Download as pdf or txt
You might also like
- Boylan - The Spiritual Life of The PriestDocument63 pagesBoylan - The Spiritual Life of The Priestpablotrollano100% (1)
- Module 2 1 Math 10 Graphs of Polynomial Functions FinalDocument29 pagesModule 2 1 Math 10 Graphs of Polynomial Functions FinalJacob Sanchez100% (1)
- The First 1,000 Days Window of OpportunityDocument6 pagesThe First 1,000 Days Window of OpportunityCar OrdzNo ratings yet
- 2007 FoodNutrBull 375 RoySKDocument9 pages2007 FoodNutrBull 375 RoySKhafsatsaniibrahimmlfNo ratings yet
- 1 s2.0 S2405844022036180 MainDocument7 pages1 s2.0 S2405844022036180 MainSherly AuliaNo ratings yet
- NAH Determinants of Normal Nutrition Among 0-59-Month-Old Filipino Children Living in Low-Income HouseholdsDocument12 pagesNAH Determinants of Normal Nutrition Among 0-59-Month-Old Filipino Children Living in Low-Income Householdsnung09No ratings yet
- The Effectiveness of Community-Based Nutrition Education On The Nutrition Status of Under-Five Children in Developing Countries. A Systematic ReviewDocument4 pagesThe Effectiveness of Community-Based Nutrition Education On The Nutrition Status of Under-Five Children in Developing Countries. A Systematic ReviewDesy rianitaNo ratings yet
- Ajcn 2Fnqz047Document10 pagesAjcn 2Fnqz047agung krisNo ratings yet
- Prebiotic Supplementation Improves Apetite Control in Children With Overweight and Obesity, A Randomized Controlled TrialDocument11 pagesPrebiotic Supplementation Improves Apetite Control in Children With Overweight and Obesity, A Randomized Controlled TrialJUAN SEBASTIAN AVELLANEDA MARTINEZNo ratings yet
- 0379572116651209Document11 pages0379572116651209Desi PuspitasariNo ratings yet
- PCH 35 01 014 PDFDocument10 pagesPCH 35 01 014 PDFDhika Adhi PratamaNo ratings yet
- Nutrition Education Programs Aimed at African Mothers of Infant Children A Systematic ReviewDocument19 pagesNutrition Education Programs Aimed at African Mothers of Infant Children A Systematic ReviewDicky Estosius TariganNo ratings yet
- 10 1093@jn@nxy249Document8 pages10 1093@jn@nxy249Natali PamilanganNo ratings yet
- StuntingDocument9 pagesStuntingAnonymous q8VmTTtmXQNo ratings yet
- The Effectiveness of Nutrition EducationDocument9 pagesThe Effectiveness of Nutrition EducationRika LedyNo ratings yet
- Restrictive Feeding and Excessive Hunger in Young Children With Obesity: A Case SeriesDocument6 pagesRestrictive Feeding and Excessive Hunger in Young Children With Obesity: A Case SeriespingkyNo ratings yet
- Timely Introduction of Complementary Feeding Among Caregivers of Children 612 Month Sodo Town EthiopiaDocument3 pagesTimely Introduction of Complementary Feeding Among Caregivers of Children 612 Month Sodo Town EthiopiaProdi S1- 1BNo ratings yet
- Effectiveness of Nutritional Supplementation During The - 2022 - The Lancet RegDocument11 pagesEffectiveness of Nutritional Supplementation During The - 2022 - The Lancet RegCawee CawNo ratings yet
- Early Obesity Prevention - A Randomized Trial ofDocument7 pagesEarly Obesity Prevention - A Randomized Trial ofClaudia Rodrigues DiasNo ratings yet
- 184-Article Text - 797-1-10-20151013Document5 pages184-Article Text - 797-1-10-20151013Bushra KainaatNo ratings yet
- YCFPDocument8 pagesYCFPMuskan ChadhaNo ratings yet
- A Community-Based Positive Deviance PDFDocument9 pagesA Community-Based Positive Deviance PDFApril ApriliantyNo ratings yet
- Infant Feeding Practices in The Peruvian Amazon: Implications For Programs To Improve FeedingDocument8 pagesInfant Feeding Practices in The Peruvian Amazon: Implications For Programs To Improve FeedingplucichNo ratings yet
- Promoting Responsive Bottle Feeding Within WIC EvDocument13 pagesPromoting Responsive Bottle Feeding Within WIC Evaimane.makerNo ratings yet
- Breast-Feeding Performance Index - A Composite Index To Describe Overall Breast-Feeding Performance Among Infants Under 6 Months of AgeDocument9 pagesBreast-Feeding Performance Index - A Composite Index To Describe Overall Breast-Feeding Performance Among Infants Under 6 Months of AgeHuan VuongNo ratings yet
- Maternal Child Nutrition - 2020 - Maingi - Maternal Knowledge in Complementary Feeding Following Baby Friendly CommunityDocument8 pagesMaternal Child Nutrition - 2020 - Maingi - Maternal Knowledge in Complementary Feeding Following Baby Friendly Communitycherrytale05No ratings yet
- Journal of Nutrition & Food SciencesDocument6 pagesJournal of Nutrition & Food Sciencesfred opinionNo ratings yet
- A Cluster Randomized Trial Determining The Efficacy of Caterpillar Cereal As A Locally Available and Sustainable Complementary Food To Prevent Stunting and AnaemiaDocument8 pagesA Cluster Randomized Trial Determining The Efficacy of Caterpillar Cereal As A Locally Available and Sustainable Complementary Food To Prevent Stunting and AnaemiaAri YulistiNo ratings yet
- Sdarticle 142 PDFDocument1 pageSdarticle 142 PDFRio Michelle CorralesNo ratings yet
- Nzaa 085Document27 pagesNzaa 085Lovely CruzxNo ratings yet
- Parenteral Nutrition in Critically Ill Children: EditorialsDocument3 pagesParenteral Nutrition in Critically Ill Children: EditorialsPrasetya Ismail PermadiNo ratings yet
- 1 s2.0 S2405844021018727 MainDocument6 pages1 s2.0 S2405844021018727 MainainindyaNo ratings yet
- Nutritional Care The Poor Child' of Clinical Cerebral PalsyDocument6 pagesNutritional Care The Poor Child' of Clinical Cerebral Palsycvdk8dc8sbNo ratings yet
- Diarrhea Prevention Through Food Safety EducationDocument4 pagesDiarrhea Prevention Through Food Safety Educationceking99No ratings yet
- Brennan Et Al-2018-Journal of Parenteral and Enteral Nutrition PDFDocument9 pagesBrennan Et Al-2018-Journal of Parenteral and Enteral Nutrition PDFMarilu PachasNo ratings yet
- Nutrition StudDocument7 pagesNutrition StudfeelanNo ratings yet
- Indicaciones NP Onc PedDocument7 pagesIndicaciones NP Onc PedSebastian MarinNo ratings yet
- Journal Pone 0250562Document16 pagesJournal Pone 0250562addanaNo ratings yet
- Grandmothers Knowledge Positively Influences Maternal Knowledge and Infant and Young Child Feeding PracticesDocument10 pagesGrandmothers Knowledge Positively Influences Maternal Knowledge and Infant and Young Child Feeding PracticesAdnan AhmadNo ratings yet
- An Interventional Study To Evaluate The Effectiveness of Selected Nutritional Diet On Growth of Pre Schooler at Selected Slums Area of Bhopal M.PDocument6 pagesAn Interventional Study To Evaluate The Effectiveness of Selected Nutritional Diet On Growth of Pre Schooler at Selected Slums Area of Bhopal M.PEditor IJTSRDNo ratings yet
- Dietary Patterns Exhibit Sex-Specific 3Document9 pagesDietary Patterns Exhibit Sex-Specific 3Luiz Eduardo RodriguezNo ratings yet
- 9B. Effectiveness of Educational Intervention On Breastfeeding Among Primi Pregnant WomanDocument6 pages9B. Effectiveness of Educational Intervention On Breastfeeding Among Primi Pregnant Womanagaua16No ratings yet
- A Responsive Feeding Intervention Increases ChildrDocument7 pagesA Responsive Feeding Intervention Increases Childrandayu nareswariNo ratings yet
- 15-Article Text-14-1-10-20181031 PDFDocument5 pages15-Article Text-14-1-10-20181031 PDFTayyaba RahatNo ratings yet
- Effect of A Ready-To-Use Supplementary Food On The Recovery of Preschool Children With MalnutritionDocument8 pagesEffect of A Ready-To-Use Supplementary Food On The Recovery of Preschool Children With MalnutritionAndres Henry Zegarra LaricoNo ratings yet
- Cooking and Gardening Behaviors and Improvements in Dietary Intake in Hispanic/Latino YouthDocument12 pagesCooking and Gardening Behaviors and Improvements in Dietary Intake in Hispanic/Latino Youthjanileth mejiaNo ratings yet
- The Dietary Intake of Two Groups of Lactating Women in Shanghai During The PuerperiumDocument10 pagesThe Dietary Intake of Two Groups of Lactating Women in Shanghai During The PuerperiumtraphuongNo ratings yet
- Role of Social Support in Improving Infant Feeding Practices in Western Kenya: A Quasi-Experimental StudyDocument18 pagesRole of Social Support in Improving Infant Feeding Practices in Western Kenya: A Quasi-Experimental StudyMhdianaNo ratings yet
- Maternal Knowledge, Attitude, and Practices About Traditional Food Feeding With Stunting and Wasting of Toddlers in Farmer FamiliesDocument7 pagesMaternal Knowledge, Attitude, and Practices About Traditional Food Feeding With Stunting and Wasting of Toddlers in Farmer Familiessarrah salsabilaNo ratings yet
- BMC Public HealthDocument10 pagesBMC Public HealthPam Travezani MiyazakiNo ratings yet
- Adaptation of Content Validity IndexDocument1 pageAdaptation of Content Validity IndexRinda nurulNo ratings yet
- Ajol File Journals - 110 - Articles - 159782 - Submission - Proof - 159782 1309 414936 1 10 20170804Document19 pagesAjol File Journals - 110 - Articles - 159782 - Submission - Proof - 159782 1309 414936 1 10 20170804Uche NjemanzeNo ratings yet
- HKI Case Study ENA NepalDocument2 pagesHKI Case Study ENA NepalkithchetrashchNo ratings yet
- Pengetahuan, Sikap, Motivasi Ibu, Dan Praktik Pemberian MP-ASI Pada Anak Usia 6-23 Bulan: Studi Formatif Di AcehDocument13 pagesPengetahuan, Sikap, Motivasi Ibu, Dan Praktik Pemberian MP-ASI Pada Anak Usia 6-23 Bulan: Studi Formatif Di AcehDesmaria Rohani CitohangNo ratings yet
- A Mixed Method Study Exploring Adherence To and AcDocument12 pagesA Mixed Method Study Exploring Adherence To and AcEvi NurhidayatiNo ratings yet
- 15 Advanced Menu AB 1Document11 pages15 Advanced Menu AB 1Roy CabarlesNo ratings yet
- A Randomized Controlled Trial of Three School Meals Weekend Food Backpacks On Food Security in VirginiaDocument12 pagesA Randomized Controlled Trial of Three School Meals Weekend Food Backpacks On Food Security in VirginiaPrita AnggraeniNo ratings yet
- Randomized Controlled Trial of A Primary Care-Based Child Obesity Prevention Intervention On Infant Feeding PracticesDocument9 pagesRandomized Controlled Trial of A Primary Care-Based Child Obesity Prevention Intervention On Infant Feeding PracticesSardono WidinugrohoNo ratings yet
- 1 Maternal Child Nutrition - 2021 - Martin - Engaging Fathers To Improve Complementary Feeding Is Acceptable and FeasibleDocument14 pages1 Maternal Child Nutrition - 2021 - Martin - Engaging Fathers To Improve Complementary Feeding Is Acceptable and FeasibleKeneniNo ratings yet
- 191572-Article Text-485953-1-10-20191203Document11 pages191572-Article Text-485953-1-10-20191203Abubakar AdanNo ratings yet
- 1 s2.0 S0021755721000991 MainDocument8 pages1 s2.0 S0021755721000991 MainF Gonzales XtlvNo ratings yet
- Global Landscape of Nutrition Challenges in Infants and ChildrenFrom EverandGlobal Landscape of Nutrition Challenges in Infants and ChildrenNo ratings yet
- Tabletop Gaming - Best Games of 2019Document198 pagesTabletop Gaming - Best Games of 2019Paulina Barszez100% (1)
- Benign Ovarian TumorsDocument16 pagesBenign Ovarian TumorsPatNo ratings yet
- Vanilla Icebox CookiesDocument2 pagesVanilla Icebox CookiesmadduxdavidNo ratings yet
- Private Peaceful EssayDocument7 pagesPrivate Peaceful Essayb6zm3pxh100% (2)
- Silver Schmidt Concrete Test Hammer User Manual PDFDocument28 pagesSilver Schmidt Concrete Test Hammer User Manual PDFICIC CALICUT CENTERNo ratings yet
- Draftsmangrade II PDFDocument3 pagesDraftsmangrade II PDFakhilaNo ratings yet
- Physics 158 Final Exam Review Package: UBC Engineering Undergraduate SocietyDocument22 pagesPhysics 158 Final Exam Review Package: UBC Engineering Undergraduate SocietySpam MailNo ratings yet
- Lesson 2 Space in Relation To MovementsDocument7 pagesLesson 2 Space in Relation To MovementsJhanin BuenavistaNo ratings yet
- Class VI Science Chap - 3 TP Solution (Date 19-07-2019)Document3 pagesClass VI Science Chap - 3 TP Solution (Date 19-07-2019)Gopal ShuklaNo ratings yet
- 2sk3673 MosfetDocument4 pages2sk3673 Mosfetagus2kNo ratings yet
- Hazardous Areas - Explosionproof Solenoids: Some HistoryDocument5 pagesHazardous Areas - Explosionproof Solenoids: Some HistoryShahram GhassemiNo ratings yet
- Growth and DevelopmentDocument57 pagesGrowth and DevelopmentKelvin kipkuruiNo ratings yet
- Timken #1 in Comparison Test:: Tapered Roller Bearings Commonly Used in Agricultural-Type EquipmentDocument2 pagesTimken #1 in Comparison Test:: Tapered Roller Bearings Commonly Used in Agricultural-Type Equipmentapi-89480251No ratings yet
- Fashion Through The Decades PowerpointDocument11 pagesFashion Through The Decades PowerpointNigar khanNo ratings yet
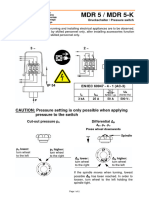
- Pressure Switch MDR5Document4 pagesPressure Switch MDR5Fidelis NdanoNo ratings yet
- 8.7 Measurements Performance Requirements: 8.7.1 Cpich RSCPDocument125 pages8.7 Measurements Performance Requirements: 8.7.1 Cpich RSCPAnthony WeaverNo ratings yet
- Research Report - Aakanksha MistryDocument19 pagesResearch Report - Aakanksha MistryAakanksha MistryNo ratings yet
- CE 1102 Fundamentals of Civil Engineering: Your LecturerDocument36 pagesCE 1102 Fundamentals of Civil Engineering: Your Lecturersaumya irugalbandaraNo ratings yet
- 26 MatricesDocument26 pages26 MatricesFazli KamawalNo ratings yet
- Maryland Route 214 - WikipediaDocument9 pagesMaryland Route 214 - WikipediadwrreNo ratings yet
- Catalogue - Nitoproof 600PFDocument2 pagesCatalogue - Nitoproof 600PFkenneth0129aaNo ratings yet
- Watson InformationDocument17 pagesWatson InformationJorge ForeroNo ratings yet
- Structural Design Report 2017.12.25Document27 pagesStructural Design Report 2017.12.25Gihan ChathurangaNo ratings yet
- IE 411 Lecture6 90ABDocument15 pagesIE 411 Lecture6 90ABZain Ul AbidinNo ratings yet
- Digestibility Evaluation of Fish Meal, Rice Bran, Soya Bean Meal, Pollard On Ongole Cross Breed Cattle and Frisien Holstein Cross BreedDocument7 pagesDigestibility Evaluation of Fish Meal, Rice Bran, Soya Bean Meal, Pollard On Ongole Cross Breed Cattle and Frisien Holstein Cross BreedFailal Ulfi MauliahNo ratings yet
- Continental Drift - WikipediaDocument18 pagesContinental Drift - WikipediaRed EmperadorNo ratings yet
- Information Systems For Sustainable DevelopmentDocument23 pagesInformation Systems For Sustainable DevelopmentnshekhaNo ratings yet