
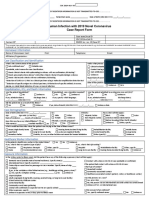
Malaria Case Surveillance Report: Yrs. Mos. Wks. Days (Circle Units)
Malaria Case Surveillance Report: Yrs. Mos. Wks. Days (Circle Units)
You might also like
- Adverse Drug Reaction FormDocument2 pagesAdverse Drug Reaction FormAre Pee Etc0% (1)
- Food Poisoning Investigation Form Version 3 - 0 - 0Document10 pagesFood Poisoning Investigation Form Version 3 - 0 - 0shahanaa AR100% (1)
- Transfer Summary Form Hha To Hospital PDFDocument2 pagesTransfer Summary Form Hha To Hospital PDFsafasayedNo ratings yet
- Healing Trough Humour - Ghazian LuthfiDocument3 pagesHealing Trough Humour - Ghazian Luthfighazian luthfiNo ratings yet
- CDC Covid-19 Report FormDocument2 pagesCDC Covid-19 Report FormiggybauNo ratings yet
- Human Infection With 2019 Novel Coronavirus Case Report FormDocument2 pagesHuman Infection With 2019 Novel Coronavirus Case Report FormRicardo F. BernardinelliNo ratings yet
- ReportForm TyphoidDocument2 pagesReportForm TyphoidSundarajan ManiNo ratings yet
- 11 Trauma Emergency Form 19102023Document2 pages11 Trauma Emergency Form 19102023Marjorie BricenioNo ratings yet
- HAEP CaseReport FormDocument1 pageHAEP CaseReport Formkaleem durraniNo ratings yet
- Viral Haemorrhagic Fever - Case Investigation Form: Date of Detection of The Case Case IDDocument3 pagesViral Haemorrhagic Fever - Case Investigation Form: Date of Detection of The Case Case IDSalihu MustaphaNo ratings yet
- NursereportDocument1 pageNursereportcodenurse95No ratings yet
- CT Screening FormDocument1 pageCT Screening FormJuliano PachecoNo ratings yet
- Barangay Assisted Booking Form: CODE: D1ADocument4 pagesBarangay Assisted Booking Form: CODE: D1AChristine May CagaraNo ratings yet
- Graduate PDFDocument2 pagesGraduate PDFTrieu LeNo ratings yet
- My Personal Health RecordDocument2 pagesMy Personal Health RecordKimmi Joy BakerNo ratings yet
- Enrolment FormDocument2 pagesEnrolment FormHiy GisingNo ratings yet
- ADR Form PDFDocument1 pageADR Form PDFChatie PipitNo ratings yet
- Typhoid Fever: Administrative DemographicsDocument6 pagesTyphoid Fever: Administrative DemographicsMohan ChikkalaNo ratings yet
- IDCAP Clinical Assessment ToolsDocument4 pagesIDCAP Clinical Assessment ToolsIDCAP2011100% (1)
- Medical and Medication HistoryDocument19 pagesMedical and Medication HistoryV NNo ratings yet
- ResultDocument8 pagesResultV NNo ratings yet
- General Data: Hannei Lei C. Ung Batch CerebraDocument9 pagesGeneral Data: Hannei Lei C. Ung Batch CerebraEloiza Jean CustodioNo ratings yet
- Pui FormDocument2 pagesPui FormBotez ElviraNo ratings yet
- Obstetrics History General DataDocument7 pagesObstetrics History General DataColeen NeyraNo ratings yet
- Health Screening and Assessment Form - SampleDocument3 pagesHealth Screening and Assessment Form - SampleRhu1 San Ildefonso100% (1)
- Malaria Identification and Counseling FormDocument1 pageMalaria Identification and Counseling FormTewodros TafereNo ratings yet
- Canine Brucellosis Case ReportDocument1 pageCanine Brucellosis Case ReportOktavia firnandaNo ratings yet
- Uganda HCT Client CardDocument2 pagesUganda HCT Client Cardelmore kakaNo ratings yet
- Oil and Natural Gas Corporation LTD Self Declaration On Medical StatusDocument4 pagesOil and Natural Gas Corporation LTD Self Declaration On Medical StatusDodiya NikunjNo ratings yet
- ANTENATAL Assessment FINALDocument12 pagesANTENATAL Assessment FINALM. jehovah Nissie YeshalomeNo ratings yet
- Birla Institute of Technology & Science, Pilani (Rajasthan)Document1 pageBirla Institute of Technology & Science, Pilani (Rajasthan)saminafirojNo ratings yet
- Adult HIV Confidential Case Report FormDocument4 pagesAdult HIV Confidential Case Report FormilyaskureshiNo ratings yet
- Medical Health RecordDocument1 pageMedical Health RecordNikay SerdeñaNo ratings yet
- Epilepsyquestionnaire 2Document2 pagesEpilepsyquestionnaire 2Sana KhanNo ratings yet
- CDC Data Collection Long FormDocument13 pagesCDC Data Collection Long FormBanzai Health Private LimitedNo ratings yet
- Medical Certificate of Fitness: To Be Filled by CandidateDocument2 pagesMedical Certificate of Fitness: To Be Filled by CandidatevenkatNo ratings yet
- CIF-MR 2022 Ver1Document2 pagesCIF-MR 2022 Ver1Ivy marie BonNo ratings yet
- 130 Physicians-Report 7-21-2023Document2 pages130 Physicians-Report 7-21-2023medisnadaNo ratings yet
- ANSAT CC - Nursing Assessment - Meeting The Care Needs of A Client-PatientDocument5 pagesANSAT CC - Nursing Assessment - Meeting The Care Needs of A Client-PatientjackydoodsonNo ratings yet
- Neuropreceptorial ChecklistDocument33 pagesNeuropreceptorial ChecklistAlloiBialba0% (1)
- Georgia College and State University School of Nursing Episodic DocumentDocument10 pagesGeorgia College and State University School of Nursing Episodic Documentapi-310557802No ratings yet
- Cullman Regional Community Vaccination Clinic Waitlist FormDocument1 pageCullman Regional Community Vaccination Clinic Waitlist FormFOX54 News HuntsvilleNo ratings yet
- Community Covid-19 Registration Form: Medical ConditionsDocument1 pageCommunity Covid-19 Registration Form: Medical ConditionsTheCullmanTribuneNo ratings yet
- Medical Certificate of Fitness: Section 1: Candidate's Personal DetailsDocument2 pagesMedical Certificate of Fitness: Section 1: Candidate's Personal DetailsSwastik Trading AgenciesNo ratings yet
- Revised Case Report Form For Confirmed Novel Coronavirus COVID-19 (Report To WHO Within 48 Hours of Case Identification)Document3 pagesRevised Case Report Form For Confirmed Novel Coronavirus COVID-19 (Report To WHO Within 48 Hours of Case Identification)Lindo Gondales Jr.No ratings yet
- Confidential Report On Adverse Drug Experience: (Mmm/dd/yyyy)Document1 pageConfidential Report On Adverse Drug Experience: (Mmm/dd/yyyy)Jorge ReyesNo ratings yet
- Patient Registration Form 29Document8 pagesPatient Registration Form 29Cahayastore CahayastoreNo ratings yet
- Annex A1: Print Legibly. Mark Appropriate Boxes C With " "Document6 pagesAnnex A1: Print Legibly. Mark Appropriate Boxes C With " "Chum ChitaruNo ratings yet
- Surgery Admission 2014Document2 pagesSurgery Admission 2014Lisa VaughnNo ratings yet
- GM - FORMATO SINIESTROS - Medical ReportDocument5 pagesGM - FORMATO SINIESTROS - Medical ReportRicardo CadenaNo ratings yet
- Annex A1: Print Legibly. Mark Appropriate Boxes C With " "Document21 pagesAnnex A1: Print Legibly. Mark Appropriate Boxes C With " "allen zacariasNo ratings yet
- Medical Form For Grade 7 12Document3 pagesMedical Form For Grade 7 12Deonna Angeline100% (1)
- MedWard Checklist 1 - 2Document10 pagesMedWard Checklist 1 - 2Karess AvilloNo ratings yet
- Viral Hemorrhagic Fever VHF Case ProformaDocument1 pageViral Hemorrhagic Fever VHF Case ProformaDr Sarimul Hoque MazumderNo ratings yet
- AUC Health ClearanceDocument2 pagesAUC Health ClearanceNatasha ReddyNo ratings yet
- Patient Information Form 2017Document1 pagePatient Information Form 2017Merabo SimonishviliNo ratings yet
- Apta Eval-Fax Version Asapt 2007Document4 pagesApta Eval-Fax Version Asapt 2007Abdur RasyidNo ratings yet
- History and Physical ExaminationDocument4 pagesHistory and Physical ExaminationVernonDimalNo ratings yet
- One Step Med: General Medical Information Record Keeping ManualFrom EverandOne Step Med: General Medical Information Record Keeping ManualNo ratings yet
- Physician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideFrom EverandPhysician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideNo ratings yet
- CHCDIS007 STUDENT WORKBOOK (WORD) (C3) .v1.1Document60 pagesCHCDIS007 STUDENT WORKBOOK (WORD) (C3) .v1.1Elsa Miriam Binoy100% (4)
- 04-25-13 EditionDocument36 pages04-25-13 EditionSan Mateo Daily JournalNo ratings yet
- 7 Natural Cures For Today Most Common Health ProblemsDocument10 pages7 Natural Cures For Today Most Common Health Problemsnicolas0danekNo ratings yet
- Parse's Theory of Human BecomingDocument16 pagesParse's Theory of Human Becomingprincess anneNo ratings yet
- Pharmacokinetic&Pharmacodynamics Mivacurium in Young Adult and Elderly PatientDocument8 pagesPharmacokinetic&Pharmacodynamics Mivacurium in Young Adult and Elderly PatientIndah PrihandiniNo ratings yet
- Beast Mentality E-BookDocument40 pagesBeast Mentality E-BookMilton DesignerNo ratings yet
- CRANIOTOMYDocument5 pagesCRANIOTOMYJesha PlatigueNo ratings yet
- Factors of Care During Pregnancy, ScreeningsDocument38 pagesFactors of Care During Pregnancy, ScreeningssabhyaNo ratings yet
- Isolated Systolic Hypertension in AdultDocument8 pagesIsolated Systolic Hypertension in AdultBkash ShahNo ratings yet
- Vet Radiology Ultrasound - 2011 - Hittmair - RADIOGRAPHIC AND ULTRASONOGRAPHIC DIAGNOSIS OF STENOSING TENOSYNOVITIS OF THEDocument7 pagesVet Radiology Ultrasound - 2011 - Hittmair - RADIOGRAPHIC AND ULTRASONOGRAPHIC DIAGNOSIS OF STENOSING TENOSYNOVITIS OF THECésar Sa JimNo ratings yet
- HCLDocument10 pagesHCLaakritiNo ratings yet
- Thyroid - History Taking: 1. Patient DetailsDocument5 pagesThyroid - History Taking: 1. Patient DetailsNellayappan SivasubramanianNo ratings yet
- Republic of The Philippines Regional Trial Court Branch 26Document5 pagesRepublic of The Philippines Regional Trial Court Branch 26JenMarlon Corpuz AquinoNo ratings yet
- Chapter-1 Edi WowDocument8 pagesChapter-1 Edi WowJanette Cosip GaboNo ratings yet
- Mouth Cancer Research PaperDocument6 pagesMouth Cancer Research Paperqhujvirhf100% (1)
- Approved InstDocument368 pagesApproved InstSatish VermaNo ratings yet
- Cna Resume Template FreeDocument4 pagesCna Resume Template Freeafmrhbpxtgrdme100% (1)
- Spiritual Struggle Healing Spirit Fall 2008 PDFDocument4 pagesSpiritual Struggle Healing Spirit Fall 2008 PDFphone growthNo ratings yet
- Ruptured Appendectomy - Docx 1Document7 pagesRuptured Appendectomy - Docx 1Rachel QuionNo ratings yet
- Pharmacology, Pathology, Genetics: QP Code: BNN203Document1 pagePharmacology, Pathology, Genetics: QP Code: BNN203Mamta KumariNo ratings yet
- SpecificationDocument56 pagesSpecificationIwan Herawan100% (1)
- HDP COVER, FOREWORD and TABLE OF CONTENTSDocument7 pagesHDP COVER, FOREWORD and TABLE OF CONTENTSMiko MiguelNo ratings yet
- 3 - Updated Undertaking For EmployerDocument1 page3 - Updated Undertaking For EmployerRamnuj Orecul SoralcNo ratings yet
- Legal Medicine: The Branch of Medicine That Deals With TheDocument3 pagesLegal Medicine: The Branch of Medicine That Deals With TheEthel Joi Manalac MendozaNo ratings yet
- Role and Responsibility of HSEDocument5 pagesRole and Responsibility of HSErnp2007123100% (2)
- Synopsis-Brain TumourDocument9 pagesSynopsis-Brain TumourKomalNo ratings yet
- Solas 1974 Chapter Ii-2: - Construction - Fire ProtectionDocument15 pagesSolas 1974 Chapter Ii-2: - Construction - Fire ProtectionOladokun Sulaiman Olanrewaju100% (5)
- Practice Test 6: I. Chọn từ có cách phát âm khác với các từ còn lại ở phần gạch chânDocument3 pagesPractice Test 6: I. Chọn từ có cách phát âm khác với các từ còn lại ở phần gạch chânHiếu Nguyễn MinhNo ratings yet
- Lymphocytic LeukemiaDocument6 pagesLymphocytic Leukemiaル シリ100% (1)























































































Download as pdf or txt
You might also like
- Adverse Drug Reaction FormDocument2 pagesAdverse Drug Reaction FormAre Pee Etc0% (1)
- Food Poisoning Investigation Form Version 3 - 0 - 0Document10 pagesFood Poisoning Investigation Form Version 3 - 0 - 0shahanaa AR100% (1)
- Transfer Summary Form Hha To Hospital PDFDocument2 pagesTransfer Summary Form Hha To Hospital PDFsafasayedNo ratings yet
- Healing Trough Humour - Ghazian LuthfiDocument3 pagesHealing Trough Humour - Ghazian Luthfighazian luthfiNo ratings yet
- CDC Covid-19 Report FormDocument2 pagesCDC Covid-19 Report FormiggybauNo ratings yet
- Human Infection With 2019 Novel Coronavirus Case Report FormDocument2 pagesHuman Infection With 2019 Novel Coronavirus Case Report FormRicardo F. BernardinelliNo ratings yet
- ReportForm TyphoidDocument2 pagesReportForm TyphoidSundarajan ManiNo ratings yet
- 11 Trauma Emergency Form 19102023Document2 pages11 Trauma Emergency Form 19102023Marjorie BricenioNo ratings yet
- HAEP CaseReport FormDocument1 pageHAEP CaseReport Formkaleem durraniNo ratings yet
- Viral Haemorrhagic Fever - Case Investigation Form: Date of Detection of The Case Case IDDocument3 pagesViral Haemorrhagic Fever - Case Investigation Form: Date of Detection of The Case Case IDSalihu MustaphaNo ratings yet
- NursereportDocument1 pageNursereportcodenurse95No ratings yet
- CT Screening FormDocument1 pageCT Screening FormJuliano PachecoNo ratings yet
- Barangay Assisted Booking Form: CODE: D1ADocument4 pagesBarangay Assisted Booking Form: CODE: D1AChristine May CagaraNo ratings yet
- Graduate PDFDocument2 pagesGraduate PDFTrieu LeNo ratings yet
- My Personal Health RecordDocument2 pagesMy Personal Health RecordKimmi Joy BakerNo ratings yet
- Enrolment FormDocument2 pagesEnrolment FormHiy GisingNo ratings yet
- ADR Form PDFDocument1 pageADR Form PDFChatie PipitNo ratings yet
- Typhoid Fever: Administrative DemographicsDocument6 pagesTyphoid Fever: Administrative DemographicsMohan ChikkalaNo ratings yet
- IDCAP Clinical Assessment ToolsDocument4 pagesIDCAP Clinical Assessment ToolsIDCAP2011100% (1)
- Medical and Medication HistoryDocument19 pagesMedical and Medication HistoryV NNo ratings yet
- ResultDocument8 pagesResultV NNo ratings yet
- General Data: Hannei Lei C. Ung Batch CerebraDocument9 pagesGeneral Data: Hannei Lei C. Ung Batch CerebraEloiza Jean CustodioNo ratings yet
- Pui FormDocument2 pagesPui FormBotez ElviraNo ratings yet
- Obstetrics History General DataDocument7 pagesObstetrics History General DataColeen NeyraNo ratings yet
- Health Screening and Assessment Form - SampleDocument3 pagesHealth Screening and Assessment Form - SampleRhu1 San Ildefonso100% (1)
- Malaria Identification and Counseling FormDocument1 pageMalaria Identification and Counseling FormTewodros TafereNo ratings yet
- Canine Brucellosis Case ReportDocument1 pageCanine Brucellosis Case ReportOktavia firnandaNo ratings yet
- Uganda HCT Client CardDocument2 pagesUganda HCT Client Cardelmore kakaNo ratings yet
- Oil and Natural Gas Corporation LTD Self Declaration On Medical StatusDocument4 pagesOil and Natural Gas Corporation LTD Self Declaration On Medical StatusDodiya NikunjNo ratings yet
- ANTENATAL Assessment FINALDocument12 pagesANTENATAL Assessment FINALM. jehovah Nissie YeshalomeNo ratings yet
- Birla Institute of Technology & Science, Pilani (Rajasthan)Document1 pageBirla Institute of Technology & Science, Pilani (Rajasthan)saminafirojNo ratings yet
- Adult HIV Confidential Case Report FormDocument4 pagesAdult HIV Confidential Case Report FormilyaskureshiNo ratings yet
- Medical Health RecordDocument1 pageMedical Health RecordNikay SerdeñaNo ratings yet
- Epilepsyquestionnaire 2Document2 pagesEpilepsyquestionnaire 2Sana KhanNo ratings yet
- CDC Data Collection Long FormDocument13 pagesCDC Data Collection Long FormBanzai Health Private LimitedNo ratings yet
- Medical Certificate of Fitness: To Be Filled by CandidateDocument2 pagesMedical Certificate of Fitness: To Be Filled by CandidatevenkatNo ratings yet
- CIF-MR 2022 Ver1Document2 pagesCIF-MR 2022 Ver1Ivy marie BonNo ratings yet
- 130 Physicians-Report 7-21-2023Document2 pages130 Physicians-Report 7-21-2023medisnadaNo ratings yet
- ANSAT CC - Nursing Assessment - Meeting The Care Needs of A Client-PatientDocument5 pagesANSAT CC - Nursing Assessment - Meeting The Care Needs of A Client-PatientjackydoodsonNo ratings yet
- Neuropreceptorial ChecklistDocument33 pagesNeuropreceptorial ChecklistAlloiBialba0% (1)
- Georgia College and State University School of Nursing Episodic DocumentDocument10 pagesGeorgia College and State University School of Nursing Episodic Documentapi-310557802No ratings yet
- Cullman Regional Community Vaccination Clinic Waitlist FormDocument1 pageCullman Regional Community Vaccination Clinic Waitlist FormFOX54 News HuntsvilleNo ratings yet
- Community Covid-19 Registration Form: Medical ConditionsDocument1 pageCommunity Covid-19 Registration Form: Medical ConditionsTheCullmanTribuneNo ratings yet
- Medical Certificate of Fitness: Section 1: Candidate's Personal DetailsDocument2 pagesMedical Certificate of Fitness: Section 1: Candidate's Personal DetailsSwastik Trading AgenciesNo ratings yet
- Revised Case Report Form For Confirmed Novel Coronavirus COVID-19 (Report To WHO Within 48 Hours of Case Identification)Document3 pagesRevised Case Report Form For Confirmed Novel Coronavirus COVID-19 (Report To WHO Within 48 Hours of Case Identification)Lindo Gondales Jr.No ratings yet
- Confidential Report On Adverse Drug Experience: (Mmm/dd/yyyy)Document1 pageConfidential Report On Adverse Drug Experience: (Mmm/dd/yyyy)Jorge ReyesNo ratings yet
- Patient Registration Form 29Document8 pagesPatient Registration Form 29Cahayastore CahayastoreNo ratings yet
- Annex A1: Print Legibly. Mark Appropriate Boxes C With " "Document6 pagesAnnex A1: Print Legibly. Mark Appropriate Boxes C With " "Chum ChitaruNo ratings yet
- Surgery Admission 2014Document2 pagesSurgery Admission 2014Lisa VaughnNo ratings yet
- GM - FORMATO SINIESTROS - Medical ReportDocument5 pagesGM - FORMATO SINIESTROS - Medical ReportRicardo CadenaNo ratings yet
- Annex A1: Print Legibly. Mark Appropriate Boxes C With " "Document21 pagesAnnex A1: Print Legibly. Mark Appropriate Boxes C With " "allen zacariasNo ratings yet
- Medical Form For Grade 7 12Document3 pagesMedical Form For Grade 7 12Deonna Angeline100% (1)
- MedWard Checklist 1 - 2Document10 pagesMedWard Checklist 1 - 2Karess AvilloNo ratings yet
- Viral Hemorrhagic Fever VHF Case ProformaDocument1 pageViral Hemorrhagic Fever VHF Case ProformaDr Sarimul Hoque MazumderNo ratings yet
- AUC Health ClearanceDocument2 pagesAUC Health ClearanceNatasha ReddyNo ratings yet
- Patient Information Form 2017Document1 pagePatient Information Form 2017Merabo SimonishviliNo ratings yet
- Apta Eval-Fax Version Asapt 2007Document4 pagesApta Eval-Fax Version Asapt 2007Abdur RasyidNo ratings yet
- History and Physical ExaminationDocument4 pagesHistory and Physical ExaminationVernonDimalNo ratings yet
- One Step Med: General Medical Information Record Keeping ManualFrom EverandOne Step Med: General Medical Information Record Keeping ManualNo ratings yet
- Physician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideFrom EverandPhysician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideNo ratings yet
- CHCDIS007 STUDENT WORKBOOK (WORD) (C3) .v1.1Document60 pagesCHCDIS007 STUDENT WORKBOOK (WORD) (C3) .v1.1Elsa Miriam Binoy100% (4)
- 04-25-13 EditionDocument36 pages04-25-13 EditionSan Mateo Daily JournalNo ratings yet
- 7 Natural Cures For Today Most Common Health ProblemsDocument10 pages7 Natural Cures For Today Most Common Health Problemsnicolas0danekNo ratings yet
- Parse's Theory of Human BecomingDocument16 pagesParse's Theory of Human Becomingprincess anneNo ratings yet
- Pharmacokinetic&Pharmacodynamics Mivacurium in Young Adult and Elderly PatientDocument8 pagesPharmacokinetic&Pharmacodynamics Mivacurium in Young Adult and Elderly PatientIndah PrihandiniNo ratings yet
- Beast Mentality E-BookDocument40 pagesBeast Mentality E-BookMilton DesignerNo ratings yet
- CRANIOTOMYDocument5 pagesCRANIOTOMYJesha PlatigueNo ratings yet
- Factors of Care During Pregnancy, ScreeningsDocument38 pagesFactors of Care During Pregnancy, ScreeningssabhyaNo ratings yet
- Isolated Systolic Hypertension in AdultDocument8 pagesIsolated Systolic Hypertension in AdultBkash ShahNo ratings yet
- Vet Radiology Ultrasound - 2011 - Hittmair - RADIOGRAPHIC AND ULTRASONOGRAPHIC DIAGNOSIS OF STENOSING TENOSYNOVITIS OF THEDocument7 pagesVet Radiology Ultrasound - 2011 - Hittmair - RADIOGRAPHIC AND ULTRASONOGRAPHIC DIAGNOSIS OF STENOSING TENOSYNOVITIS OF THECésar Sa JimNo ratings yet
- HCLDocument10 pagesHCLaakritiNo ratings yet
- Thyroid - History Taking: 1. Patient DetailsDocument5 pagesThyroid - History Taking: 1. Patient DetailsNellayappan SivasubramanianNo ratings yet
- Republic of The Philippines Regional Trial Court Branch 26Document5 pagesRepublic of The Philippines Regional Trial Court Branch 26JenMarlon Corpuz AquinoNo ratings yet
- Chapter-1 Edi WowDocument8 pagesChapter-1 Edi WowJanette Cosip GaboNo ratings yet
- Mouth Cancer Research PaperDocument6 pagesMouth Cancer Research Paperqhujvirhf100% (1)
- Approved InstDocument368 pagesApproved InstSatish VermaNo ratings yet
- Cna Resume Template FreeDocument4 pagesCna Resume Template Freeafmrhbpxtgrdme100% (1)
- Spiritual Struggle Healing Spirit Fall 2008 PDFDocument4 pagesSpiritual Struggle Healing Spirit Fall 2008 PDFphone growthNo ratings yet
- Ruptured Appendectomy - Docx 1Document7 pagesRuptured Appendectomy - Docx 1Rachel QuionNo ratings yet
- Pharmacology, Pathology, Genetics: QP Code: BNN203Document1 pagePharmacology, Pathology, Genetics: QP Code: BNN203Mamta KumariNo ratings yet
- SpecificationDocument56 pagesSpecificationIwan Herawan100% (1)
- HDP COVER, FOREWORD and TABLE OF CONTENTSDocument7 pagesHDP COVER, FOREWORD and TABLE OF CONTENTSMiko MiguelNo ratings yet
- 3 - Updated Undertaking For EmployerDocument1 page3 - Updated Undertaking For EmployerRamnuj Orecul SoralcNo ratings yet
- Legal Medicine: The Branch of Medicine That Deals With TheDocument3 pagesLegal Medicine: The Branch of Medicine That Deals With TheEthel Joi Manalac MendozaNo ratings yet
- Role and Responsibility of HSEDocument5 pagesRole and Responsibility of HSErnp2007123100% (2)
- Synopsis-Brain TumourDocument9 pagesSynopsis-Brain TumourKomalNo ratings yet
- Solas 1974 Chapter Ii-2: - Construction - Fire ProtectionDocument15 pagesSolas 1974 Chapter Ii-2: - Construction - Fire ProtectionOladokun Sulaiman Olanrewaju100% (5)
- Practice Test 6: I. Chọn từ có cách phát âm khác với các từ còn lại ở phần gạch chânDocument3 pagesPractice Test 6: I. Chọn từ có cách phát âm khác với các từ còn lại ở phần gạch chânHiếu Nguyễn MinhNo ratings yet
- Lymphocytic LeukemiaDocument6 pagesLymphocytic Leukemiaル シリ100% (1)