LNHDocument86 pagesArthritis: by DR Samra Tahseen Registrar, Radiology LNHAngelic khanNo ratings yet
- Knee Examination OSCE GuideDocument23 pagesKnee Examination OSCE GuideAaron Nameer Abrar RahmanNo ratings yet
- Best Homeopathic Remedies For Knee PainDocument29 pagesBest Homeopathic Remedies For Knee PainKrish MotupalliNo ratings yet
- Knee PainDocument34 pagesKnee Painmanoj ramlal kandoi100% (1)
- Important MCQs Rheumatology2Document7 pagesImportant MCQs Rheumatology2little luluNo ratings yet
- Baker CystDocument4 pagesBaker CystFitriany LihawaNo ratings yet
- What Is A Baker's Cyst ("Popliteal Cyst") ?Document2 pagesWhat Is A Baker's Cyst ("Popliteal Cyst") ?Faris AzharNo ratings yet