Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 7 Weird Tips To Boost Your TestosteroneDocument22 pages7 Weird Tips To Boost Your Testosteronekyo4life67% (3)
- ObstetricsDocument92 pagesObstetricsMARK ARTHUR MARTINEZ100% (1)
- Students For Life of America 2017 - 2018 Annual ReportDocument17 pagesStudents For Life of America 2017 - 2018 Annual ReportStudentsforlifeHQ100% (2)
- Price List Kit Apd Solida: 2-June-2020Document1 pagePrice List Kit Apd Solida: 2-June-2020Bodat BodatsNo ratings yet
- Comprehensive Geriatric AssessmentDocument75 pagesComprehensive Geriatric AssessmentBodat BodatsNo ratings yet
- Bluestone1998 PDFDocument17 pagesBluestone1998 PDFBodat BodatsNo ratings yet
- Ridgway 2019Document8 pagesRidgway 2019Bodat BodatsNo ratings yet
- 11111Document7 pages11111Bodat BodatsNo ratings yet
- Review of Aetiology and Management of Testicular Abscess and Case Reports On Testicle Sparing Management of Testicular AbscessDocument5 pagesReview of Aetiology and Management of Testicular Abscess and Case Reports On Testicle Sparing Management of Testicular AbscessBodat BodatsNo ratings yet
- Unipolar Depressive Disorders: Key PointsDocument7 pagesUnipolar Depressive Disorders: Key PointsBodat BodatsNo ratings yet
- Promoting Sexual and Reproductive Health in Early Adolescence in South Africa and Tanzania: Development of A Theory-And Evidence-Based Intervention ProgrammeDocument10 pagesPromoting Sexual and Reproductive Health in Early Adolescence in South Africa and Tanzania: Development of A Theory-And Evidence-Based Intervention ProgrammeBodat BodatsNo ratings yet
- Pdflib Plop: PDF Linearization, Optimization, Protection Page Inserted by Evaluation VersionDocument9 pagesPdflib Plop: PDF Linearization, Optimization, Protection Page Inserted by Evaluation VersionBodat BodatsNo ratings yet
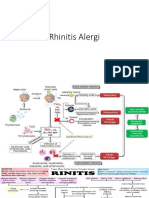
- Rhinitis AlergiDocument22 pagesRhinitis AlergiBodat BodatsNo ratings yet
- Antepartum Haemorrhage: ReviewDocument6 pagesAntepartum Haemorrhage: ReviewBodat BodatsNo ratings yet
- The Connection Between Attachment and SexualityDocument8 pagesThe Connection Between Attachment and SexualityAnca Nicolae100% (1)
- 23011214560126@70 - Pichay, Loren Sta - Teresa - L230000355933 - 2300013461Document2 pages23011214560126@70 - Pichay, Loren Sta - Teresa - L230000355933 - 2300013461maxor4242No ratings yet
- Skills For Normal Vaginal Delivery NSVD 1Document1 pageSkills For Normal Vaginal Delivery NSVD 1Jewel Ann NuñezNo ratings yet
- Ivf Market in IndiaDocument15 pagesIvf Market in IndiaSunil Tak50% (2)
- NWO Plans Exposed by Insider in 1969Document36 pagesNWO Plans Exposed by Insider in 1969Stig Dragholm100% (3)
- PENGARUH PENGGUNAAN MAGNESIUM SULFATE (MgSO4) SAAT ANTENATAL SEBAGAI NEUROPROTEKTOR BAYI PREMATUR TERHADAP PERKEMBANGAN MOTORIK KASAR USIA 2-3 TAHUNDocument8 pagesPENGARUH PENGGUNAAN MAGNESIUM SULFATE (MgSO4) SAAT ANTENATAL SEBAGAI NEUROPROTEKTOR BAYI PREMATUR TERHADAP PERKEMBANGAN MOTORIK KASAR USIA 2-3 TAHUNAyik AyulanjaniNo ratings yet
- Antenatal Fetal MonitoringDocument51 pagesAntenatal Fetal MonitoringCodillia Cheong100% (2)
- Trias RevisiDocument20 pagesTrias RevisiDion PratamaNo ratings yet
- 3.1.5.3 Patologi Anatomi Sistem Urogenital Dan PayudaraDocument70 pages3.1.5.3 Patologi Anatomi Sistem Urogenital Dan PayudaraaiysahmirzaNo ratings yet
- The Apgar ScoreDocument6 pagesThe Apgar ScoretiuwangNo ratings yet
- Atg Quiz PresentperfectDocument30 pagesAtg Quiz PresentperfectfirstclassNo ratings yet
- G10 Science Q3 - Week 1 - Male Reproductive SystemDocument18 pagesG10 Science Q3 - Week 1 - Male Reproductive SystemKlent CalunsagNo ratings yet
- CP Vs BE en La IATFDocument7 pagesCP Vs BE en La IATFSterlin MorenoNo ratings yet
- Chapter 10 - MeiosisDocument29 pagesChapter 10 - Meiosisnancie8No ratings yet
- Reproductive Hormones and Their FunctionsDocument6 pagesReproductive Hormones and Their FunctionsOwolabi PetersNo ratings yet
- 1.menstrual CycleDocument7 pages1.menstrual CycleAyenachew AyelikNo ratings yet
- 3HIV AIDSWordSearchDocument1 page3HIV AIDSWordSearchTimothy William C. LaurenceNo ratings yet
- Benign Lesions of The OvariesDocument12 pagesBenign Lesions of The OvariesdocjosmaNo ratings yet
- Puberty and The Tanner StagesDocument2 pagesPuberty and The Tanner StagesPramedicaPerdanaPutraNo ratings yet
- Film ScriptDocument4 pagesFilm ScriptclinvilNo ratings yet
- Bleeding PregDocument261 pagesBleeding PregElsya ParamitasariNo ratings yet
- Solution Manual For Olds Maternal Newborn Nursing Womens Health Across The Lifespan 9 e 9th Edition 0133073777Document36 pagesSolution Manual For Olds Maternal Newborn Nursing Womens Health Across The Lifespan 9 e 9th Edition 0133073777pourlieustationcc2w7s100% (48)
- Infectious FungiDocument129 pagesInfectious FungiEDWARD MAURICIO GALLO GUALDRÓN100% (4)
- Testical MassageDocument11 pagesTestical MassageRangerItaly100% (1)
- Medico Legal TerminologiesDocument13 pagesMedico Legal TerminologiesMoHiT NaRaYaNNo ratings yet
- Cognitive Dysfunction - Endocrine - KlinefeltersDocument5 pagesCognitive Dysfunction - Endocrine - KlinefeltersBenNo ratings yet
- G-Spots: The Clitoris, A-Spot, G-Spot and U-SpotDocument4 pagesG-Spots: The Clitoris, A-Spot, G-Spot and U-SpotraviikumarNo ratings yet