
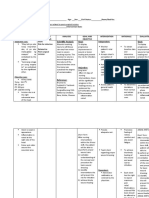
Potential Nursing Care Plan
Potential Nursing Care Plan
You might also like
- Renal Replacement TherapyDocument303 pagesRenal Replacement TherapyPaloma Cruz100% (9)
- Steroid Potency ChartDocument1 pageSteroid Potency ChartKumar Bhai100% (2)
- NURSING CARE PLAN Risk For InfectionDocument3 pagesNURSING CARE PLAN Risk For InfectionEvelyn Lampios100% (1)
- Davao Doctors College General Malvar Street, Davao City Nursing ProgramDocument5 pagesDavao Doctors College General Malvar Street, Davao City Nursing ProgramJhoneric Vencer EscultorNo ratings yet
- NCP-Risk For InfectionDocument2 pagesNCP-Risk For Infectioneihjay-bravo-804175% (81)
- Assesment Diagnosis Inference Objective Intervention Raionale Evaluation Subjective: Objective: Long Term Goal: Goal MetDocument2 pagesAssesment Diagnosis Inference Objective Intervention Raionale Evaluation Subjective: Objective: Long Term Goal: Goal MetChaeL90No ratings yet
- FNCP FinaaaalDocument5 pagesFNCP FinaaaalSoniaMarieBalanay0% (1)
- School Nursing Common DRUG STUDYDocument10 pagesSchool Nursing Common DRUG STUDYMaria Francheska OsiNo ratings yet
- Aspirin Divided PowdersDocument6 pagesAspirin Divided PowdersRaizane Sky Palec100% (1)
- Tuberculosis QsenDocument22 pagesTuberculosis Qsenapi-534410130No ratings yet
- Initial Thesis Report (Global Ayurvedic Village)Document26 pagesInitial Thesis Report (Global Ayurvedic Village)dipu singh82% (11)
- Nursing Care Plan Risk For InjuryDocument1 pageNursing Care Plan Risk For InjuryAce Dioso TubascoNo ratings yet
- NCP .Postoperative.Document5 pagesNCP .Postoperative.Jerome GazmenNo ratings yet
- NCP Risk For InfectionDocument2 pagesNCP Risk For InfectiontermskipopNo ratings yet
- NCP For Ulnar SurgeryDocument5 pagesNCP For Ulnar SurgeryjiloNo ratings yet
- NCP 2Document2 pagesNCP 2Angelica OctotNo ratings yet
- NCP Stab WoundDocument3 pagesNCP Stab WoundjovedNo ratings yet
- Subjective: Objective: Short Term: Independent: Independent: Short TermDocument2 pagesSubjective: Objective: Short Term: Independent: Independent: Short TermJohn Patrick CuencoNo ratings yet
- Nursing Care Plan On Foul-Smelling LochiaDocument3 pagesNursing Care Plan On Foul-Smelling LochiaNE Tdr100% (1)
- Nursing Care Plan: WWW - Unp.edu - PHDocument4 pagesNursing Care Plan: WWW - Unp.edu - PHKrizha Angela Nicolas0% (1)
- NCP Acute AppendicitisDocument2 pagesNCP Acute AppendicitisJane Arian Berzabal100% (1)
- Risk For Infection - NCP 3Document5 pagesRisk For Infection - NCP 3Daphne Cayaba BeltranNo ratings yet
- Assessment Explanation of The Problem Objectives Nursing Interventions Rationale EvaluationDocument3 pagesAssessment Explanation of The Problem Objectives Nursing Interventions Rationale EvaluationAvery LabawigNo ratings yet
- Nursing Care Plan: Lang Ako Tapos Operahan". As Verbalized by The PatientDocument9 pagesNursing Care Plan: Lang Ako Tapos Operahan". As Verbalized by The PatientJoshua KellyNo ratings yet
- NCP AidsDocument4 pagesNCP AidsMelvin D. RamosNo ratings yet
- NCP Risk For InfectionDocument10 pagesNCP Risk For Infectionson hyejooNo ratings yet
- NCP, Ent, Risk For InfectionDocument1 pageNCP, Ent, Risk For InfectionGale DizonNo ratings yet
- كير بلان بالغينDocument3 pagesكير بلان بالغينSima SaeedNo ratings yet
- Assessme NT Diagnosis Planning Intervention Rational E Evaluation Subjectiv E: Short Term: Independent: Short TermDocument2 pagesAssessme NT Diagnosis Planning Intervention Rational E Evaluation Subjectiv E: Short Term: Independent: Short TermPeter Emmil GonzalesNo ratings yet
- Scientific Analysis Goal: Goal:: Subjective CuesDocument2 pagesScientific Analysis Goal: Goal:: Subjective CuesChloie Marie RosalejosNo ratings yet
- NCP 3Document3 pagesNCP 3Grae TaclobNo ratings yet
- Depolonia NCPDocument6 pagesDepolonia NCPMary AllizaNo ratings yet
- NURSING CARE PLAN 2 - Written ReportDocument3 pagesNURSING CARE PLAN 2 - Written ReportAkira PinedaNo ratings yet
- Nursing Care Plan #1 Cues Nursing Diagnosis Objectives Intervention Rationale Evaluation Subjective: Short Term: Independent: Independent Short TermDocument5 pagesNursing Care Plan #1 Cues Nursing Diagnosis Objectives Intervention Rationale Evaluation Subjective: Short Term: Independent: Independent Short TermAlmer OstreaNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective Short Term Independent - Observe Areas Short TermDocument3 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective Short Term Independent - Observe Areas Short TermYkel VidalNo ratings yet
- NCP CASE PRES Potential Risk InfectionDocument2 pagesNCP CASE PRES Potential Risk InfectionKuda Gene LorenNo ratings yet
- B. Surgical ManagementDocument20 pagesB. Surgical ManagementNickaela CalalangNo ratings yet
- NCP 1 - Chicken PoxDocument2 pagesNCP 1 - Chicken Poxphearlie100% (2)
- All NCPsDocument83 pagesAll NCPsDennis Nyambane Momanyi100% (6)
- Diabetes Mellitus Client "Nursing Care Plan": Assesment Nursing Diagnosis Planning Nursing Interventions RationaleDocument11 pagesDiabetes Mellitus Client "Nursing Care Plan": Assesment Nursing Diagnosis Planning Nursing Interventions RationaleKatherine_Chyr_9112No ratings yet
- Nursing Care Plan #3 Assessment Diagnosis Planning Implementation Rationale EvaluationDocument2 pagesNursing Care Plan #3 Assessment Diagnosis Planning Implementation Rationale EvaluationJustine Jean GuillermoNo ratings yet
- Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Inference Planning Intervention Rationale EvaluationLaurel Joshua Reyes DauzNo ratings yet
- NCP Impaired SkinDocument2 pagesNCP Impaired Skinarjay2306_obcq100% (1)
- NCP 1Document2 pagesNCP 1Troy CaballeroNo ratings yet
- NCP 1Document2 pagesNCP 1Troy CaballeroNo ratings yet
- Diabetes Mellitus: Assessment Diagnosis Planning Intervention Rationale EvaluationDocument12 pagesDiabetes Mellitus: Assessment Diagnosis Planning Intervention Rationale EvaluationDerick RanaNo ratings yet
- Student Nurses' Community: NURSING CARE PLAN Neonatal SepsisDocument2 pagesStudent Nurses' Community: NURSING CARE PLAN Neonatal SepsisPanJan BalNo ratings yet
- NCP For Breast CancerDocument2 pagesNCP For Breast Cancergeng gengNo ratings yet
- Nursing Care Plan: Saint Louis University School of Nursing Bonifacio Street, Baguio CityDocument5 pagesNursing Care Plan: Saint Louis University School of Nursing Bonifacio Street, Baguio CitySoniaMarieBalanayNo ratings yet
- CA Risk For Infection NCPDocument2 pagesCA Risk For Infection NCPJheanAlphonsineT.MeansNo ratings yet
- Student Nurses' Community: NURSING CARE PLAN Neonatal SepsisDocument2 pagesStudent Nurses' Community: NURSING CARE PLAN Neonatal SepsisChristian Remetio100% (1)
- NCP Risk For InfectionDocument3 pagesNCP Risk For InfectionAubrey LafuenteNo ratings yet
- NCP Risk of InfectionDocument5 pagesNCP Risk of InfectionPaolo UyNo ratings yet
- Potential Nursing Diagnosis Problem Fdar / NCP: Activity # 2Document2 pagesPotential Nursing Diagnosis Problem Fdar / NCP: Activity # 2Karl KiwisNo ratings yet
- Risk For Infection, CSDocument1 pageRisk For Infection, CSweng_weng040983% (6)
- NCP BULONG BURNDocument6 pagesNCP BULONG BURNBULONG Darlyn GraceNo ratings yet
- Dhan Chan NCPDocument3 pagesDhan Chan NCPDhaneanne Marie ChanNo ratings yet
- UntitledDocument3 pagesUntitledCharlynne AraojoNo ratings yet
- Depolonia NCPDocument6 pagesDepolonia NCPMary AllizaNo ratings yet
- NCP Risk For InfectionDocument2 pagesNCP Risk For InfectionI Am SmilingNo ratings yet
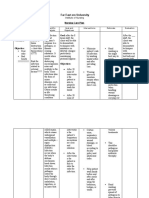
- Far East Ern University: Nursing Care PlanDocument6 pagesFar East Ern University: Nursing Care PlanmharieeeNo ratings yet
- NCP (Revised)Document7 pagesNCP (Revised)Mary AllizaNo ratings yet
- Pulmonary Infection in the Immunocompromised Patient: Strategies for ManagementFrom EverandPulmonary Infection in the Immunocompromised Patient: Strategies for ManagementCarlos AgustiNo ratings yet
- Schematic Pathophy DkaDocument2 pagesSchematic Pathophy DkaMaria Francheska OsiNo ratings yet
- Pathophysiology: SeptumDocument2 pagesPathophysiology: SeptumMaria Francheska OsiNo ratings yet
- Assessment Diagnosis Explanation of The Problem Planning Intervention Rationale Evaluation Subjective: Sto: StoDocument5 pagesAssessment Diagnosis Explanation of The Problem Planning Intervention Rationale Evaluation Subjective: Sto: StoMaria Francheska OsiNo ratings yet
- Respiratory Comp: Nursing DiagnosisDocument1 pageRespiratory Comp: Nursing DiagnosisMaria Francheska OsiNo ratings yet
- CV Disease Drug StudyDocument11 pagesCV Disease Drug StudyMaria Francheska OsiNo ratings yet
- Beta-Adrenergic Blockers: Increased Risk: Tablets: 2.5 MG, 5Document2 pagesBeta-Adrenergic Blockers: Increased Risk: Tablets: 2.5 MG, 5Maria Francheska OsiNo ratings yet
- Injection: 10 MG/ML Oral Solution: 10 Tablets: 20 MG, 40Document4 pagesInjection: 10 MG/ML Oral Solution: 10 Tablets: 20 MG, 40Maria Francheska OsiNo ratings yet
- OB Ward DRUG STUDYDocument1 pageOB Ward DRUG STUDYMaria Francheska OsiNo ratings yet
- Assessment Explanation of The Problem Planning Intervention Rationale EvaluationDocument4 pagesAssessment Explanation of The Problem Planning Intervention Rationale EvaluationMaria Francheska OsiNo ratings yet
- Building Your Immune System: What Is Healthy Eating? What Food Should I Eat?Document3 pagesBuilding Your Immune System: What Is Healthy Eating? What Food Should I Eat?Maria Francheska OsiNo ratings yet
- NCP TemplateDocument2 pagesNCP TemplateMaria Francheska OsiNo ratings yet
- PE NotesDocument1 pagePE NotesMaria Francheska OsiNo ratings yet
- Actual Nursing Care PlanDocument2 pagesActual Nursing Care PlanMaria Francheska OsiNo ratings yet
- 2 Biliary Anatomy and EmbrDocument16 pages2 Biliary Anatomy and EmbrShawn GravesNo ratings yet
- AnecdoteDocument25 pagesAnecdoteWillyAnaNo ratings yet
- Jurnal 1Document497 pagesJurnal 1Tami OvetayNo ratings yet
- The Antibacterial Efficacy of Gotu Kola (Centella Asiatica) - Base SoapDocument11 pagesThe Antibacterial Efficacy of Gotu Kola (Centella Asiatica) - Base SoapJohnnard BelenNo ratings yet
- Review On Swertia Chirata As Traditional Uses To I PDFDocument6 pagesReview On Swertia Chirata As Traditional Uses To I PDFKayal AchuNo ratings yet
- Circular Cghs Referal Expostfacto Approval Delegation 7-4-99Document4 pagesCircular Cghs Referal Expostfacto Approval Delegation 7-4-99Prakash Kapoor50% (2)
- Anabolic PDFDocument21 pagesAnabolic PDFNe MiNo ratings yet
- Lesson Plan (Gene Mutation) DocxDocument3 pagesLesson Plan (Gene Mutation) DocxMae Codium GallentesNo ratings yet
- ABC of AllergiesDocument47 pagesABC of Allergiesdrkis200100% (2)
- CBA 8 MCQ Compilation 2020Document17 pagesCBA 8 MCQ Compilation 2020Sadia YousafNo ratings yet
- GMAT SC Concepts Part 4 Pronouns Sandeep GuptaDocument81 pagesGMAT SC Concepts Part 4 Pronouns Sandeep GuptavirenderNo ratings yet
- Urinary Retentio Ec. Suspect BPH Hernia Scrotalis Dextra: Consultant: Dr. Ninoy Mailoa, SP.B byDocument13 pagesUrinary Retentio Ec. Suspect BPH Hernia Scrotalis Dextra: Consultant: Dr. Ninoy Mailoa, SP.B byCentia PicalNo ratings yet
- Oral Systemic ConnectionDocument37 pagesOral Systemic Connectionchrisdina puspita sari100% (1)
- Vayus GateDocument45 pagesVayus GateRoberta PippiNo ratings yet
- Asif Hanif: Analysis With Chi-SquareDocument14 pagesAsif Hanif: Analysis With Chi-SquareAsad ChaudharyNo ratings yet
- Jandy VS Flopro JEPROMDocument21 pagesJandy VS Flopro JEPROMandyvtranNo ratings yet
- Outcomes of Crowding in Emergency Departments A SyDocument10 pagesOutcomes of Crowding in Emergency Departments A SyPatricio Marcos CasazzaNo ratings yet
- Pain Relief CompressedDocument64 pagesPain Relief Compressedpabulumzeng100% (1)
- Medical Gases CalculationsDocument14 pagesMedical Gases CalculationsNghiaNo ratings yet
- Med AidesDocument17 pagesMed AidesRoseNo ratings yet
- Competency-Based Training in Basic Emergency Obstetric and Newborn Care (BEmONC) Improves Provider's Performance in TanzaniaDocument16 pagesCompetency-Based Training in Basic Emergency Obstetric and Newborn Care (BEmONC) Improves Provider's Performance in TanzaniaJhpiego100% (2)
- ICRC 2014 Healthcare in DetentionDocument100 pagesICRC 2014 Healthcare in DetentionJoseOrlandoRosales100% (1)
- (Only The Ring Finger Knows 5) Satoru Kannagi - Only The Ring Finger Knows Volume 5 - The Finger Never SleepsDocument198 pages(Only The Ring Finger Knows 5) Satoru Kannagi - Only The Ring Finger Knows Volume 5 - The Finger Never Sleepsamu chanNo ratings yet
- Soal PAS B.Ing Kelas 9Document5 pagesSoal PAS B.Ing Kelas 9DidikSakLaekEtohNo ratings yet
- 1416804674Document11 pages1416804674Kenneth MillerNo ratings yet






































































































Download as docx, pdf, or txt
You might also like
- Renal Replacement TherapyDocument303 pagesRenal Replacement TherapyPaloma Cruz100% (9)
- Steroid Potency ChartDocument1 pageSteroid Potency ChartKumar Bhai100% (2)
- NURSING CARE PLAN Risk For InfectionDocument3 pagesNURSING CARE PLAN Risk For InfectionEvelyn Lampios100% (1)
- Davao Doctors College General Malvar Street, Davao City Nursing ProgramDocument5 pagesDavao Doctors College General Malvar Street, Davao City Nursing ProgramJhoneric Vencer EscultorNo ratings yet
- NCP-Risk For InfectionDocument2 pagesNCP-Risk For Infectioneihjay-bravo-804175% (81)
- Assesment Diagnosis Inference Objective Intervention Raionale Evaluation Subjective: Objective: Long Term Goal: Goal MetDocument2 pagesAssesment Diagnosis Inference Objective Intervention Raionale Evaluation Subjective: Objective: Long Term Goal: Goal MetChaeL90No ratings yet
- FNCP FinaaaalDocument5 pagesFNCP FinaaaalSoniaMarieBalanay0% (1)
- School Nursing Common DRUG STUDYDocument10 pagesSchool Nursing Common DRUG STUDYMaria Francheska OsiNo ratings yet
- Aspirin Divided PowdersDocument6 pagesAspirin Divided PowdersRaizane Sky Palec100% (1)
- Tuberculosis QsenDocument22 pagesTuberculosis Qsenapi-534410130No ratings yet
- Initial Thesis Report (Global Ayurvedic Village)Document26 pagesInitial Thesis Report (Global Ayurvedic Village)dipu singh82% (11)
- Nursing Care Plan Risk For InjuryDocument1 pageNursing Care Plan Risk For InjuryAce Dioso TubascoNo ratings yet
- NCP .Postoperative.Document5 pagesNCP .Postoperative.Jerome GazmenNo ratings yet
- NCP Risk For InfectionDocument2 pagesNCP Risk For InfectiontermskipopNo ratings yet
- NCP For Ulnar SurgeryDocument5 pagesNCP For Ulnar SurgeryjiloNo ratings yet
- NCP 2Document2 pagesNCP 2Angelica OctotNo ratings yet
- NCP Stab WoundDocument3 pagesNCP Stab WoundjovedNo ratings yet
- Subjective: Objective: Short Term: Independent: Independent: Short TermDocument2 pagesSubjective: Objective: Short Term: Independent: Independent: Short TermJohn Patrick CuencoNo ratings yet
- Nursing Care Plan On Foul-Smelling LochiaDocument3 pagesNursing Care Plan On Foul-Smelling LochiaNE Tdr100% (1)
- Nursing Care Plan: WWW - Unp.edu - PHDocument4 pagesNursing Care Plan: WWW - Unp.edu - PHKrizha Angela Nicolas0% (1)
- NCP Acute AppendicitisDocument2 pagesNCP Acute AppendicitisJane Arian Berzabal100% (1)
- Risk For Infection - NCP 3Document5 pagesRisk For Infection - NCP 3Daphne Cayaba BeltranNo ratings yet
- Assessment Explanation of The Problem Objectives Nursing Interventions Rationale EvaluationDocument3 pagesAssessment Explanation of The Problem Objectives Nursing Interventions Rationale EvaluationAvery LabawigNo ratings yet
- Nursing Care Plan: Lang Ako Tapos Operahan". As Verbalized by The PatientDocument9 pagesNursing Care Plan: Lang Ako Tapos Operahan". As Verbalized by The PatientJoshua KellyNo ratings yet
- NCP AidsDocument4 pagesNCP AidsMelvin D. RamosNo ratings yet
- NCP Risk For InfectionDocument10 pagesNCP Risk For Infectionson hyejooNo ratings yet
- NCP, Ent, Risk For InfectionDocument1 pageNCP, Ent, Risk For InfectionGale DizonNo ratings yet
- كير بلان بالغينDocument3 pagesكير بلان بالغينSima SaeedNo ratings yet
- Assessme NT Diagnosis Planning Intervention Rational E Evaluation Subjectiv E: Short Term: Independent: Short TermDocument2 pagesAssessme NT Diagnosis Planning Intervention Rational E Evaluation Subjectiv E: Short Term: Independent: Short TermPeter Emmil GonzalesNo ratings yet
- Scientific Analysis Goal: Goal:: Subjective CuesDocument2 pagesScientific Analysis Goal: Goal:: Subjective CuesChloie Marie RosalejosNo ratings yet
- NCP 3Document3 pagesNCP 3Grae TaclobNo ratings yet
- Depolonia NCPDocument6 pagesDepolonia NCPMary AllizaNo ratings yet
- NURSING CARE PLAN 2 - Written ReportDocument3 pagesNURSING CARE PLAN 2 - Written ReportAkira PinedaNo ratings yet
- Nursing Care Plan #1 Cues Nursing Diagnosis Objectives Intervention Rationale Evaluation Subjective: Short Term: Independent: Independent Short TermDocument5 pagesNursing Care Plan #1 Cues Nursing Diagnosis Objectives Intervention Rationale Evaluation Subjective: Short Term: Independent: Independent Short TermAlmer OstreaNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective Short Term Independent - Observe Areas Short TermDocument3 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective Short Term Independent - Observe Areas Short TermYkel VidalNo ratings yet
- NCP CASE PRES Potential Risk InfectionDocument2 pagesNCP CASE PRES Potential Risk InfectionKuda Gene LorenNo ratings yet
- B. Surgical ManagementDocument20 pagesB. Surgical ManagementNickaela CalalangNo ratings yet
- NCP 1 - Chicken PoxDocument2 pagesNCP 1 - Chicken Poxphearlie100% (2)
- All NCPsDocument83 pagesAll NCPsDennis Nyambane Momanyi100% (6)
- Diabetes Mellitus Client "Nursing Care Plan": Assesment Nursing Diagnosis Planning Nursing Interventions RationaleDocument11 pagesDiabetes Mellitus Client "Nursing Care Plan": Assesment Nursing Diagnosis Planning Nursing Interventions RationaleKatherine_Chyr_9112No ratings yet
- Nursing Care Plan #3 Assessment Diagnosis Planning Implementation Rationale EvaluationDocument2 pagesNursing Care Plan #3 Assessment Diagnosis Planning Implementation Rationale EvaluationJustine Jean GuillermoNo ratings yet
- Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Inference Planning Intervention Rationale EvaluationLaurel Joshua Reyes DauzNo ratings yet
- NCP Impaired SkinDocument2 pagesNCP Impaired Skinarjay2306_obcq100% (1)
- NCP 1Document2 pagesNCP 1Troy CaballeroNo ratings yet
- NCP 1Document2 pagesNCP 1Troy CaballeroNo ratings yet
- Diabetes Mellitus: Assessment Diagnosis Planning Intervention Rationale EvaluationDocument12 pagesDiabetes Mellitus: Assessment Diagnosis Planning Intervention Rationale EvaluationDerick RanaNo ratings yet
- Student Nurses' Community: NURSING CARE PLAN Neonatal SepsisDocument2 pagesStudent Nurses' Community: NURSING CARE PLAN Neonatal SepsisPanJan BalNo ratings yet
- NCP For Breast CancerDocument2 pagesNCP For Breast Cancergeng gengNo ratings yet
- Nursing Care Plan: Saint Louis University School of Nursing Bonifacio Street, Baguio CityDocument5 pagesNursing Care Plan: Saint Louis University School of Nursing Bonifacio Street, Baguio CitySoniaMarieBalanayNo ratings yet
- CA Risk For Infection NCPDocument2 pagesCA Risk For Infection NCPJheanAlphonsineT.MeansNo ratings yet
- Student Nurses' Community: NURSING CARE PLAN Neonatal SepsisDocument2 pagesStudent Nurses' Community: NURSING CARE PLAN Neonatal SepsisChristian Remetio100% (1)
- NCP Risk For InfectionDocument3 pagesNCP Risk For InfectionAubrey LafuenteNo ratings yet
- NCP Risk of InfectionDocument5 pagesNCP Risk of InfectionPaolo UyNo ratings yet
- Potential Nursing Diagnosis Problem Fdar / NCP: Activity # 2Document2 pagesPotential Nursing Diagnosis Problem Fdar / NCP: Activity # 2Karl KiwisNo ratings yet
- Risk For Infection, CSDocument1 pageRisk For Infection, CSweng_weng040983% (6)
- NCP BULONG BURNDocument6 pagesNCP BULONG BURNBULONG Darlyn GraceNo ratings yet
- Dhan Chan NCPDocument3 pagesDhan Chan NCPDhaneanne Marie ChanNo ratings yet
- UntitledDocument3 pagesUntitledCharlynne AraojoNo ratings yet
- Depolonia NCPDocument6 pagesDepolonia NCPMary AllizaNo ratings yet
- NCP Risk For InfectionDocument2 pagesNCP Risk For InfectionI Am SmilingNo ratings yet
- Far East Ern University: Nursing Care PlanDocument6 pagesFar East Ern University: Nursing Care PlanmharieeeNo ratings yet
- NCP (Revised)Document7 pagesNCP (Revised)Mary AllizaNo ratings yet
- Pulmonary Infection in the Immunocompromised Patient: Strategies for ManagementFrom EverandPulmonary Infection in the Immunocompromised Patient: Strategies for ManagementCarlos AgustiNo ratings yet
- Schematic Pathophy DkaDocument2 pagesSchematic Pathophy DkaMaria Francheska OsiNo ratings yet
- Pathophysiology: SeptumDocument2 pagesPathophysiology: SeptumMaria Francheska OsiNo ratings yet
- Assessment Diagnosis Explanation of The Problem Planning Intervention Rationale Evaluation Subjective: Sto: StoDocument5 pagesAssessment Diagnosis Explanation of The Problem Planning Intervention Rationale Evaluation Subjective: Sto: StoMaria Francheska OsiNo ratings yet
- Respiratory Comp: Nursing DiagnosisDocument1 pageRespiratory Comp: Nursing DiagnosisMaria Francheska OsiNo ratings yet
- CV Disease Drug StudyDocument11 pagesCV Disease Drug StudyMaria Francheska OsiNo ratings yet
- Beta-Adrenergic Blockers: Increased Risk: Tablets: 2.5 MG, 5Document2 pagesBeta-Adrenergic Blockers: Increased Risk: Tablets: 2.5 MG, 5Maria Francheska OsiNo ratings yet
- Injection: 10 MG/ML Oral Solution: 10 Tablets: 20 MG, 40Document4 pagesInjection: 10 MG/ML Oral Solution: 10 Tablets: 20 MG, 40Maria Francheska OsiNo ratings yet
- OB Ward DRUG STUDYDocument1 pageOB Ward DRUG STUDYMaria Francheska OsiNo ratings yet
- Assessment Explanation of The Problem Planning Intervention Rationale EvaluationDocument4 pagesAssessment Explanation of The Problem Planning Intervention Rationale EvaluationMaria Francheska OsiNo ratings yet
- Building Your Immune System: What Is Healthy Eating? What Food Should I Eat?Document3 pagesBuilding Your Immune System: What Is Healthy Eating? What Food Should I Eat?Maria Francheska OsiNo ratings yet
- NCP TemplateDocument2 pagesNCP TemplateMaria Francheska OsiNo ratings yet
- PE NotesDocument1 pagePE NotesMaria Francheska OsiNo ratings yet
- Actual Nursing Care PlanDocument2 pagesActual Nursing Care PlanMaria Francheska OsiNo ratings yet
- 2 Biliary Anatomy and EmbrDocument16 pages2 Biliary Anatomy and EmbrShawn GravesNo ratings yet
- AnecdoteDocument25 pagesAnecdoteWillyAnaNo ratings yet
- Jurnal 1Document497 pagesJurnal 1Tami OvetayNo ratings yet
- The Antibacterial Efficacy of Gotu Kola (Centella Asiatica) - Base SoapDocument11 pagesThe Antibacterial Efficacy of Gotu Kola (Centella Asiatica) - Base SoapJohnnard BelenNo ratings yet
- Review On Swertia Chirata As Traditional Uses To I PDFDocument6 pagesReview On Swertia Chirata As Traditional Uses To I PDFKayal AchuNo ratings yet
- Circular Cghs Referal Expostfacto Approval Delegation 7-4-99Document4 pagesCircular Cghs Referal Expostfacto Approval Delegation 7-4-99Prakash Kapoor50% (2)
- Anabolic PDFDocument21 pagesAnabolic PDFNe MiNo ratings yet
- Lesson Plan (Gene Mutation) DocxDocument3 pagesLesson Plan (Gene Mutation) DocxMae Codium GallentesNo ratings yet
- ABC of AllergiesDocument47 pagesABC of Allergiesdrkis200100% (2)
- CBA 8 MCQ Compilation 2020Document17 pagesCBA 8 MCQ Compilation 2020Sadia YousafNo ratings yet
- GMAT SC Concepts Part 4 Pronouns Sandeep GuptaDocument81 pagesGMAT SC Concepts Part 4 Pronouns Sandeep GuptavirenderNo ratings yet
- Urinary Retentio Ec. Suspect BPH Hernia Scrotalis Dextra: Consultant: Dr. Ninoy Mailoa, SP.B byDocument13 pagesUrinary Retentio Ec. Suspect BPH Hernia Scrotalis Dextra: Consultant: Dr. Ninoy Mailoa, SP.B byCentia PicalNo ratings yet
- Oral Systemic ConnectionDocument37 pagesOral Systemic Connectionchrisdina puspita sari100% (1)
- Vayus GateDocument45 pagesVayus GateRoberta PippiNo ratings yet
- Asif Hanif: Analysis With Chi-SquareDocument14 pagesAsif Hanif: Analysis With Chi-SquareAsad ChaudharyNo ratings yet
- Jandy VS Flopro JEPROMDocument21 pagesJandy VS Flopro JEPROMandyvtranNo ratings yet
- Outcomes of Crowding in Emergency Departments A SyDocument10 pagesOutcomes of Crowding in Emergency Departments A SyPatricio Marcos CasazzaNo ratings yet
- Pain Relief CompressedDocument64 pagesPain Relief Compressedpabulumzeng100% (1)
- Medical Gases CalculationsDocument14 pagesMedical Gases CalculationsNghiaNo ratings yet
- Med AidesDocument17 pagesMed AidesRoseNo ratings yet
- Competency-Based Training in Basic Emergency Obstetric and Newborn Care (BEmONC) Improves Provider's Performance in TanzaniaDocument16 pagesCompetency-Based Training in Basic Emergency Obstetric and Newborn Care (BEmONC) Improves Provider's Performance in TanzaniaJhpiego100% (2)
- ICRC 2014 Healthcare in DetentionDocument100 pagesICRC 2014 Healthcare in DetentionJoseOrlandoRosales100% (1)
- (Only The Ring Finger Knows 5) Satoru Kannagi - Only The Ring Finger Knows Volume 5 - The Finger Never SleepsDocument198 pages(Only The Ring Finger Knows 5) Satoru Kannagi - Only The Ring Finger Knows Volume 5 - The Finger Never Sleepsamu chanNo ratings yet
- Soal PAS B.Ing Kelas 9Document5 pagesSoal PAS B.Ing Kelas 9DidikSakLaekEtohNo ratings yet
- 1416804674Document11 pages1416804674Kenneth MillerNo ratings yet