Download as pdf or txt
You might also like
- SINGI Solved Papers of ENTDocument430 pagesSINGI Solved Papers of ENTjbtcmdtjjvNo ratings yet
- Eustachian Tube: Structure, Function, and Role in Middle-Ear Disease, 2eFrom EverandEustachian Tube: Structure, Function, and Role in Middle-Ear Disease, 2eNo ratings yet
- IEC 60950 Rev1Document3 pagesIEC 60950 Rev1Rip_BarNo ratings yet
- Lecture On: Objective Structured Practical Examination (OSPE) in ENTDocument34 pagesLecture On: Objective Structured Practical Examination (OSPE) in ENTEdward Smith100% (1)
- Ent Lecture NotesDocument2 pagesEnt Lecture NotesThistell ThistleNo ratings yet
- Practical View of ENTDocument31 pagesPractical View of ENTAbouzr Mohammed ElsaidNo ratings yet
- Otolaryngology Mcqs & SBAs 2nd EditionDocument6 pagesOtolaryngology Mcqs & SBAs 2nd EditionJohn M. Hemsworth100% (1)
- Hydraulic Axial Piston Eaton Vickers PVB Pump: - Basic CharacteristicsDocument13 pagesHydraulic Axial Piston Eaton Vickers PVB Pump: - Basic Characteristicsjose alberto olvera gomezNo ratings yet
- Carbon Footprint of Organic FertilizerDocument5 pagesCarbon Footprint of Organic FertilizerSteve Savage100% (6)
- ENT OSCE (Girls 1428-29)Document9 pagesENT OSCE (Girls 1428-29)Maria Monica De CastroNo ratings yet
- DOHNS Part II OSCE Glasgow May 2013Document4 pagesDOHNS Part II OSCE Glasgow May 2013rizwan afzal100% (2)
- Ent VivaDocument3 pagesEnt VivayamnaNo ratings yet
- ENT Short Cases Records & OSCE Questions: 1 EditionDocument15 pagesENT Short Cases Records & OSCE Questions: 1 EditionSaya MenangNo ratings yet
- Ent SpottersDocument18 pagesEnt SpottersJithin Gopal100% (1)
- Thyroglossal Duct Cysts, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandThyroglossal Duct Cysts, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Neck Lumps, (Cervical Masses) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandNeck Lumps, (Cervical Masses) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- E.N.T Guide For Medical Students: Neck Examination: Dr. Giovanni Henry ENT Resident 2016Document79 pagesE.N.T Guide For Medical Students: Neck Examination: Dr. Giovanni Henry ENT Resident 2016John M. HemsworthNo ratings yet
- Ent Ospe Badhahin v1 7 PDFDocument26 pagesEnt Ospe Badhahin v1 7 PDFWasi OsmanNo ratings yet
- Ent Past Years Question According To TopicsDocument32 pagesEnt Past Years Question According To Topicsmohamed100% (1)
- ENT AyaSalahEldeenDocument147 pagesENT AyaSalahEldeenFatma ShnewraNo ratings yet
- Osce - Nose & PnsDocument19 pagesOsce - Nose & Pnsaakash maanNo ratings yet
- ENT OSPE (Batch 2) - 1Document11 pagesENT OSPE (Batch 2) - 1Mahnoor khanNo ratings yet
- Tonsillectomy Slides 050427Document62 pagesTonsillectomy Slides 050427Aidiel FikriNo ratings yet
- Post Graduate Degree Standard Paper - I CodeDocument7 pagesPost Graduate Degree Standard Paper - I CodeFZ icebladeNo ratings yet
- Otolaryngology PDA Toronto NotesDocument29 pagesOtolaryngology PDA Toronto NotesNor Aimi Abd Rahman100% (1)
- 4 Dohns May 2004Document7 pages4 Dohns May 2004rizwan afzalNo ratings yet
- Ent Osce 2008Document22 pagesEnt Osce 2008salamred100% (2)
- Otorhinolaryngology (ENT) Syllabus of ENT 4 and 6 Semester EARDocument10 pagesOtorhinolaryngology (ENT) Syllabus of ENT 4 and 6 Semester EARShubhashish SinghathakurNo ratings yet
- Ears, Nose and Throat Diseases: Prepared By: Hannelli BelingonDocument103 pagesEars, Nose and Throat Diseases: Prepared By: Hannelli BelingonPatricia Kamille I. PawidNo ratings yet
- ENTDocument8 pagesENTapi-19863548No ratings yet
- Ent Case 2Document29 pagesEnt Case 2Trina CardonaNo ratings yet
- 02a MRCS ENT RegulationsDocument3 pages02a MRCS ENT RegulationsAravind NooneyNo ratings yet
- Otorhinolaryngology PDFDocument19 pagesOtorhinolaryngology PDFالطالب الطبيبNo ratings yet
- Concept Book Ent Working FileDocument801 pagesConcept Book Ent Working FileDrAssadullah HamzaNo ratings yet
- Paediatric OtorhinolaryngologyDocument37 pagesPaediatric OtorhinolaryngologySana BushraNo ratings yet
- Chhabhadiya Laxman (Ent)Document7 pagesChhabhadiya Laxman (Ent)Venkatesh GarikapatiNo ratings yet
- ENT EmergencyDocument57 pagesENT EmergencykylieverNo ratings yet
- Ent Imp Points To Diagnose ScenariosDocument46 pagesEnt Imp Points To Diagnose Scenariosusmandumassar0% (1)
- Clinicals ENTDocument70 pagesClinicals ENTMarrow Pg42No ratings yet
- Branchial Cleft CystsDocument8 pagesBranchial Cleft CystsHere LeafsNo ratings yet
- Ear, Nose, and Throat EmergenciesDocument23 pagesEar, Nose, and Throat EmergenciesRajesh SharmaNo ratings yet
- Ear, Nose and Throat EmergenciesDocument3 pagesEar, Nose and Throat Emergenciesfmta100% (1)
- ENT Lecture NotesDocument190 pagesENT Lecture NotesMizrab NadeemNo ratings yet
- Otitis MediaDocument67 pagesOtitis MediaFurqan MirzaNo ratings yet
- Candidate Instructions and Guidance NotesDocument5 pagesCandidate Instructions and Guidance NotesShaun DaveyNo ratings yet
- Ent NotesDocument3 pagesEnt Notesapi-26186766No ratings yet
- Cholesteatoma Part 5 Congenital Cholesteatoma PDFDocument4 pagesCholesteatoma Part 5 Congenital Cholesteatoma PDFSuprit Sn100% (1)
- Basic Sinus AnatomyDocument71 pagesBasic Sinus AnatomyTalal AlanzyNo ratings yet
- Ear, Nose and Throat emerg-ENT-cies: With Laura WilkinsDocument43 pagesEar, Nose and Throat emerg-ENT-cies: With Laura WilkinsIrina AndreeaNo ratings yet
- Utmb-Glomus Tumors of The Temporal BoneDocument11 pagesUtmb-Glomus Tumors of The Temporal BoneAnoop SinghNo ratings yet
- ENT Clinical Skill: Dr. Pulo R S Banjarnahor, SP THT-KL Dr. Reno H Kelan, SP - THT-KLDocument80 pagesENT Clinical Skill: Dr. Pulo R S Banjarnahor, SP THT-KL Dr. Reno H Kelan, SP - THT-KLDavidVictoriousLukasNo ratings yet
- ورق مذاكره PDFDocument100 pagesورق مذاكره PDFsalamred100% (1)
- Mbbs Feb11Document22 pagesMbbs Feb11Dr. T. Balasubramanian100% (2)
- Acute Suppurative Otitis MediaDocument19 pagesAcute Suppurative Otitis MediaRajesh Sharma100% (1)
- Basic Physical Examination in ENTDocument44 pagesBasic Physical Examination in ENTKIWANUKA GEORGE100% (1)
- Otorhinolaryngology 10 YearsDocument4 pagesOtorhinolaryngology 10 YearsSarbashis HazraNo ratings yet
- 2012 ENT OSCE QuestionsDocument4 pages2012 ENT OSCE QuestionsFaiq Syukri Bin Saparudin50% (2)
- Ent OsceDocument42 pagesEnt OsceAkash GuptaNo ratings yet
- OSCE Notes in Otology Surgery by DrtbaluDocument85 pagesOSCE Notes in Otology Surgery by DrtbaluDrAli JafarNo ratings yet
- Final Written ENT With CoverDocument231 pagesFinal Written ENT With CoverAlyAl-MakhzangyNo ratings yet
- Ent PapersDocument17 pagesEnt PapersPNo ratings yet
- Consultant in Audiology: Passbooks Study GuideFrom EverandConsultant in Audiology: Passbooks Study GuideNo ratings yet
- Epistaxis (Nose Bleed), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandEpistaxis (Nose Bleed), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Scanned by CamscannerDocument46 pagesScanned by CamscannerMuhammad IbrahimNo ratings yet
- Scottish Health Survey 2003/4 Booklet For 8-12 Year Olds: in ConfidenceDocument6 pagesScottish Health Survey 2003/4 Booklet For 8-12 Year Olds: in ConfidenceMuhammad IbrahimNo ratings yet
- Case PresentationDocument25 pagesCase PresentationMuhammad IbrahimNo ratings yet
- Code of ConductDocument1 pageCode of ConductMuhammad IbrahimNo ratings yet
- Psoas AbscessDocument3 pagesPsoas AbscessMuhammad IbrahimNo ratings yet
- Past Papers King Edward Medical UniversityDocument14 pagesPast Papers King Edward Medical UniversityMuhammad IbrahimNo ratings yet
- Physical Education IV: (Recreation)Document28 pagesPhysical Education IV: (Recreation)Faye Corazon GaurinoNo ratings yet
- Model ETR-9200 Automatic Tuning Smarter Logic ControllerDocument26 pagesModel ETR-9200 Automatic Tuning Smarter Logic ControllervhelectronicaNo ratings yet
- Training - Cga ApplicationDocument34 pagesTraining - Cga ApplicationSubhan Muhammad100% (1)
- Duolingo Word ListDocument30 pagesDuolingo Word ListSabira AlizadaNo ratings yet
- Analysis On Explanation TextDocument2 pagesAnalysis On Explanation Textasih dwi astutiNo ratings yet
- Msds-Of M 220-Eng - 43-29357Document13 pagesMsds-Of M 220-Eng - 43-29357Lennier SaezNo ratings yet
- Microbiology 101: Laboratory Exercise #22: Carbohydrate MetabolismDocument16 pagesMicrobiology 101: Laboratory Exercise #22: Carbohydrate Metabolismmaraki998No ratings yet
- Mina NEGRA HUANUSHA 2 ParteDocument23 pagesMina NEGRA HUANUSHA 2 ParteRoberto VillegasNo ratings yet
- Wear Solutions BrochureDocument16 pagesWear Solutions BrochureOkan KalendarNo ratings yet
- Like Water For Chocolate QuestionsDocument2 pagesLike Water For Chocolate Questionslde918No ratings yet
- Laboratory Information Management System: Prepared By: Mariela C. Ronquillo, RMTDocument33 pagesLaboratory Information Management System: Prepared By: Mariela C. Ronquillo, RMTRonel RonquilloNo ratings yet
- Analise de Agua e EfluentesDocument28 pagesAnalise de Agua e EfluentesFabiano Luiz NavesNo ratings yet
- SRHR - FGD With Young PeopleDocument3 pagesSRHR - FGD With Young PeopleMandira PrakashNo ratings yet
- Welding Procedure Specification Joint Venture: Azzawiya Control System Modernization ProjectDocument4 pagesWelding Procedure Specification Joint Venture: Azzawiya Control System Modernization ProjectwentropremNo ratings yet
- Environmental Geotechniques: Theories of Ion ExchangeDocument21 pagesEnvironmental Geotechniques: Theories of Ion ExchangeTenkurala srujanaNo ratings yet
- Basic Symbals P&ID PDFDocument736 pagesBasic Symbals P&ID PDFPavar RavitejaNo ratings yet
- Cognitive Chapter 6 Cornell NotesDocument10 pagesCognitive Chapter 6 Cornell Notesvalcobacl.681.studNo ratings yet
- 1 Case IDC PDFDocument7 pages1 Case IDC PDFPilar Dueñas Maldonado0% (1)
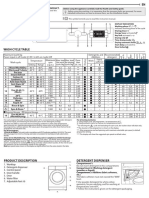
- Whirlpool BIWDWG861484uk enDocument4 pagesWhirlpool BIWDWG861484uk ennadaljoachim77No ratings yet
- Generator Automatic Voltage Regulator Operation ManualDocument6 pagesGenerator Automatic Voltage Regulator Operation ManualMahdi DehghankarNo ratings yet
- Weekly Report ExampleDocument3 pagesWeekly Report Examplewawan setiawanNo ratings yet
- b4 EngDocument2 pagesb4 EngAdrian LopezNo ratings yet
- Gujarat Cancer and Research Institute RatesDocument33 pagesGujarat Cancer and Research Institute RatesNimhans HospitalNo ratings yet
- Dan Sof TG 0122Document30 pagesDan Sof TG 0122Erick Trujillo100% (1)
- Towncall Rural Bank, Inc.: To Adjust Retirement Fund Based On Retirement Benefit Obligation BalanceDocument1 pageTowncall Rural Bank, Inc.: To Adjust Retirement Fund Based On Retirement Benefit Obligation BalanceJudith CastroNo ratings yet
- Lecture 6Document32 pagesLecture 6Nilesh PanchalNo ratings yet
- Critikon Dinamap MPS - Product Description PDFDocument9 pagesCritikon Dinamap MPS - Product Description PDFJulio Benancio ZuluagaNo ratings yet