
Initial Medical Management of Patients Severely Irradiated in The Tokai-Mura Criticality Accident (Hirama 2003)
Initial Medical Management of Patients Severely Irradiated in The Tokai-Mura Criticality Accident (Hirama 2003)
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Textbook of Clinical NeuropsychiatryDocument746 pagesTextbook of Clinical Neuropsychiatrymayamanush100% (1)
- Circuit Pulaski Sixtii Division AL Plaintiffs: in The Court County, ArkansasDocument4 pagesCircuit Pulaski Sixtii Division AL Plaintiffs: in The Court County, ArkansasGAPNo ratings yet
- NOV I 0 2020: Order Dismissing AppealDocument2 pagesNOV I 0 2020: Order Dismissing AppealGAPNo ratings yet
- Pathological Changes in The Gastrointestinal Trect of A Heavily Radiation-Exposed Worker at The Tokai-Mura Criticallity Accident (Igaki 2008)Document8 pagesPathological Changes in The Gastrointestinal Trect of A Heavily Radiation-Exposed Worker at The Tokai-Mura Criticallity Accident (Igaki 2008)GAPNo ratings yet
- The Pathology of Multi-Organ Involvement: Two Autopsy Cases From The Tokai-Mura Criticality Accident (Uozaki 2005)Document4 pagesThe Pathology of Multi-Organ Involvement: Two Autopsy Cases From The Tokai-Mura Criticality Accident (Uozaki 2005)GAPNo ratings yet
- Interview Questions 3Document2 pagesInterview Questions 3api-296922357No ratings yet
- Greer Citizen E-Edition 4.26.17Document16 pagesGreer Citizen E-Edition 4.26.17greercitizenNo ratings yet
- Characterization of Clays and Clay Minerals For Industrial ApplicationsDocument184 pagesCharacterization of Clays and Clay Minerals For Industrial Applicationspam2345100% (1)
- Conclusion in BiologyDocument3 pagesConclusion in Biologyadeza azaresNo ratings yet
- Nucmed 7Document33 pagesNucmed 7John Paul MarasiganNo ratings yet
- Change in Measured GFR Vs EGFR CKD OutcomeDocument9 pagesChange in Measured GFR Vs EGFR CKD OutcomeAlizaPinkyNo ratings yet
- Clinical Practice: History SubtypesDocument6 pagesClinical Practice: History SubtypesRafael Alejandro Marín GuzmánNo ratings yet
- Hirschprung Associated EnterocolitisDocument9 pagesHirschprung Associated Enterocolitiskeyla_shineeeNo ratings yet
- Management of HAZCHEM ProcedureDocument35 pagesManagement of HAZCHEM ProcedurechdprNo ratings yet
- Detailed Neurologic Assessment of Infants and Children - UpToDateDocument25 pagesDetailed Neurologic Assessment of Infants and Children - UpToDateLeoberto Batista Pereira SobrinhoNo ratings yet
- Radiobiology DilshadDocument78 pagesRadiobiology DilshadAJAY K VNo ratings yet
- ANSWER Chapter II-Vocabulary ExerciseDocument4 pagesANSWER Chapter II-Vocabulary Exerciseberliana CahyaNo ratings yet
- Tobacco Harm Reduction 2010Document304 pagesTobacco Harm Reduction 2010Billy HadjisNo ratings yet
- 3 Kuliah GERDDocument40 pages3 Kuliah GERDAnonymous vUEDx8No ratings yet
- Aloe Vera: A Potential Herb and Its Medicinal ImportanceDocument25 pagesAloe Vera: A Potential Herb and Its Medicinal ImportanceSusan Sitha Irma YuhanitaNo ratings yet
- Manual de Procesos Quimicos en La Industria George Austin DescargarDocument15 pagesManual de Procesos Quimicos en La Industria George Austin DescargarAmerica Cardenas OntonNo ratings yet
- Iraqi Injury Surveillance System Annual Report 2013Document46 pagesIraqi Injury Surveillance System Annual Report 2013bejarhasanNo ratings yet
- Block - 3 - 2014 Block 3 BookDocument197 pagesBlock - 3 - 2014 Block 3 BookhappyhappylandNo ratings yet
- Jurnal Vertigo Post TraumaDocument5 pagesJurnal Vertigo Post TraumaginapuspaNo ratings yet
- Cosmecueticals Mod1Document35 pagesCosmecueticals Mod1Top 10No ratings yet
- Don Mariano Marcos Memorial State UniversityDocument6 pagesDon Mariano Marcos Memorial State Universitysoledad l. casillaNo ratings yet
- Elekta Infinity™ BrochureDocument12 pagesElekta Infinity™ BrochureDC ShekharNo ratings yet
- Handbook of RadioembolizationDocument349 pagesHandbook of RadioembolizationEdu MassanaNo ratings yet
- Inpatient Rehab LTLD Referral GuidelinesDocument8 pagesInpatient Rehab LTLD Referral GuidelinesAdi Kurnia SandiNo ratings yet
- Chapter 6 Cancer PrepU QuestionsDocument7 pagesChapter 6 Cancer PrepU QuestionsKevin ClarkNo ratings yet
- TahbsoDocument42 pagesTahbsoMarlon RoyoNo ratings yet
- Vocabulary - Health and Health CareDocument10 pagesVocabulary - Health and Health CareDajana RakićNo ratings yet
- Chemical Dependency EvaluationDocument1 pageChemical Dependency EvaluationBekki JonesNo ratings yet
- High-Performance Medicine: The Convergence of Human and Artificial IntelligenceDocument13 pagesHigh-Performance Medicine: The Convergence of Human and Artificial Intelligencefernandoribeirojr98No ratings yet









































































The British Journal of Radiology, 76 (2003), 246–253 E 2003 The British Institute of Radiology
DOI: 10.1259/bjr/82373369
Initial medical management of patients severely irradiated in
the Tokai-mura criticality accident
1
T HIRAMA, MD, PhD, 1S TANOSAKI, MD, PhD, 2S KANDATSU, MD, PhD, 1N KUROIWA, MD,
2
T KAMADA, MD, PhD, 2H TSUJI, MD, PhD, 2S YAMADA, MD, PhD, 2H KATOH, MD, PhD,
2
N YAMAMOTO, MD, PhD, 2H TSUJII, MD, PhD, 3G SUZUKI, MD, PhD and 1M AKASHI, MD, PhD
1
Research Center for Radiation Emergency Medicine, 2Research Center for Charged Particle Therapy, National Institute
of Radiological Sciences, Chiba, Japan and, 3Radiation Effect Research Foundation, Hiroshima, Japan
Abstract. A nuclear criticality accident occurred in Japan on September 30, 1999, which resulted in severe
exposure of three victims to mixed flux of neutrons and c-rays. Estimated average doses for the three victims
were 5.4 Gy of neutrons and 8.5 Gy of c-rays for Patient A, 2.9 Gy of neutrons and 4.5 Gy of c-rays for Patient
B, and 0.81 Gy of neutrons and 1.3 Gy of c-rays for Patient C. They then suffered the consequences of the
effects of ionizing radiation resulting in acute radiation syndrome. In Patients A and B, bone marrow failure
was so severe that they received haematopoietic stem cell transplantation. The graft initially took successfully in
both patients, although in Patient B it was later taken over by his own haematopoietic cells. They also suffered
from severe skin lesions, later exhibited gastrointestinal bleeding and eventually died of multiple organ failure
82 and 210 days after the accident, respectively. The survival of these patients beyond the period of
agranulocytosis means that bone marrow failure per se caused by exposure to ionizing radiation may now be
overcome. Patient C also developed bone marrow failure and was treated with granulocyte colony-stimulating
factor as well as supportive care. He recovered without major complications and is now under periodical follow-
up. Remarkably, during the prodromal phase, all the patients exhibited hypoxaemia, two of whom also showed
interstitial oedema of the lungs. In Patient C these manifestations improved within a week. The circumstances of
the accident and the initial medical treatment of the victims are described.
Since the advent of the nuclear industry, more than 40 Thus, for the survival chance of patients with a severe
accidents associated with nuclear criticality in undesired form of ARS to ever exist, therapeutic intervention to
manners have occurred [1, 2]. Most occurred before 1970, support general physical condition as well as bone marrow
on which our knowledge of the medical outcomes of such failure is of the utmost importance. In contrast, in the
accidents is mainly based. Criticality accidents differ from survivors of previous criticality accidents, radiation-
other types of radiation accidents in that they cause induced skin damage has typically been absent, except
exposure to neutrons and c-rays in quite a short period, localized epilation, and the decrease in leukocytes has been
often a moment, and can be lethal for those within several slower and milder.
metres of the source of radiation, who are often those who In the criticality accident in Tokai-mura, Japan, which
triggered the chain reaction. Those who were in the occurred in 1999, three victims were exposed to high doses
immediate vicinity of the source of radiation exhibit symp- of neutrons and c-rays. Two of the victims exhibited
toms reflecting the severe damaging effects of high-dose extremely severe damage to the bone marrow as well as to
ionizing radiation to many organ systems, such as the bone the skin, which was comparable with a severe form of
marrow, gastrointestinal tract, cardiovascular system and ARS. However, state of the art therapy, including
skin, which are collectively described as a severe form of haematopoietic stem cell transplantation, enabled them
acute radiation syndrome (ARS). Typically, survival terms to survive 82 days and 210 days after the accident,
illustrating that bone marrow failure per se may no
of such patients after a criticality accident have been less
longer be the limiting factor for the survival of such
than 10 days [3, 4]. For instance, in a reported criticality
patients. In the present report, we describe the circum-
accident in 1946 in the United States [5], the victim who
stances in which the victims were irradiated, their medical
was directly handling the critical assembly survived 9 days.
condition and the therapeutic strategy in the initial period.
In another recent criticality accident in Russia, the victim
We also show that arterial blood gas analysis and CT of
survived 66.5 h [6]. Earliest clinical manifestations in such
the chest may be of diagnostic value, at least in criticality
patients, following non-specific prodromal symptoms such accidents, even when the symptoms of ARS are still subtle.
as nausea and vomiting, have been early and severe leuko-
penia and painful oedema of the upper extremities, which
in most cases had been closest to the source of radiation.
Patients and methods
Received 12 November 2001 and in revised form 4 October 2002, Patients
accepted 11 November 2002.
Address correspondence to Toshiyasu Hirama, Research Center for Patients A, B and C, all male, were 35 years old,
Radiation Emergency Medicine, National Institute of Radiological 39 years old and 54 years old, respectively, at the time of
Sciences, 4-9-1 Anagawa, Inage-ku, Chiba 263-8555, Japan. the accident. Disclosure of any information related to
246 The British Journal of Radiology, April 2003
Tokai-mura criticality accident
the patients in this report is based on written informed criticality was triggered, all three workers saw a flash of
consent. blue light. Workers A and B then ran to the next building,
where Worker A collapsed and lost consciousness for some
20 s. He then experienced vomiting and diarrhoea. The
CT stools were not described. Worker C stayed at the scene
for approximately 5 min trying to contact the radiation
CT was performed with a HighSpeed Advantage (GE safety personnel of the facility by telephone. He then
Medical Systems, Milwaukee, WI) scanner. Scans were joined the other two workers. The three workers (hereafter
obtained at end inspiration using 10 mm collimation and referred to as patients) were initially transported to
at 10 mm intervals through the chest, with the patient National Mito Hospital. Because the patients were radioac-
in a supine position. CT was performed at 140 kVp and tive by routine radiological survey and their granulocytosis
200 mAs. and lymphopenia were already marked, physicians of the
hospital readily recognized the severity of the circum-
stances and decided to send the patients to the National
The accident Institute of Radiological Sciences (NIRS) in Chiba, which
A nuclear criticality accident occurred in Tokai-mura, had been assigned, as the hospital in charge of medical
located approximately 120 km northeast of Tokyo. It treatment of victims of radiation accidents in Japan’s Basic
occurred in a company that had been manufacturing Plans for Disaster Prevention. The three patients arrived at
nuclear fuel for power plants in Japan. On September 30, the NIRS at 15:10. While the physicians of the NIRS were
1999, three workers were mixing together seven batches evaluating the medical condition of the patients, our
(2.4 kg uranium per batch) of individually prepared uranyl health physicists and radiation safety staff made radi-
nitrate solution, one of the final steps in the process of ological analyses. Their body surface was significantly
producing 18.8% uranium for an experimental fast reactor radioactive as surveyed by Geiger–Muller survey meter,
in Tokai-mura. Previously they had used a container with but not by alpha survey meter. The vomitus of Patient A
a controlled geometry for this purpose to prevent criti- was analyzed and 24Na detected [7], which is produced by
cality. On that day, however, they decided to mix the neutron activation of stable 23Na and emits b- and c-rays
batches in a larger container, the precipitation tank, of and has been routinely utilized to calculate neutron flux to
which the mass limit to prevent criticality was 2.4 kg estimate doses in previous criticality accidents. It was thus
uranium. At 10:35 am on September 30, when they were known that these were victims of a criticality accident.
pouring the seventh batch of solution into the tank and its
uranium content reached approximately 16 kg, criticality
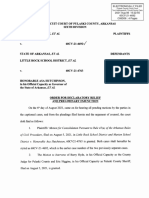
was triggered. The positions and postures of the workers
Evaluation of patients
at the scene were reconstructed by interviewing them Within hours of total body irradiation, radiation acci-
(Figure 1). Worker A, who was the most severely irra- dent victims exhibit symptoms such as nausea, vomiting,
diated, apparently was standing beside and facing the tank diarrhoea, fever and in severe cases, hypotension and even
holding a funnel with at least his right hand. Worker B, loss of consciousness, which might reflect an acute
who was also severely irradiated, was crouching on a stage response of the neurovascular system [8]. Although none
with his right foot on a stair, pouring the solution from a of these symptoms are specific for ARS, collectively their
bucket into the tank, with his face and right hand very promptness and severity have been described to reflect the
close to the tank. Worker C, who was less severely extent of damage that the body had received from ionizing
irradiated, was sitting at his desk a few metres away from radiation and have often been compatible with the dose of
the tank separated by a thin wall. At the moment that radiation estimated by physical methods [9]. Therefore, we
carefully observed the initial symptoms and physical signs
of the patients to get a rough picture of the severity of the
effect of irradiation and thereby formulate reasonable
therapeutic strategies [10].
Patient A experienced nausea, vomiting and a transient
loss of consciousness minutes after the exposure, and
diarrhoea within 1 h. The type of stools at the accident
scene was not reported, but during his 3-day admission at
the NIRS, stools were watery and negative for occult
blood, which meant that the intestinal epithelium was still
intact. On admission, the patient was febrile without any
evidence of infection, slightly drowsy and hypotensive with
a systolic blood pressure of 70 mmHg. The patient also
had diffuse erythema on the ventral body surface, facial
oedema, injection of the conjunctiva bulbi and painful
bilateral parotid swelling. He complained of diffuse
tenderness of the abdominal wall by palpation and dif-
ficulty in voiding. These findings strongly indicated that
the patient had received serious damage from the irra-
Figure 1. The positions and postures of the victims of the diation, comparable with the victims of reported accidents
accident at the moment when criticality was triggered, recon- with fatal outcome.
structed by interviewing Workers B and C. Patient B also experienced nausea and vomiting within
The British Journal of Radiology, April 2003 247
T Hirama, S Tanosaki, S Kandatsu et al
1 h of exposure, but without early diarrhoea. Although agreed fairly well with the above values. Doses based on
Patient B was normotensive on the day of the accident, his the 24Na content in the peripheral blood were 5.4 Gy of
blood pressure was rather low for the next several days neutrons and 8.5 Gy of c-rays for Patient A, 2.9 Gy of
(lowest recorded 80/44 mmHg). The patient was also neutrons and 4.5 Gy of c-rays for Patient B and 0.81 Gy
slightly drowsy, febrile, had erythema on the ventral body of neutrons and 1.3 Gy of c-rays for Patient C 12].
surface and salivary gland swelling, and complained of Chromosome analyses of the patients’ lymphocytes, utili-
mild epigastralgia on admission. These findings indicated zing the prematurely condensed ring method, resulted in
that he would also undergo a severe form of ARS, doses equivalent to c-rays, which were more than 20 GyEq
although to a lesser degree than Patient A. for Patient A, 7.4 GyEq for Patient B and 2.3 GyEq for
Patient C experienced only mild nausea several hours Patient C [13].
after exposure. On admission, his skin had slight but Laboratory analyses revealed several remarkable find-
diffuse erythema. Otherwise, the patient was asymptomatic ings (Table 1a). All three patients showed granulocytosis
and appeared to be in a good physical condition. If we and degrees of lymphocytopenia on the day of the accident
utilize the published table by the International Atomic (day 0). Serum amylase increased after admission and
Energy Agency that correlates symptoms of ARS during peaked on the day following the accident (day 1). It then
its prodromal phase with results of dosimetry, the symp- decreased and, in Patient C, returned to within the normal
toms and signs in Patients A, B and C would correspond range on day 4. Isoenzyme analyses of serum amylase
to the degrees of damage caused by more than 8 Gy, revealed a predominant S-fraction, indicating damage to
between 6 and 8 Gy and less than 4 Gy, respectively, of the salivary glands. Serum uric acid also increased in
ionizing radiation [9]. Patients A and B on day 1. Arterial blood gas was
Lymphocytes represent one of the most sensitive types analyzed in all of them and invariably showed hypox-
of cells to ionizing radiation; the rapidity and extent of the aemia, with partial pressure of oxygen in arterial blood
decrease of lymphocytes are known to correlate with the (PaO2) values of approximately 60 mmHg (Table 1b). In
severity of exposure. Baranov et al have formulated a Patient C, PaO2 gradually improved to 79.8 mmHg by
function between the lymphocyte count and the corre- day 5. Respiratory function was assessed on Patient C
sponding exposure dose in ARS [11]. Although the method and initially revealed a slightly decreased diffusion capa-
can be influenced by the baseline numbers of lymphocytes, city of the lung for carbon monoxide (DLCO) value of
which vary from one individual to another, it provides 13.36 ml min21 mmHg21. The value had returned to normal
information about the severity of ARS in the first when the test was repeated 3 months later. Respiratory
24 h, when the results of dosimetry are typically not yet function was not assessed on Patients A and B because of
available. Because their data were based on c-ray accidents, the impracticality of doing so under reverse isolation.
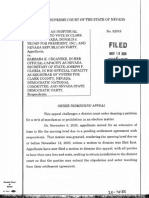
we plotted the patients’ lymphocyte counts in the formula Remarkably, in Patient C, CT of the chest peformed on
and obtained values equivalent to c-rays. The resultant day 1 revealed a crescent-shaped subpleural thickening in
values for Patients A, B and C were more than 10 Grey the dorsum of the lower lobes of the lung, and adjacent
Equivalent (GyEq), between 6 GyEq and 10 GyEq, and reticular shadows in the lung parenchyma, together sug-
between 1 GyEq and 4.5 GyEq, respectively. In Patient A, gesting interstitial oedema of the organ (Figure 3a, arrow).
the lymphocyte counts were far outside the range of In accordance with the improvement of PaO2, a CT
the graph. scan taken on day 6 showed remarkable recovery, with
The results of dosimetric analyses by specialists came only minimal reticular shadows (Figure 3b), which further
2 days after the accident and were refined thereafter. They became almost insignificant on day 60 (Figure 3c). Similar
Table 1. (a) Blood counts and serum chemistry on admission (5.5 h after exposure) to the NIRS. Values marked with an asterisk
are of the following day of the accident. (b) Arterial blood gas analyses on the day of admission. For Patient C, chronological
change is also shown.
a)
Patient Neutrophil (6109 l21) Lymphocyte (6109 l21) Haemoglobin (g l21) Amylase (IU l21) Uric acid (mg l21)
A 24.3 414 165 2143* 112*
B 12.5 268 129 2454* 98*
C 12.2 795 175 1094* 62*
b)
Patient Day pHa PaCO2 (mmHg) PaO2 (mmHg) HCO3 (mmol l21) BE (mmol l21) O2Sat (%)
A 0 7.553 33.9 62.4 29.2 7.0 94.6
B 0 7.574 36.8 55.1 33.3 10.7 92.7
C 0 7.525 42.2 62.6 34.1 10.2 94.0
C 3 7.435 40.5 64.3 26.6 2.2 93.2
C 5 7.402 42.5 79.8 25.9 0.4 95.8
C 13 7.413 45.0 80.8 28.1 2.9 96.0
PaCO2, partial pressure of carbon dioxide in arterial blood; PaO2, partial pressure of oxygen in arterial blood; BE, base excess; O2Sat,
oxygen saturation of arterial blood.
a
Initial pH values show iatrogenic alkalosis, which was caused by an administration of sodium bicarbonate at the National Institute of
Radiological Sciences for the purpose of decorporating uranium that might have been inhaled.
248 The British Journal of Radiology, April 2003
Tokai-mura criticality accident
findings were observed initially in Patient A (Figure 3d). subsequently became tenser. Although the patient con-
Also, in Patient B, mild subpleural thickening was observed tinued to have watery diarrhoea and complained of diffuse
(not shown). abdominal tenderness by palpation, he was apparently well
on days 1 and 2, following which his general condition
rapidly deteriorated. He received peripheral blood stem
Clinical course cell transplantation on days 6 and 7. His progressive
hypoxaemia necessitated endotracheal intubation on day 10.
On admission, Patients A and B were kept under reverse Although the graft took, the patient continued to have
isolation. Initial therapeutic measures that were taken respiratory failure, subsequently exhibited severe skin
common for all three patients included strict maintenance lesion and gastrointestinal bleeding, and died of multiple
of body fluid balance with the infusion of electrolytes and organ failure on day 82. The detail of his therapy has been
plasma under central venous pressure monitoring and published elsewhere [14].
selective digestive tract decontamination with oral admin-
istration of kanamycin sulfate (3 g day21), polymyxin B
(3 000 000 units day21) and amphotericin B (400 mg day21).
Patient B
On day 4, vancomycin was substituted (2 g day21) for
kanamycin. Prophylactic systemic administration of anti- G-CSF (100 mg, intravenous infusion) was started on
biotics (imipenem 1 g day21), antiviral (acyclovir 1 g day21) day 1. This patient also exhibited systemic rash after the
and antifungal (fluconazole 200 mg day21) reagents was infusion, it was decided to administer the growth factor
also started on day 1. Below the clinical picture of each through round the clock infusion from day 2 (500 mg day21).
patient is described separately. Bone marrow aspirates from the sternum and iliac crest on
day 1 were markedly hypocellular with some intranuclear
vacuolations. The myelogram of the smear from the
Patient A sternum was as follows: promyelocyte 0.4%; myelocyte
2.2%; metamyelocyte 2.0%; band 32.4%; segmented 58%;
Granulocyte colony-stimulating factor (G-CSF, 100 mg) eosinophil 1.2%; lymphocyte 2.2%; and phagocyte 1.6%.
was administered intravenously on the evening of day 1. WBC slightly increased on day 2, almost stabilized on
Shortly after it was infused, the patient complained of mild day 3 and then rapidly decreased and almost disappeared
dyspnea and systemic rash. The symptoms resolved after by day 7 (Figure 2a). Lymphocytes also rapidly decreased
inhaled oxygen concentration was increased to 50%. and disappeared on day 7 (Figure 2a). Platelets and hae-
Electrocardiogram was normal on day 1, but evolved moglobin decreased rather gradually (Figure 2a). We
inverted T waves in leads II, III and aVF on day 2, anticipated that Patient B, although obviously having
possibly suggesting damage to the inferior myocardium. been less severely irradiated than Patient A, would suffer
Bone marrow taps were taken from the sternum and iliac at least a prolonged period of severe leukopenia. As the
crest on day 1 and showed marked hypocellularity in both patient may have exhibited severe skin injury and gast-
the erythroid and myeloid lineages (not shown). The rointestinal lesion during that period, we reasoned that it
myelogram of the smear from the sternum was as follows: should be more beneficial than detrimental to support his
myeloblast 1%; promyelocyte 1%; myelocyte 3.6%; meta- leukopenic period with haematopoietic stem cell trans-
myelocyte 4%; band 32.4%; segmented 54.4%; eosinophil plantation. He was transferred to the Institute of Medical
1.4%; monocyte 0.8%; lymphocyte 1%; and plasma cell Science, University of Tokyo, which was another of our
0.2%. Some cells had intranuclear vacuolations, which collaborating hospitals, and received umbilical cord blood
have also been reported in previous accidents [5]. White transplantation on day 9. The graft initially took, and then
blood cells (WBC) of Patient A slightly increased on was gradually replaced by his own haematopoietic cells.
day 2, then rapidly decreased and almost disappeared The patient also had oedema in the right forearm in the
by day 7 (Figure 2a). Later we were informed that he first several days, and later evolved severe skin lesions
had been warned of leukocytosis for at least 2 years. involving the large part of his body surface, in particular
Lymphocytes kept decreasing and disappeared on day 3 the face and extremities. Although the skin lesions were
(Figure 2a). Platelets also decreased steeply, necessitating extensively treated with skin grafts, he later evolved
platelet transfusion starting from day 5 (Figure 2a). gastrointestinal bleeding and infectious complications,
Haemoglobin was rather elevated initially (Table 1a), pos- which caused him to die of multiple organ failure on
sibly reflecting haemoconcentration, but then decreased day 210. The detail of his therapy has been published [15].
rather steeply by day 7 (Figure 2a, lower right panel, dia-
mond) without documented bleeding. From our evaluation
of the severity of his disease based on his symptoms and
Patient C
signs in comparison to the victims of previous accidents
and the preliminary results of dosimetry that we received Judging from Patient C’s symptoms and signs, as well as
on day 2, the spontaneous recovery of the bone marrow of the preliminary results of dosimetry, we expected his bone
Patient A was judged to be quite unlikely. Therefore on marrow to recover spontaneously. Therefore, he remained
day 2 it was decided to treat the patient with haemato- at the hospital of the NIRS and was treated without
poietic stem cell transplantation and to transfer him to the haematopoietic stem cell transplantation. The bone mar-
University of Tokyo Hospital, which was one of our row aspirates from the sternum and iliac crest on day 1
collaborators. G-CSF was discontinued for several days. showed decreased erythroid series and well preserved
While in the NIRS hospital, the patient’s facial oedema myeloid series. The myelogram of the smear from the
slightly improved. However, he complained of painful sternum was as follows: myeloblast 0.4%; promyelocyte
forearm swelling on the right side on day 2, which 2.8%; myelocyte 5.2%; metamyelocyte 4.6%; band 17.3%;
The British Journal of Radiology, April 2003 249
T Hirama, S Tanosaki, S Kandatsu et al
Figure 2. Haematologic data of the patients.
(a) Peripheral blood counts of Patients A, B
and C during the first 11 days are depicted
with diamonds, rectangles and triangles, res-
pectively. (b) Haematologic data of Patient C
during the whole admission period. The
dynamics of neutrophil (upper left), platelet
(middle left), lymphocyte (lower left), haemo-
globin (upper right), reticulocyte (middle
right) and serum iron (lower right) are shown.
segmented 32.6%; eosinophil 3.4%; monocyte 1.8%; recovery (Figure 2a). Haemoglobin slowly decreased
lymphocyte 17.2%; plasma cell 1%; phagocyte 0.4%; baso- from above 150 g l21 to 102 g l21 without any evidence
philic normoblast 1%; polychromatic normoblast 5%; and of bleeding (Figure 2b). Serum iron concentration steeply
orthochromatic normoblast 6.8%. Some morphologically increased from 134 mg dl21 on day 0 to 235 mg dl21 on
abnormal megakaryocytes were also seen (data not day 1, presumably reflecting the halting of erythropoiesis
shown). The patient’s WBC count returned to normal (Figure 2b). It then decreased abruptly in the second
on day 1, then increased in response to G-CSF, which was month, coinciding with the recovery of reticulocytes, which
started on the evening of day 2 (Figure 2a). Neutrophils had decreased during the first week and had then
then started to decrease following a stairwise pattern, and undergone two transient rises (Figure 2b). During admis-
reached a nadir of 1.096109 l21 on day 20 (Figure 2b). sion the patient exhibited spotty epilation as well as
The patient was kept under reverse isolation while having marked diminution in the growth of beard. In addition, he
neutropenia. Following the recovery of the neutrophil had a localized painless defect of the oral mucosa without
count, G-CSF was reduced and eventually discontinued on his knowing, which was pointed out on day 19. The lack
day 28. The decrease in platelets was slower than that of of pain might be attributable to inefficient inflammation
the other two patients (Figure 2a), but necessitated platelet because of the neutropenia that peaked on day 20. These
transfusion on days 17, 20 and 23 (Figure 2b). Platelets symptoms were presumed to have been caused by
made a gradual recovery thereafter. The number of irradiation and improved gradually. He is now being
lymphocytes was lowest on day 2 and also made a slow followed up in the outpatient clinic of the NIRS.
250 The British Journal of Radiology, April 2003
Tokai-mura criticality accident
Figure 3. CT image of the chest of Patients
A and C. Arrows show the relevant areas
stated below. (a) Day 1, Patient C. Note
bilateral subpleural thickening, more severe
in the right side, in the dorsum of the lower
lobes of the lung. Adjacent to the thickening,
restiform or rough reticular shadow can be
seen. These findings were also observed in
the dorsum of the upper lobes (not shown).
(b) Day 6, Patient C. Remarkable improve-
ment of the initial findings is obvious. (c)
Day 60 of Patient C. Only equivocal reticular
shadow remains. (d) Day 1, Patient A. Note
bilateral crescent form shadows. The density
of the area is higher than that of water, indi-
cating proteinacious exudate or soft tissue
thickening.
Discussion A, its rate of decrease was quicker than in Patient B, and
so extreme that it might be best comparable with that of a
This accident caused ARS in three patients, who were victim of the Los Alamos accident in 1946 [5] who died
heavily exposed to mixed flux of neutrons and c-rays. ARS 9 days after exposure. In contrast, its decrease in Patient C
develops when a large part of one’s body is exposed to a was relatively mild. Thus the degrees of lymphocyte
high dose of ionizing radiation and has two characteristics. decrease correlated well with the order of severity of ARS
First, its clinical manifestation depends upon the absorbed among the three patients, and was compatible with our
energy of ionizing radiation: with increasing energy, sym- initial reasoning that Patient A had received supralethal
ptoms resulting from the damage to the haematopoietic, dose of radiation. In addition, the predicted doses obtained
gastrointestinal, cardiovascular or central nervous system in the first 24 h relying on the graph by Baranov et al, which
prevail. Second, the syndrome has distinct clinical phases; were more than 10 GyEq, between 6 and 10 GyEq
exposure is followed by the initial prodromal phase with and between 1 and 4.5 GyEq for Patients A, B and C,
nausea and vomiting, followed by the latent phase, during respectively, seemed to be reasonable and were quite
which the patient is asymptomatic, and eventually the valuable.
symptomatic phase. In the literature, the latent phase has The dynamics of WBC also differed significantly among-
been described to be absent in patients who were exposed st the patients (Figure 2a). Although initial leukocytosis,
to more than 8 Gy [9]. However, Patient A, who obviously which reflected granulocytosis, was obvious in all of them,
exceeded this dose, was apparently well for a few days WBC of Patients A and B further increased on the
except for the tenderness on the abdominal wall and diar- morning of day 1, whereas that of Patient C returned to
rhoea, suggesting that the initial evolution of symptoms in normal. In addition, its increase in response to G-CSF was
even a severely irradiated patient may be overcome by only mild in Patients A and B (day 2), while that of
managing the medical condition appropriately. Patient C was quite significant (day 3). In Patients A and
After exposure to ionizing radiation, the severity of B, WBC then decreased rapidly and almost disappeared on
damage to a given organ and the degree of the resultant day 7, whereas in Patient C it was favourably maintained
organ-specific clinical manifestations should be dependent for another 10 days. Although the dynamics of the WBC
upon the absorbed energy of ionizing radiation. Accordingly, count differed between Patients A and B, we have to take
early clinical manifestations of a radiation accident victim into account some conditions. (1) Patient A had been
are quite valuable for predicting the degree of ARS and warned of granulocytosis before the accident, which had
thereby formulating a reasonable therapeutic strategy. not been evaluated as to its exact pathology. His leuko-
Extensive efforts have been made to formulate methods to cytosis after the accident, which was obviously more severe
predict the severity of ARS based on clinical manifestations, than that of the other two, might partly reflect his higher
in particular the dynamics of haematopoietic parameters [8, baseline reservoir of granulocytes. (2) In patient A, the
11, 16], which outweigh other clinical parameters in its ease administration of G-CSF was discontinued on day 2 and
of measuring, sensitivity and quantitativeness. Looking at restarted on day 7, whereas in Patient B it was continued.
the blood counts of the present patients would therefore be The quicker decline of WBC in Patient A on days 3 to 7,
meaningful. The lymphocyte count of Patients A and B compared with that in Patient B in the same period, might
decreased steeply in the first 48 h (Figure 2a). In Patient reflect the lack of G-CSF stimuli. Due to these two
The British Journal of Radiology, April 2003 251
T Hirama, S Tanosaki, S Kandatsu et al
limitations, we would not consider the difference of the of ARS. Hypoxaemia and the CT findings of interstitial
WBC dynamics between Patients A and B significant. oedema of the lungs might make valuable early clinical
Platelets decreased rather slowly when compared with indicators of acute high dose irradiation.
neutrophils or lymphocytes (Figure 2a). However, if we The loss of consciousness in Patient A can be explained
look at the first 7 days, its rate of decline clearly separated as early transient incapacitation (ETI), which has been
the three patients. For instance, platelet count of Patient A observed in animals after whole body exposure to a very
turned below 50 G l21 on day 5, which again was high dose of radiation. According to Franz, ETI in
comparable with case 3 of 1946 Los Alamos accident. In monkeys evolves 3–8 min after a whole body irradiation
Patient B, the platelet count turned below 50 G l21 on day and lasts for 5–20 min [22]. It is associated with a sudden
8, which might be comparable with case V of the 1958 decrease in the cerebral blood flow and systemic hypoten-
Vinca accident [17], who was the most severely irradiated sion [23, 24]. The cause of the symptom has not been
among the six victims in the accident and survived for elucidated, but might reflect the response of the neuro-
1 month. However, in the previous patient, the decrease in vascular system [8] and might be related to a rapid release
lymphocytes and granulocytes were obviously milder than of histamine [25]. MRI of the head of the patients on day 1
those in Patient B. In Patient C the decrease was even did not show any signs of cerebral oedema or focal lesions
milder and fell below 50 G l21 on day 16. In this regard, (data not shown).
this patient might be comparable with case 1 of the 1945 Elevation of serum uric acid has been described in two
Los Alamos accident who died 24 days after irradiation. lethally irradiated victims of the criticality accidents in
Because the use of G-CSF or other growth factors that 1946 and 1958 [3, 5]. Although we do not know the
mobilize myeloid cells is now an important therapeutic mechanisms that underlie this phenomenon, we speculate
option in the treatment of ARS, the platelet count, which that it reflects non-specific and massive cell death caused
is not supposed to be influenced by such reagents, might by high dose irradiation. In addition, increases in serum
make a reliable indicator of the severity of the disease amylase have been encountered after therapeutic irradia-
after several days. Interestingly but quite reasonably, the tion of the head and neck region and planned irradiation
dynamics of reticulocytes in Patient C showed a precisely of the whole body before haematopoietic stem cell trans-
flipped pattern of that of serum iron. It started to recover plantation. The increase in amylase was mainly of salivary
in the second week and exhibited two humps of transient origin, as has been described [26, 27]. As to its degree,
increase before its full recovery in the second month. The Patient B marked the highest level of serum amylase
transient rises of the reticulocyte count are seemingly amongst the three patients on day 1 after the accident,
analogous to those of his neutrophil count, although they followed by Patients A and C. Although the estimated
came several days after those of the neutrophil count. average dose in Patient B was lower than in Patient A, the
They might together represent limited proliferations of head of Patient B might have been very close to the source
damaged progenitor cells in the respective lineages. of radiation (Figure 1). Thus, the extent of the amylase
During the initial period, the three patients exhibited elevation might have roughly reflected the severity of the
hypoxaemia. One explanation for this symptom would be exposure to the head and neck in the three patients. Serum
because ionizing radiation generates a certain amount of uric acid and amylase should be measured in cases of
ozone in the human body, which reportedly transforms suspected exposure to ionizing radiation.
haemoglobin into methaemoglobin in vitro [18]. An
increased level of methaemoglobin in the blood would Conclusion
then decrease PaO2. However, this is not likely to be the
case as studies have shown exposure of intact red cells or Our experience presented in this report is an important
rabbits to ozone did not result in a significant increase of example of applying state of the art therapy and extremely
methaemoglobin [19, 20]. Another explanation would be intensive care to patients of ARS. It confirmed the value of
based on radiation damage to the lungs themselves. the early clinical signs as well as haematologic parameters
Arterial blood gas analyses in the three patients showed for predicting the severity of the disease. We have learned
increased alveolar–arterial gradients of oxygen tension, that, even in a severe form of ARS, the initial hypotensive
suggesting inefficient gas exchange (calculated results not period can be properly managed and that the damage to the
shown). In addition, respiratory function test in Patient haematopoietic system may no longer be the direct cause of
C revealed a transient decrease of the diffusion capacity death. Because a severe form of ARS involves multiple organ
of the lungs. CT of the chest performed on day 1 showed systems, the rescuing of the bone marrow would subse-
interstitial infiltration accompanied by subpleural thicken- quently confront us with the failures of other organ systems
ing in two of them. In Patient C, the hypoxaemia gradually such as the gastrointestinal tract, skin or lungs. Successful
improved, together with the CT findings. These findings treatment of the failures of such organ systems in an ARS
indicate the emergence of interstitial oedema of the lungs patient awaits further progress in the relevant fields at
caused by the damage to the endothelial cells in the organ. the moment and will continue to challenge transplantation
Lung oedema has been observed in a recent fatal criticality medicine in the future. Finally, hypoxaemia and interstitial
accident in Sarov 2 days after exposure [6] and in the Los oedema of the lungs may be considered an early indicator
Alamos accidents in the post-mortem investigation [5]. of ARS, not only in severe cases but also in otherwise
Hypoxaemia shortly after a radiation accident has a asymptomatic cases.
precedent in the Soreq accident in 1990 [21]. However, this
is the first time that the characteristic CT findings of the
Acknowledgments
chest and hypoxaemia in the very early phase of ARS are
described in a patient who has received a non-lethal dose We thank Dr Misao Hachiya for her general support,
of radiation that does not cause any prodromal symptoms and Ms Rika Hara for her secretarial help. We also thank
252 The British Journal of Radiology, April 2003
Tokai-mura criticality accident
Drs Hiroyuki Watanabe, Yoshihiro Yamaguchi, Toru 13. Hayata I, Kanda R, Minamihisamatsu M, Furukawa M,
Iseki and Hideharu Tanaka and Professor Kazuhiko Sasaki MS. Cytogenetical dose estimation for 3 severely
Maekawa for generously providing us with their expertise exposed patients in the JCO criticality accident in Tokai-
in the treatment of the three patients, and the Dose mura. J Radiat Res (Tokyo) 2001;42(Suppl.):S149–55.
14. Ishii T, Futami S, Nishida M, Suzuki T, Sakamoto T,
Estimation Working Group for Three Victims, National
Suzuki N, et al. Brief note and evaluation of acute radiation
Institute of Radiological Sciences for sharing the results of
syndrome and treatment of a Tokai-mura criticality accident
dosimetry. patient. J Radiat Res (Tokyo) 2001;42(Suppl.):S167–82.
15. Nagayama H, Misawa K, Tanaka H, Ooi J, Iseki T, Tojo A,
et al. Transient hematopoietic stem cell rescue using umbilical
References cord blood for a lethally irradiated nuclear accident victim.
Bone Marrow Transplant 2002;29:197–204.
1. Smith DR. Nuclear criticality accidents. Occup Med 16. Andrews GA. Medical management of accidental total-body
1991;6:569–79. irradiation. In: Hubner KF, Fry FA, editors. The medical
2. Vargo GJ. A brief history of nuclear criticality accidents in basis of radiation accident preparedness. Amsterdam, The
Russia—1953-1997. Health Phys 1999;77:505–11. Netherlands and New York, NY: Elsevier, 1980:297–310.
3. Lushbaugh CC. Acute radiation death resulting from an 17. Jammet H, Mathe G, Pendic B, Duplan J-F, Maupin B,
accidental nuclear critical excursion: Clinical course of Case
Latarjet R, et al. Etude de six cas d’irradiation totale aigue
K. J Occup Med 1961;(Suppl.):150–4.
accidentelle. Rev Fr Etudes Clin Biol 1959;4:210–25. [In
4. Karas JS, Stanbury JB. Fatal radiation syndrome from
French.]
an accidental nuclear excursion. N Engl J Med 1965;272:
18. Gonet B. Properties of haemoglobin in ozonized haemoly-
755–61.
sates of erythrocytes. Acta Haematol Pol 1989;20:167–75.
5. Hempelmann LH, Lisco H, Hoffman JG. The acute radiation
19. Freeman BA, Mudd JB. Reaction of ozone with sulfhydryls
syndrome: a study of nine cases and a review of the problem.
of human erythrocytes. Arch Biochem Biophys 1981;208:
Ann Intern Med 1952;36:279–510.
212–20.
6. International Atomic Energy Agency. The criticality accident
20. Ross BK, Hlastala MP, Frank R. Lack of ozone effects on
in Sarov. Vienna, Austria: International Atomic Energy
Agency, 2001. oxygen hemoglobin affinity. Arch Environ Health
7. Muramatsu Y, Noda Y, Yonehara H, Ishigure N, Yoshida S, 1979;38:161–3.
Yukawa M, et al. Determination of radionuclides produced 21. The radiological accident in Soreq. Vienna, Austria:
by neutrons in heavily exposed workers of the JCO criticality International Atomic Energy Agency, 1993.
accident in Tokai-mura for estimating an individual’s neutron 22. Franz CG. Effects of mixed neutron-gamma total-body
fluence. J Radiat Res (Tokyo) 2001;42(Suppl.):S117–28. irradiation on physical activity performance of rhesus
8. Fliedner TM, Friesecke I, Beyrer K, editors. Medical monkeys. Radiat Res 1985;101:434–41.
management of radiation accidents—manual on the acute 23. Cockerham LG, Cerveny TJ, Hampton JD. Postradiation
radiation syndrome. London: British Institute of Radiology, regional cerebral blood flow in primates. Aviat Space Environ
2001. Med 1986;57:578–82.
9. International Atomic Energy Agency. Diagnosis and 24. Cockerham LG, Hampton JD, Doyle TF. Dose dependent
Treatment of Radiation Injuries. Vienna, Austria: radiation-induced hypotension in the canine. Life Sci
International Atomic Energy Agency, 1998. 1986;39:1543–7.
10. Akashi M, Hirama T, Tanosaki S, Kuroiwa N, Nakagawa K, 25. Doyle TF, Curran CR, Turns JE, Strike TA. The prevention
Tsuji H, et al. Initial symptoms of acute radiation syndrome of radiation-induced, early, transient incapacitation of
in the JCO criticality accident in Tokai-mura. J Radiat Res monkeys by an antihistamine. Proc Soc Exp Biol Med
(Tokyo) 2001;42(Suppl.):S157–66. 1974;145:1018–24.
11. Baranov AE, Guskova AK, Nadejina NM, Nugis V. 26. Barrett A, Jacobs A, Kohn J, Raymond J, Powles RL.
Chernobyl experience: biological indicators of exposure to Changes in serum amylase and its isoenzymes after whole
ionizing radiation. Stem Cells 1995;13(Suppl. 1):69–77. body irradiation. BMJ 1982;285:170–1.
12. Ishigure N, Endo A, Yamaguchi Y, Kawachi K. Calculation 27. Junglee D, Katrak A, Mohiuddin J, Blacklock H, Prentice
of the absorbed dose for the overexposed patients at the JCO HG, Dandona P. Salivary amylase and pancreatic enzymes in
criticality accident in Tokai-mura. J Radiat Res (Tokyo) serum after total body irradiation. Clin Chem 1986;32:
2001;42(Suppl.):S137–48. 609–10.
The British Journal of Radiology, April 2003 253
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Textbook of Clinical NeuropsychiatryDocument746 pagesTextbook of Clinical Neuropsychiatrymayamanush100% (1)
- Circuit Pulaski Sixtii Division AL Plaintiffs: in The Court County, ArkansasDocument4 pagesCircuit Pulaski Sixtii Division AL Plaintiffs: in The Court County, ArkansasGAPNo ratings yet
- NOV I 0 2020: Order Dismissing AppealDocument2 pagesNOV I 0 2020: Order Dismissing AppealGAPNo ratings yet
- Pathological Changes in The Gastrointestinal Trect of A Heavily Radiation-Exposed Worker at The Tokai-Mura Criticallity Accident (Igaki 2008)Document8 pagesPathological Changes in The Gastrointestinal Trect of A Heavily Radiation-Exposed Worker at The Tokai-Mura Criticallity Accident (Igaki 2008)GAPNo ratings yet
- The Pathology of Multi-Organ Involvement: Two Autopsy Cases From The Tokai-Mura Criticality Accident (Uozaki 2005)Document4 pagesThe Pathology of Multi-Organ Involvement: Two Autopsy Cases From The Tokai-Mura Criticality Accident (Uozaki 2005)GAPNo ratings yet
- Interview Questions 3Document2 pagesInterview Questions 3api-296922357No ratings yet
- Greer Citizen E-Edition 4.26.17Document16 pagesGreer Citizen E-Edition 4.26.17greercitizenNo ratings yet
- Characterization of Clays and Clay Minerals For Industrial ApplicationsDocument184 pagesCharacterization of Clays and Clay Minerals For Industrial Applicationspam2345100% (1)
- Conclusion in BiologyDocument3 pagesConclusion in Biologyadeza azaresNo ratings yet
- Nucmed 7Document33 pagesNucmed 7John Paul MarasiganNo ratings yet
- Change in Measured GFR Vs EGFR CKD OutcomeDocument9 pagesChange in Measured GFR Vs EGFR CKD OutcomeAlizaPinkyNo ratings yet
- Clinical Practice: History SubtypesDocument6 pagesClinical Practice: History SubtypesRafael Alejandro Marín GuzmánNo ratings yet
- Hirschprung Associated EnterocolitisDocument9 pagesHirschprung Associated Enterocolitiskeyla_shineeeNo ratings yet
- Management of HAZCHEM ProcedureDocument35 pagesManagement of HAZCHEM ProcedurechdprNo ratings yet
- Detailed Neurologic Assessment of Infants and Children - UpToDateDocument25 pagesDetailed Neurologic Assessment of Infants and Children - UpToDateLeoberto Batista Pereira SobrinhoNo ratings yet
- Radiobiology DilshadDocument78 pagesRadiobiology DilshadAJAY K VNo ratings yet
- ANSWER Chapter II-Vocabulary ExerciseDocument4 pagesANSWER Chapter II-Vocabulary Exerciseberliana CahyaNo ratings yet
- Tobacco Harm Reduction 2010Document304 pagesTobacco Harm Reduction 2010Billy HadjisNo ratings yet
- 3 Kuliah GERDDocument40 pages3 Kuliah GERDAnonymous vUEDx8No ratings yet
- Aloe Vera: A Potential Herb and Its Medicinal ImportanceDocument25 pagesAloe Vera: A Potential Herb and Its Medicinal ImportanceSusan Sitha Irma YuhanitaNo ratings yet
- Manual de Procesos Quimicos en La Industria George Austin DescargarDocument15 pagesManual de Procesos Quimicos en La Industria George Austin DescargarAmerica Cardenas OntonNo ratings yet
- Iraqi Injury Surveillance System Annual Report 2013Document46 pagesIraqi Injury Surveillance System Annual Report 2013bejarhasanNo ratings yet
- Block - 3 - 2014 Block 3 BookDocument197 pagesBlock - 3 - 2014 Block 3 BookhappyhappylandNo ratings yet
- Jurnal Vertigo Post TraumaDocument5 pagesJurnal Vertigo Post TraumaginapuspaNo ratings yet
- Cosmecueticals Mod1Document35 pagesCosmecueticals Mod1Top 10No ratings yet
- Don Mariano Marcos Memorial State UniversityDocument6 pagesDon Mariano Marcos Memorial State Universitysoledad l. casillaNo ratings yet
- Elekta Infinity™ BrochureDocument12 pagesElekta Infinity™ BrochureDC ShekharNo ratings yet
- Handbook of RadioembolizationDocument349 pagesHandbook of RadioembolizationEdu MassanaNo ratings yet
- Inpatient Rehab LTLD Referral GuidelinesDocument8 pagesInpatient Rehab LTLD Referral GuidelinesAdi Kurnia SandiNo ratings yet
- Chapter 6 Cancer PrepU QuestionsDocument7 pagesChapter 6 Cancer PrepU QuestionsKevin ClarkNo ratings yet
- TahbsoDocument42 pagesTahbsoMarlon RoyoNo ratings yet
- Vocabulary - Health and Health CareDocument10 pagesVocabulary - Health and Health CareDajana RakićNo ratings yet
- Chemical Dependency EvaluationDocument1 pageChemical Dependency EvaluationBekki JonesNo ratings yet
- High-Performance Medicine: The Convergence of Human and Artificial IntelligenceDocument13 pagesHigh-Performance Medicine: The Convergence of Human and Artificial Intelligencefernandoribeirojr98No ratings yet