Download as pdf or txt
You might also like
- Community Health Education Methods A Practical Guide PDFDocument2 pagesCommunity Health Education Methods A Practical Guide PDFLaura0% (4)
- Bishop Coulston Roman Military Equipment From The Punic Wars To The Fall of RomeDocument345 pagesBishop Coulston Roman Military Equipment From The Punic Wars To The Fall of Romefevzisahin79100% (4)
- Challenges Faced by Entrepreneurs of Sari-Sari Stores in Kabankalan CityDocument40 pagesChallenges Faced by Entrepreneurs of Sari-Sari Stores in Kabankalan CityAyeng 1502100% (2)
- Kolinrergik 1Document14 pagesKolinrergik 1Fitri anaNo ratings yet
- Second Generation Atypical Antipsychotics Olanzapine and Aripiprazole Reduce Expression and Secretion of Inflammatory Cytokines in Human Immune CellsDocument8 pagesSecond Generation Atypical Antipsychotics Olanzapine and Aripiprazole Reduce Expression and Secretion of Inflammatory Cytokines in Human Immune CellsaulyaNo ratings yet
- Asian Journal of Psychiatry: Rati Ranjan Sethy, MD, DPM, Vinod Kumar Sinha, MD, DPMDocument5 pagesAsian Journal of Psychiatry: Rati Ranjan Sethy, MD, DPM, Vinod Kumar Sinha, MD, DPMpatricknuncioNo ratings yet
- The Investigation of Leptin and Hypothalamic Neuropeptides Role in First Attack Psychotic Male Patients: Olanzapine MonotherapyDocument7 pagesThe Investigation of Leptin and Hypothalamic Neuropeptides Role in First Attack Psychotic Male Patients: Olanzapine MonotherapyCansu UnsalNo ratings yet
- Serum Interleukin-6 Is A Predictive Biomarker For Ketamine's Antidepressant Effect in Treatment-Resistant Patients With Major DepressionDocument3 pagesSerum Interleukin-6 Is A Predictive Biomarker For Ketamine's Antidepressant Effect in Treatment-Resistant Patients With Major DepressionAlex AlexNo ratings yet
- ArabeDocument9 pagesArabePablo Maldonado MuñozNo ratings yet
- E Cacy of Modern Antipsychotics in Placebo-Controlled Trials in Bipolar Depression: A Meta-AnalysisDocument10 pagesE Cacy of Modern Antipsychotics in Placebo-Controlled Trials in Bipolar Depression: A Meta-AnalysisRisda AprilianiNo ratings yet
- Lit Review Junior YearDocument4 pagesLit Review Junior Yearapi-403958599No ratings yet
- Short-Term and Long-Term Evaluation of Selective Serotonin Reuptake Inhibitors in The Treatment of Panic Disorder: Fluoxetine Vs CitalopramDocument6 pagesShort-Term and Long-Term Evaluation of Selective Serotonin Reuptake Inhibitors in The Treatment of Panic Disorder: Fluoxetine Vs CitalopramBakhita MaryamNo ratings yet
- NIH Public Access: Neuroscience To Clinical PsychopharmacologyDocument22 pagesNIH Public Access: Neuroscience To Clinical PsychopharmacologysamarqandiNo ratings yet
- Neuroendocrine Derangement in Chronic Migraine (Pages 1309-1310)Document2 pagesNeuroendocrine Derangement in Chronic Migraine (Pages 1309-1310)Massio MaxNo ratings yet
- Comparison Between Clozapine, An Atypical Antipsychotic Agent and Haloperidol, A Conventional Agent Used To Treat SchizophreniaDocument6 pagesComparison Between Clozapine, An Atypical Antipsychotic Agent and Haloperidol, A Conventional Agent Used To Treat SchizophreniaLonkesNo ratings yet
- Psychiatric Safety of Ketamine in Psychopharmacology ResearchDocument9 pagesPsychiatric Safety of Ketamine in Psychopharmacology ResearchIftach HuebnerNo ratings yet
- Yan and Kreek 2018 Alcohol StressDocument12 pagesYan and Kreek 2018 Alcohol StressChon-wa CheongNo ratings yet
- How Do Psychoactive Drugs WorkDocument1 pageHow Do Psychoactive Drugs WorkErasmus CudjoeNo ratings yet
- Paper 23Document7 pagesPaper 23ramadhaniputrirezkiNo ratings yet
- Association of CRHR1 and CRHR2 With Major Depressive Disorder and Panic Disorder in A Japanese PopulationDocument8 pagesAssociation of CRHR1 and CRHR2 With Major Depressive Disorder and Panic Disorder in A Japanese PopulationNazihan Safitri AlkatiriNo ratings yet
- Translational and Reverse Translational Research On The Role of Stress in Drug Craving and RelapseDocument14 pagesTranslational and Reverse Translational Research On The Role of Stress in Drug Craving and Relapsemanan joshiNo ratings yet
- Muscarinic Cholinergic Receptor Agonist and Peripheral Antagonist For Schizophrenia (2021)Document10 pagesMuscarinic Cholinergic Receptor Agonist and Peripheral Antagonist For Schizophrenia (2021)ShadeLRKNo ratings yet
- Effects of Quetiapine On DNA Methylation in Neuroblastoma CellsDocument5 pagesEffects of Quetiapine On DNA Methylation in Neuroblastoma CellsafpiovesanNo ratings yet
- 1 s2.0 S0028390816301617 MainDocument11 pages1 s2.0 S0028390816301617 Mainshayley9No ratings yet
- Crystal MethDocument12 pagesCrystal MethrezkiNo ratings yet
- Unraveling Depression in Parkinsonõs Disease: EditorialDocument3 pagesUnraveling Depression in Parkinsonõs Disease: Editorialemilyball100% (1)
- Algorithm-Based Pharmacotherapy For First-Episode Schizophrenia Involuntarily Hospitalized: A Retrospective Analysis of Real-World PracticeDocument8 pagesAlgorithm-Based Pharmacotherapy For First-Episode Schizophrenia Involuntarily Hospitalized: A Retrospective Analysis of Real-World PracticerischaNo ratings yet
- NMDA Receptor Antagonist Effects, Cortical Glutamatergic Function, and Schizophrenia: Toward A Paradigm Shift in Medication DevelopmentDocument19 pagesNMDA Receptor Antagonist Effects, Cortical Glutamatergic Function, and Schizophrenia: Toward A Paradigm Shift in Medication DevelopmentCortate15gNo ratings yet
- Sparrow 2012Document13 pagesSparrow 2012Elisa RodríguezNo ratings yet
- Common and Distinct Neural Effects of Risperidone and Olanzapine During Procedural Learning in Schizophrenia: A Randomised Longitudinal fMRI StudyDocument11 pagesCommon and Distinct Neural Effects of Risperidone and Olanzapine During Procedural Learning in Schizophrenia: A Randomised Longitudinal fMRI StudyIntan Sari UmarNo ratings yet
- Brain, Behavior, and ImmunityDocument8 pagesBrain, Behavior, and ImmunityjioosfNo ratings yet
- Psychiatry Research: Ahmad Ghanizadeh, Zahra Rezaee, Sara Dehbozorgi, Michael Berk, Shahin AkhondzadehDocument3 pagesPsychiatry Research: Ahmad Ghanizadeh, Zahra Rezaee, Sara Dehbozorgi, Michael Berk, Shahin AkhondzadehArdi AsNo ratings yet
- Delusional Disorder: Molecular Genetic Evidence For Dopamine PsychosisDocument8 pagesDelusional Disorder: Molecular Genetic Evidence For Dopamine PsychosisRadina RusevaNo ratings yet
- Evidence-Based Guideline: Treatment of Painful Diabetic NeuropathyDocument11 pagesEvidence-Based Guideline: Treatment of Painful Diabetic NeuropathyTriNo ratings yet
- tmp9C7B TMPDocument12 pagestmp9C7B TMPFrontiersNo ratings yet
- 6578 FullDocument12 pages6578 Fullシン イNo ratings yet
- Accepted ManuscriptDocument18 pagesAccepted Manuscriptadriana.minouNo ratings yet
- Relation Between Sexual Dysfunctions and Epilepsy, Type of Epilepsy, Type of Antiepileptic Drugs: A Prospective StudyDocument5 pagesRelation Between Sexual Dysfunctions and Epilepsy, Type of Epilepsy, Type of Antiepileptic Drugs: A Prospective StudyPriska CrisnandaNo ratings yet
- RACK1 and Brain-Derived Neurotrophic Factor: A Homeostatic Pathway That Regulates Alcohol AddictionDocument11 pagesRACK1 and Brain-Derived Neurotrophic Factor: A Homeostatic Pathway That Regulates Alcohol Addictionsupraja.bommalaNo ratings yet
- 1 s2.0 S0006322397002953nlnl Nnnmain PDFDocument3 pages1 s2.0 S0006322397002953nlnl Nnnmain PDFElisa SalakayNo ratings yet
- Anp. Anxiety - EnglDocument5 pagesAnp. Anxiety - Englarif mujionoNo ratings yet
- Wearing Off ParkinsonDocument6 pagesWearing Off ParkinsonYunita Christiani BiyangNo ratings yet
- H1 Histamine Receptor Affinity Predicts Short Term Weight Gain For Typical and Atypical Antipsychotic DrugsDocument9 pagesH1 Histamine Receptor Affinity Predicts Short Term Weight Gain For Typical and Atypical Antipsychotic DrugsLefinia PutriNo ratings yet
- Sanghani2018 - Electroconvulsive Therapy (ECT) in Schizophrenia - A Review of Recent LiteratureDocument10 pagesSanghani2018 - Electroconvulsive Therapy (ECT) in Schizophrenia - A Review of Recent Literatureenfermaria3bhupesNo ratings yet
- Prescribing Antipsychotics in Geriatric Patients:: First of 3 PartsDocument8 pagesPrescribing Antipsychotics in Geriatric Patients:: First of 3 PartsAlexRázuri100% (1)
- Fibro Sistematic Review and Meta OEA AltosDocument12 pagesFibro Sistematic Review and Meta OEA AltosAntonietaValenzuelaMayorgaNo ratings yet
- Urinary Neurotransmitter Analysis As A Biomarker For Psychiatric DisordersDocument3 pagesUrinary Neurotransmitter Analysis As A Biomarker For Psychiatric DisordersPpa Gpat AmitNo ratings yet
- A Systematic Review of The Evidence of Clozapine's Anti-Aggressive EffectsDocument21 pagesA Systematic Review of The Evidence of Clozapine's Anti-Aggressive EffectsDivaNo ratings yet
- HHS Public Access: Association of Antipsychotic Use With Mortality Risk in Patients With Parkinson DiseaseDocument17 pagesHHS Public Access: Association of Antipsychotic Use With Mortality Risk in Patients With Parkinson DiseasekasandraharahapNo ratings yet
- Topiramate For Prevention of Olanzapine Associated Weight Gai - 2010 - SchizophrDocument6 pagesTopiramate For Prevention of Olanzapine Associated Weight Gai - 2010 - SchizophrSol ContrerasNo ratings yet
- HHS Public Access: Early Life Stress and Glutamate Neurotransmission in Major Depressive DisorderDocument17 pagesHHS Public Access: Early Life Stress and Glutamate Neurotransmission in Major Depressive DisorderJpNo ratings yet
- The Effects of Naltrexone On Subjective ResponseDocument10 pagesThe Effects of Naltrexone On Subjective ResponseClarissa Castro RodríguezNo ratings yet
- NPP 2014330 ADocument8 pagesNPP 2014330 ADoc HadiNo ratings yet
- Atypical Antipsychotic Augmentation in Major Depressive DisorderDocument13 pagesAtypical Antipsychotic Augmentation in Major Depressive DisorderrantiNo ratings yet
- Psychotic Decompensation During Nalmefene Treatment in A Patient With Schizoaffective Disorder: A Case ReportDocument5 pagesPsychotic Decompensation During Nalmefene Treatment in A Patient With Schizoaffective Disorder: A Case ReportJauza Raudhatul JannahNo ratings yet
- Naltrexone Treatment For Kleptomania: A Case Report 2: Pınar Çetinay Aydin, Buket Belkiz Güngör, Leyla GülserenDocument3 pagesNaltrexone Treatment For Kleptomania: A Case Report 2: Pınar Çetinay Aydin, Buket Belkiz Güngör, Leyla GülserennurulamaliahNo ratings yet
- 1 s2.0 S0278584622000549 MainDocument13 pages1 s2.0 S0278584622000549 MainGregory AssonitisNo ratings yet
- Cannabis Therapeutics and The Future ofDocument11 pagesCannabis Therapeutics and The Future ofRóbson BatistaNo ratings yet
- NIH Public AccessDocument18 pagesNIH Public AccessMiko FernandezNo ratings yet
- Out Come FactorsDocument9 pagesOut Come FactorsSatrya PermanaNo ratings yet
- Caripirazine Compared To Aripiprazole in PCP Induced Attention DeficitsDocument12 pagesCaripirazine Compared To Aripiprazole in PCP Induced Attention DeficitsEsraa SaeedNo ratings yet
- Depresi Dan KankerDocument10 pagesDepresi Dan KankernigoNo ratings yet
- Manuscript Belli EnglishDocument8 pagesManuscript Belli EnglishFachrul HardtopNo ratings yet
- Bullying FactsDocument1 pageBullying FactsFachrul HardtopNo ratings yet
- 2338-Article Text-6184-1-10-20220905Document7 pages2338-Article Text-6184-1-10-20220905Fachrul HardtopNo ratings yet
- Brain Sciences: The Polygenic Nature and Complex Genetic Architecture of Specific Learning DisorderDocument43 pagesBrain Sciences: The Polygenic Nature and Complex Genetic Architecture of Specific Learning DisorderFachrul HardtopNo ratings yet
- RSJD Dr. Amino Gondohutomo, Central Java 347 Brigjend. Sudiarto Street, Semarang City, 50611, IndonesiaDocument18 pagesRSJD Dr. Amino Gondohutomo, Central Java 347 Brigjend. Sudiarto Street, Semarang City, 50611, IndonesiaFachrul HardtopNo ratings yet
- DR Yong Ko PinDocument2 pagesDR Yong Ko PinFachrul HardtopNo ratings yet
- Peranan Visum Et Repertum Psikiatrikum GDocument19 pagesPeranan Visum Et Repertum Psikiatrikum GFachrul HardtopNo ratings yet
- Rekap Peserta WS1Document1 pageRekap Peserta WS1Fachrul HardtopNo ratings yet
- Andreasen1982 SANSDocument5 pagesAndreasen1982 SANSFachrul Hardtop100% (1)
- Internet Gaming Disorder (IGD) A Case Report of Social AnxietyDocument6 pagesInternet Gaming Disorder (IGD) A Case Report of Social AnxietyFachrul HardtopNo ratings yet
- Forenisk LiverDocument6 pagesForenisk LiverFachrul HardtopNo ratings yet
- Involving Patients With Dementia in Decisions To Initiate Treatment: Effect On Patient Acceptance, Satisfaction and Medication PrescriptionDocument2 pagesInvolving Patients With Dementia in Decisions To Initiate Treatment: Effect On Patient Acceptance, Satisfaction and Medication PrescriptionFachrul HardtopNo ratings yet
- Continental Device India Limited: Silicon Epitaxial TransistorDocument3 pagesContinental Device India Limited: Silicon Epitaxial TransistorRaymundo Moran LopezNo ratings yet
- UTS 013 CaseStudies HasbahDigital v1.0 MEDocument2 pagesUTS 013 CaseStudies HasbahDigital v1.0 METhomas ThomasNo ratings yet
- Classification of HotelsDocument14 pagesClassification of HotelsJeevesh ViswambharanNo ratings yet
- CHEMISTRY, NEET CRASH COURSE LEACTURE PLAN - Neet Crash Course ChemistryDocument2 pagesCHEMISTRY, NEET CRASH COURSE LEACTURE PLAN - Neet Crash Course ChemistryIsh AnandNo ratings yet
- Io TDocument39 pagesIo TECESPLNo ratings yet
- Comprobante SantanderDocument26 pagesComprobante SantanderCristinaNo ratings yet
- Formaldehyde From Production To Application: November 2013Document17 pagesFormaldehyde From Production To Application: November 2013Mohammed FaiqNo ratings yet
- Vineeta Singh (Final)Document3 pagesVineeta Singh (Final)9304768839No ratings yet
- Balance of Payment - Chapter1 - IED - AssignmentDocument4 pagesBalance of Payment - Chapter1 - IED - Assignmentavika jainNo ratings yet
- 1.1 Nanomaterials and NanoparticlesDocument2 pages1.1 Nanomaterials and NanoparticlesDuyen75% (4)
- Agrirobot PDFDocument103 pagesAgrirobot PDFMuhamad Azlan ShahNo ratings yet
- BU ProspectusDocument40 pagesBU ProspectusVikram YadavNo ratings yet
- Fault Diagnosis of Power Transformer Based On Multi-Layer SVM ClassifierDocument7 pagesFault Diagnosis of Power Transformer Based On Multi-Layer SVM ClassifierFelipe KaewNo ratings yet
- English 4 Q1 WK1Document3 pagesEnglish 4 Q1 WK1Ace B. SilvestreNo ratings yet
- Output 1Document2 pagesOutput 1Atul Singh ChauhanNo ratings yet
- 4.3 - Maintenance Processing V2.0Document14 pages4.3 - Maintenance Processing V2.0ఈశ్వర్ భరణి100% (1)
- Prospective vs. Retrospective Delay Analysis: Rohit Singhal, Shishir Kant & Adarsh KumarDocument10 pagesProspective vs. Retrospective Delay Analysis: Rohit Singhal, Shishir Kant & Adarsh KumarKevin DonNo ratings yet
- EXD2010 EX200: Compact Ex D Electro-Hydraulic Positioning and Monitoring SystemDocument8 pagesEXD2010 EX200: Compact Ex D Electro-Hydraulic Positioning and Monitoring SystemKelvin Anthony OssaiNo ratings yet
- Active and Passive VoiceDocument3 pagesActive and Passive VoiceCray CrayNo ratings yet
- CL3600-2023-Lecture 4-Cell Growth KineticsDocument62 pagesCL3600-2023-Lecture 4-Cell Growth KineticsJodie BakerNo ratings yet
- Analytic Marking Scheme To Assess Students' Oral SkillDocument6 pagesAnalytic Marking Scheme To Assess Students' Oral Skilliin hermiyantoNo ratings yet
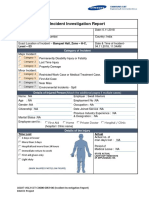
- Incident Investigation Report - Fire Incedent - 04-11-2018 Swati InteriorsDocument4 pagesIncident Investigation Report - Fire Incedent - 04-11-2018 Swati InteriorsMobin Thomas AbrahamNo ratings yet
- Chart Patterns: Symmetrical Triangles The Ascending TriangleDocument8 pagesChart Patterns: Symmetrical Triangles The Ascending TriangleGene Stanley100% (1)
- CAMBODIAN Temple Designs-And Hindu Cosmology-: DR Uday DokrasDocument15 pagesCAMBODIAN Temple Designs-And Hindu Cosmology-: DR Uday DokrasUday DokrasNo ratings yet
- World Population From 1800 To 2100Document19 pagesWorld Population From 1800 To 2100bharatNo ratings yet
- Job Stress QuestionnaireDocument5 pagesJob Stress QuestionnaireRehman KhanNo ratings yet
- Abhishek Shukla Project Reporton (Power Purchase)Document57 pagesAbhishek Shukla Project Reporton (Power Purchase)beast singhNo ratings yet